
Abstract
Background
Instability of the sternoclavicular joint (SCJ) is a rare problem that is often treated closed, with few published outcomes of surgical treatment with tendon graft reconstruction.
Methods
We reviewed a consecutive series of patients who underwent tendon graft reconstruction for SCJ instability over a 7-year period. Cases with acute fractures or fewer than 2 years of follow-up were excluded. Pre- and postoperative function and pain were assessed using Single assessment numeric evaluation (SANE), simple shoulder test (SST), and visual analog scale (VAS) outcome measures.
Results
Thirty cases were included, with 27 (90%) available for follow-up at a minimum of 2 years postoperatively. SANE scores improved from a median of 40 to 90. SST scores improved from a median of 3 positive responses to a median of 12 on a 12-point scale. VAS scores decreased from a median of 7 to 0 points. One patient underwent reoperation for recurrent instability and wound dehiscence. Three (11%) patients did not achieve a minimum 30% of maximum possible improvement in SST scores.
Conclusions
Tendon graft reconstruction for SCJ instability is a safe procedure with a low complication rate and statistically and clinically significant improvements in patient-reported outcome measures at 2-year minimum follow-up.
Level of evidence
Level IV: Therapeutic.
Introduction
Dislocations of the sternoclavicular joint (SCJ) are a rare injury, often associated with high-energy direct trauma to the chest. 1 The majority of these injuries can be treated with closed reduction in the operating room. 2 A small minority of injuries remain chronically unstable, resulting in limitations of functional activities. Due to the proximity of the SCJ to mediastinal structures, posterior instability of the SCJ can also result in difficulty with swallowing and breathing and can cause vascular compromise. 1
Surgical treatment has been recommended in cases where closed reduction does not result in satisfactory stability of the SCJ, but there have been few published data regarding clinical outcomes after reconstruction of the unstable SCJ in skeletally mature patients. 3 Historical techniques for reconstructing the SCJ have included local soft-tissue repair, reconstruction with synthetic material, open reduction and internal fixation with screws and/or plates, medial clavicular resection with or without ligament repair, and tendon transfers. 4 Tendon graft reconstruction of the unstable SCJ has gained popularity in recent years as a result of the biomechanical stability provided by a figure-of-eight configuration. 5 Several case series from the past decade have shown good clinical outcomes with a low complication rate.4–13 The purpose of this study was to review a consecutive series of tendon graft reconstructions for traumatic SCJ instability and report minimum 2-year objective and patient-reported outcomes. We hypothesized that this technique would result in clinical improvement and stability at a minimum of 2 years after surgery. Our null hypothesis was that patients would not have durable stability and clinical improvement would be less than the minimum clinically important difference. We also describe a reproducible surgical reconstruction algorithm that provides maximum safety and protection of mediastinal structures.
Methods
Study population
Institutional Review Board approval (IRB# STUDY00008239) was granted for a retrospective review of a longitudinal, prospectively compiled outcomes database. A consecutive series of patients who underwent tendon graft reconstruction for SCJ instability by a single surgeon from August 2009 to March 2016 were eligible for inclusion. Patients routinely underwent computerized tomography (CT) scan of the bilateral SCJs preoperatively. Cases with associated acute fracture or SCJ stabilization without use of a tendon graft were excluded. Patients were indicated for surgery if they had symptomatic instability with failure of conservative treatment. Symptomatic instability was defined on the basis of a systematic clinical examination including supine axial loading of the SCJ. All relevant study information has been reported according to STROBE (strengthening the reporting of observational studies in epidemiology) guidelines. 14
Surgical technique
A thoracic surgeon is immediately available for every surgery to address serious bleeding if encountered. Any necessary instruments as determined by the thoracic surgeon should be available in the room prior to the start of the procedure.
Surgery is performed in a supine position (Figure 1). To allow the shoulders to be manipulated freely, no pillow or other positioning device is placed between the scapulae. The entire thorax is draped from the neck to the umbilicus, including bilateral acromioclavicular joints. A necklace-type incision is made along Langer's lines across the SCJ (Figure 2). The 2 heads of the sternocleidomastoid (SCM) muscle and the sternal notch are identified. A fresh knife is used to incise the sternoclavicular capsule sharply, and the medial clavicle is exposed (Figure 3). A minimal debridement is performed if osteophytes have developed secondary to chronic instability. Substantial resection of the medial clavicle greater than 5 mm should be avoided to prevent late instability. 5
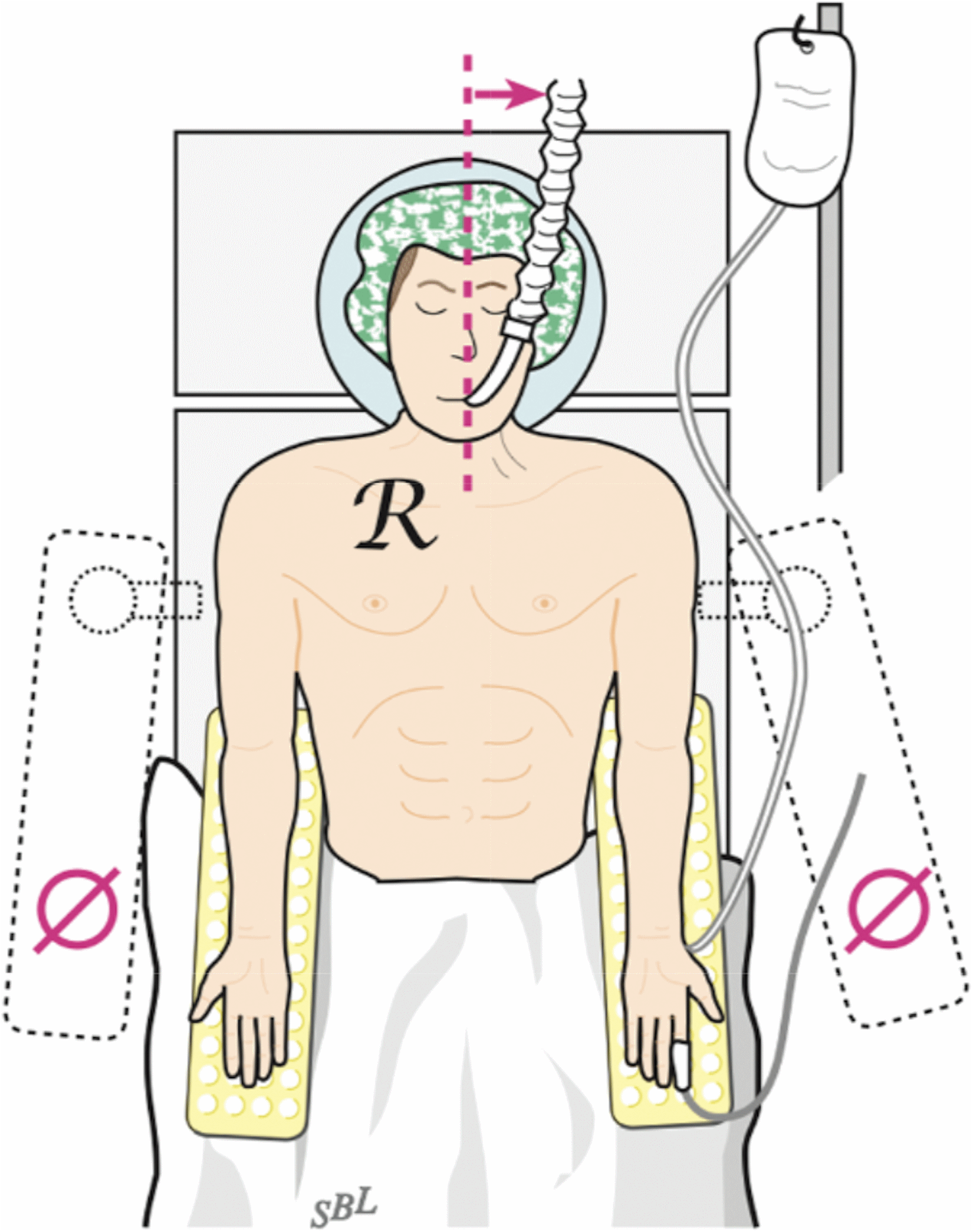
Positioning for sternoclavicular reconstruction. (From Warme WJ, Bois AJ, Somerson JS. Open management of atraumatic disorders of the sternoclavicular joint: indications, techniques, outcomes, and complications. In: Matsen FA, Cordasco FA, Sperling JW, editors. Rockwood and Matsen's The Shoulder. 6th ed. Philadelphia: Elsevier.)
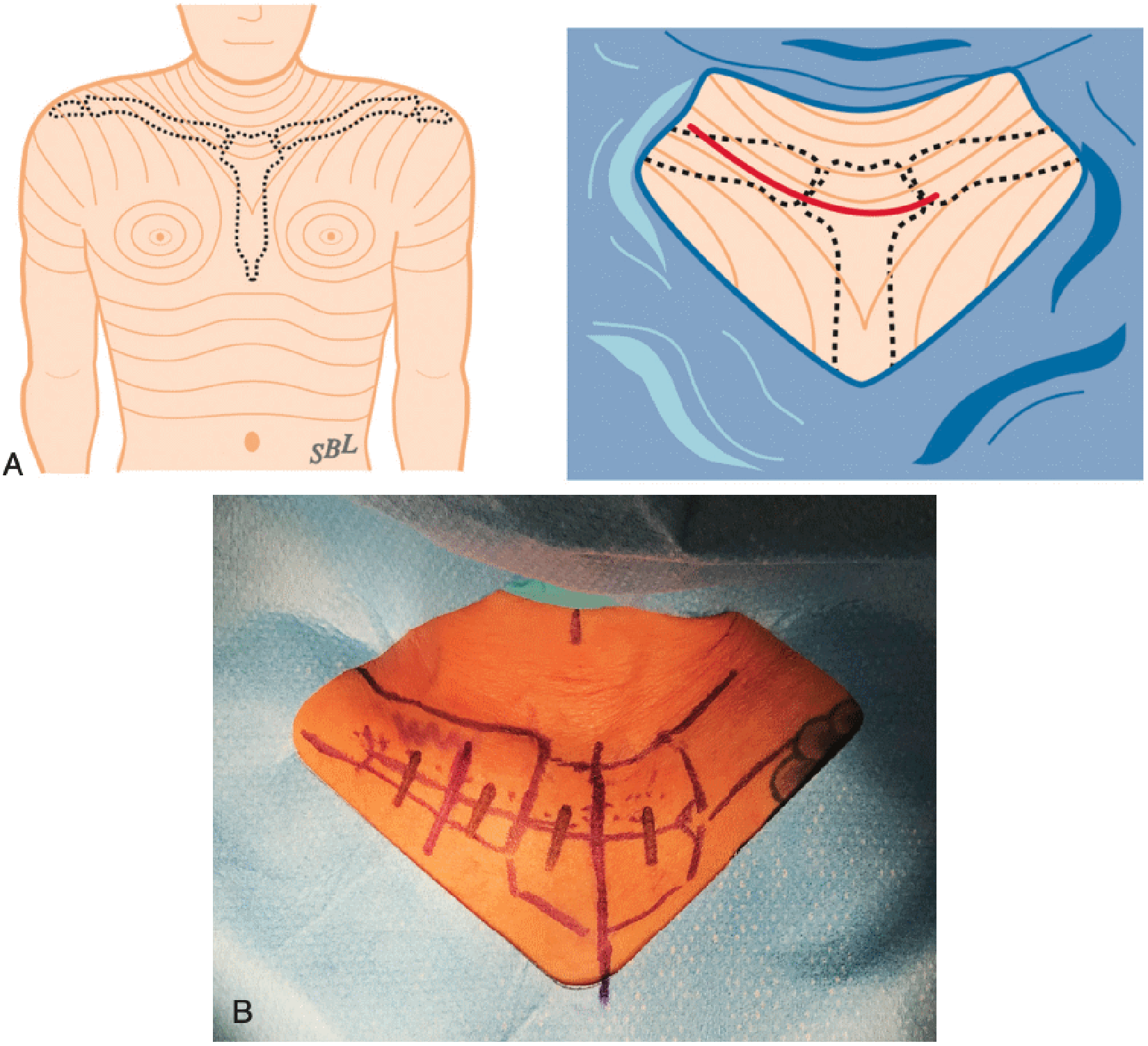
A necklace incision along langer's lines provides for cosmetic healing. (A) Location of Langer's lines, (B) markings for incision site. (From Warme WJ, Bois AJ, Somerson JS. Open management of atraumatic disorders of the sternoclavicular joint: Indications, techniques, outcomes, and complications. In: Matsen FA, Cordasco FA, Sperling JW, editors. Rockwood and Matsen's The Shoulder. 6th ed. Philadelphia: Elsevier.)
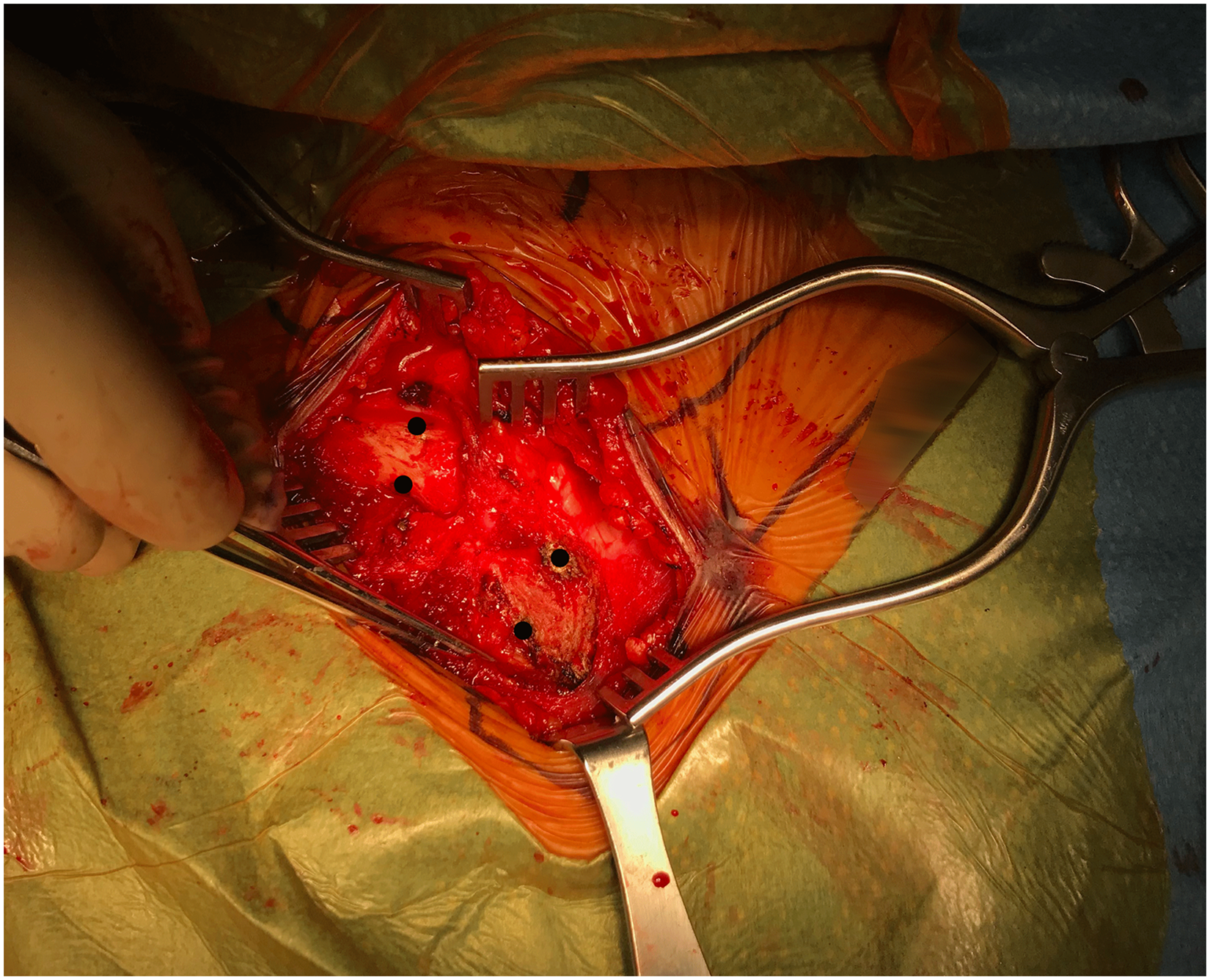
Tunnel sites for sternoclavicular joint reconstruction at the clavicle and sternum.
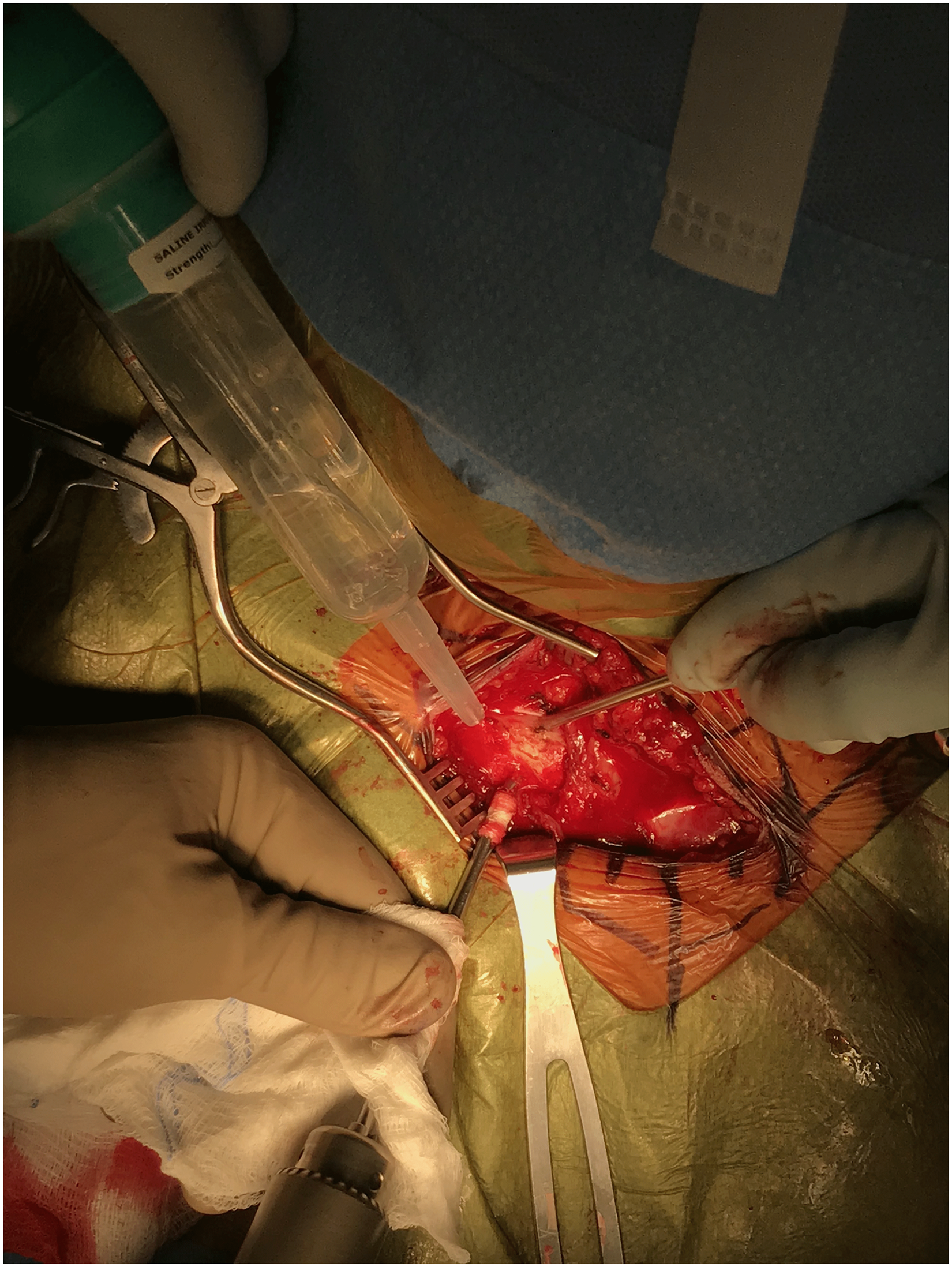
For cases of anterior instability, 2 unicortical tunnels are marked and prepared with the 4.5 drill in the medial clavicle and in the manubrium (Figure 4). A small sterile adhesive bandage strip can be wrapped around the drill to mark the desired tunnel depth (Figure 5). The tunnels are connected with right-angle clamps, and the graft (semitendinosus allograft, prepared prior to SCJ incision and prepared with 2 size 0 looped nonabsorbable sutures) is shuttled through the tunnels with a Hewson suture passer, placing 2 parallel arms anteriorly (Figure 6). With the graft in the tunnels, it is demonstrated that the appropriate amount of tension and stability can be returned to the joint when tightened (Figure 7). The graft is loosened to allow for a capsulorraphy to be performed with 2-0 nonabsorbable sutures in a figure-of-eight fashion, which greatly stabilizes the joint on its own. The graft is then secured as previously mentioned and oversewn with 2-0 nonabsorbable sutures until it is robustly fixed (Figure 8). Once the graft is snug, the joint is examined once again for clavicular stability.
Unicortical tunnels are created for cases of anterior sternoclavicular instability.

Drill depth can be marked with an adhesive tape.
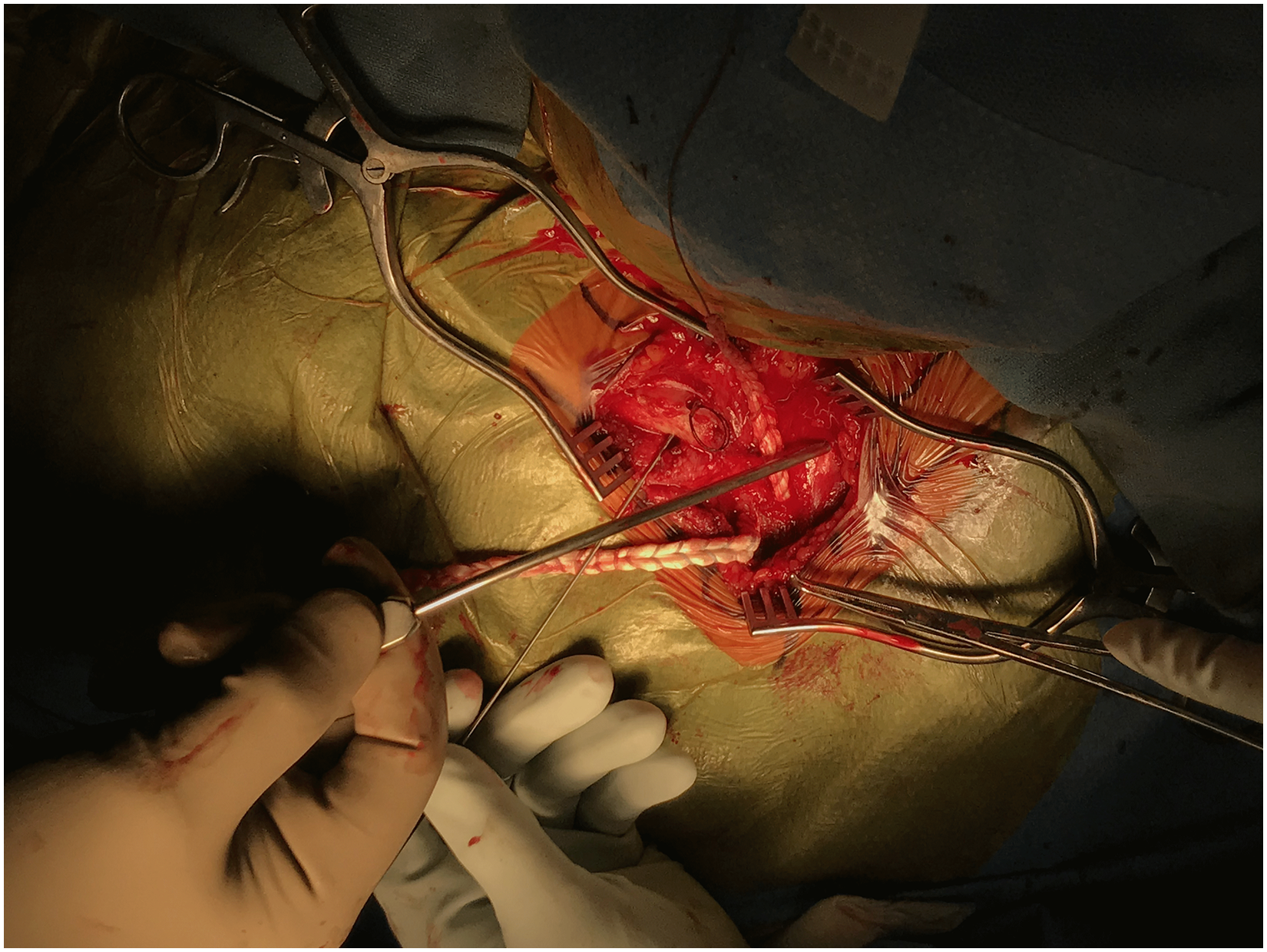
The tendon graft is passed through the unicortical tunnels.
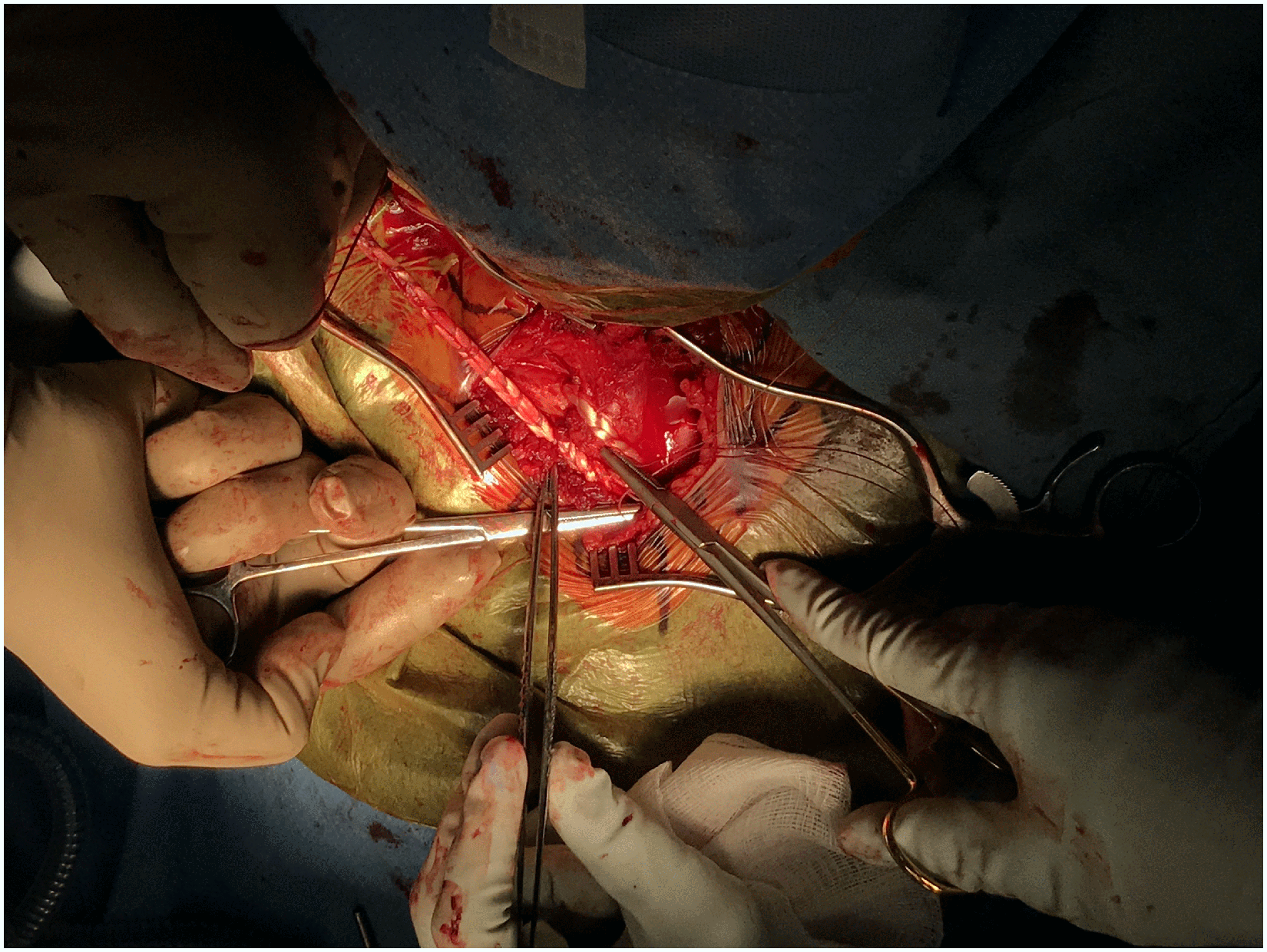
Graft configuration for anterior sternoclavicular instability.
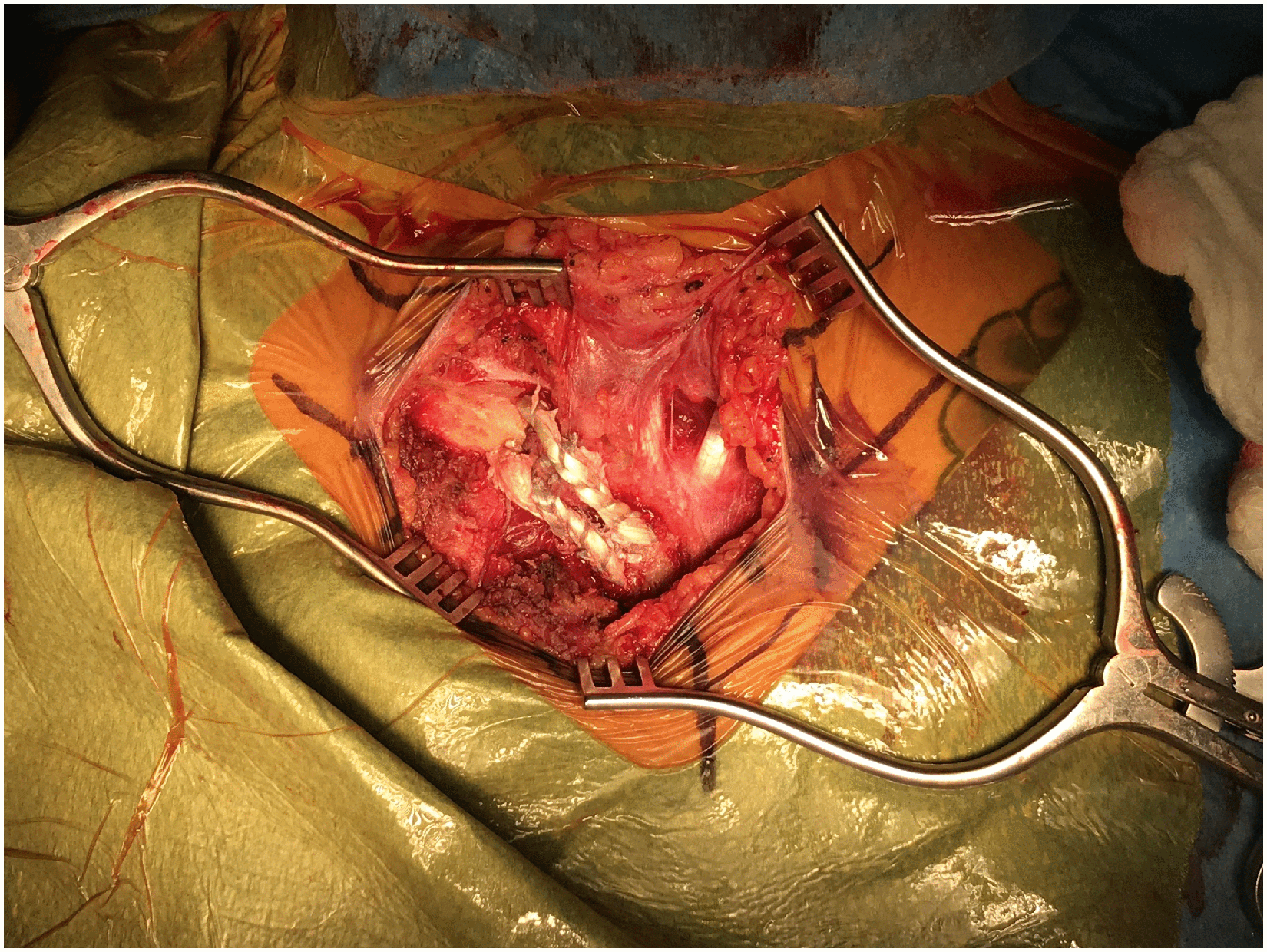
Final graft position after suture fixation.
For posterior instability, special equipment includes a posterior cruciate ligament (PCL) tunnel-aiming system to ensure added safety for tunnel placement, an 18-gauge wire to create smooth passing loops, and a 2-0 nonabsorbable suture for capsular repair. 7 An allograft semitendinosus tendon is used in most cases, unless the patient has a preference for autologous tissue. After exposing the SCJ, a vertical incision is then made at the sternal notch between the sternothyroid muscles similar to the starting incision made for mediastinoscopy. Blunt-finger dissection is performed posterior to the sternum and clavicle. It is important that the posterior aspects of the SCJ and medial clavicle are free of soft-tissue attachments. Two bicortical tunnels are then placed through the medial clavicle and sternum for graft passage. Care should be taken to ensure an adequate bone bridge of at least 1 cm between the tunnels to prevent fracture. A PCL tibial-aiming guide is carefully placed behind the medial clavicle. A safety stop is attached to the drill guide at the measured length, and a guide wire is drilled just through the posterior cortex of the clavicle. The PCL-aiming guide and guide wire are removed. The blunt end of the guide wire is then inserted through the drilled hole and captured in a blunt-tipped elevator. A tunnel can then be reamed over the guide wire to the desired diameter; this is based on the measured graft width and is typically 4 mm. Power reaming is used until the posterior cortex is reached. After the cortex is reached, the tunnel can be completed by hand reaming. A finger can be placed directly onto the posterior cortex of the clavicle during this step for added safety. This process is repeated at the clavicle and at the sternum twice, resulting in 4 parallel tunnels. Smooth, curved loops for suture passage are created using doubled segments of 18-gauge wire. The curve of the wire loops is fashioned so that the loop can safely pass through the tunnels out the sternal notch incision. The field is irrigated to allow for easier graft passage, and the graft is pulled through the tunnels in a figure-of-eight configuration. The parallel limbs of the figure-of-eight graft are positioned at the posterior aspect of the SCJ, and the limbs are crossed at the anterior aspect of the joint.
After graft passage, the SCJ capsulotomy is repaired using 2-0 nonabsorbable suture, with the joint held in a reduced position by medial pressure on the ipsilateral shoulder. The graft is then held taut, and the crossing ends of the graft are sutured to one another anteriorly with horizontal mattress 2-0 nonabsorbable sutures. The sutures should be aligned obliquely to the graft's line of pull to ensure that there is no loss of tension once the shoulder is no longer supported. If the sternal head of the SCM was detached, it should be repaired anatomically to ensure that there is no alteration of cosmesis or neck discomfort.
Postoperative course
A shoulder immobilizer is placed at the conclusion of surgery. The patient should perform only hand, wrist, and elbow active range of motion (AROM) for the first 2 weeks. From 2 to 6 weeks, supine active-assisted range of motion is initiated with a limit of 90 degrees forward elevation. The sling is discontinued at 6 weeks, but horizontal abduction past neutral is still restricted. From 6 to 9 weeks, AROM is advanced to a goal of 120 degrees of forward elevation and 90 degrees of abduction. Full AROM is targeted for 12 weeks. Light resistance weight training may be initiated at 3 to 4 months postoperatively, and gradual resumption of prior activities is expected from 4 to 6 months after surgery.
Data collection
The following patient-reported outcome scores were collected preoperatively and at latest follow-up: single assessment numeric evaluation (SANE), simple shoulder Test (SST), and visual analog scale (VAS) for pain. The Rockwood SCJ score 15 was calculated on the basis of reported limitations in strength, range of motion and work, VAS pain score, and SANE subjective outcome score. Patients were also asked about any complications or reoperations they had experienced, whether they had any residual limitations with regard to activities of daily living or sports, and whether they would recommend the procedure to others.
Statistical analysis
Statistical analyses were performed using JMP version 9 (SAS Institute, Cary, NC). Paired t tests were used for comparison from preoperative to postoperative matched pairs. A P value of <.05 was defined as statistically significant.
Results
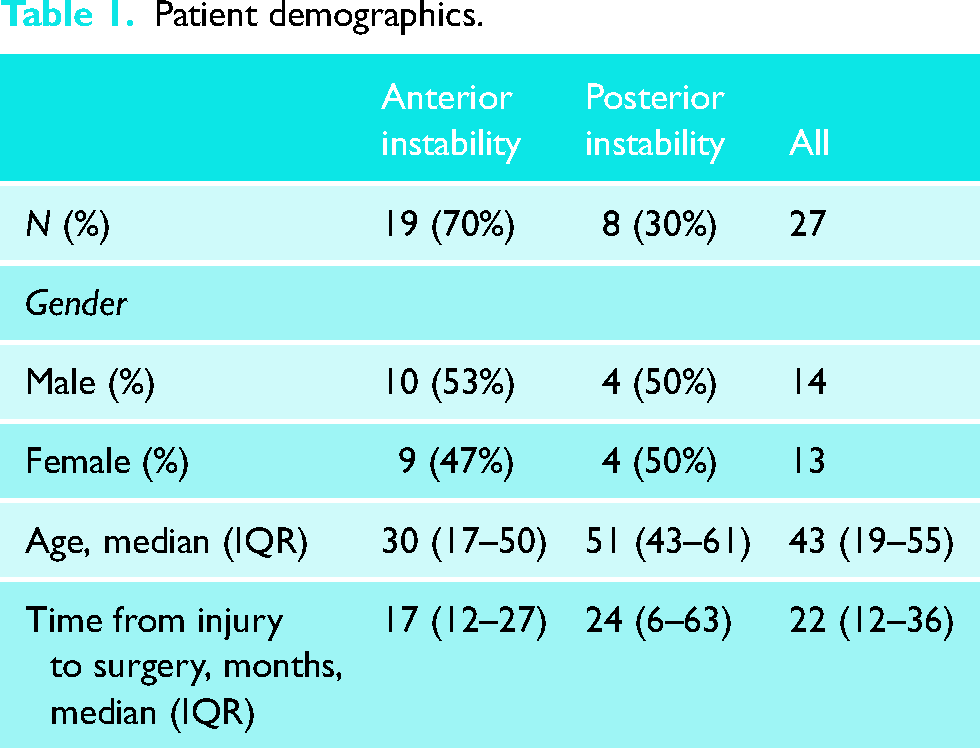
During the retrospective study period, the senior author performed 30 cases of primary SCJ reconstruction using a tendon graft. Of these, 21 procedures were for anterior instability and 9 were for posterior instability. At a minimum of 2 years after surgery, 27 of the 30 cases (90%) were available for follow-up with patient-reported outcomes (median follow-up, 3 years; range, 2–7 years). Patient demographics are reported in Table 1.
Patient demographics.
Outcomes.
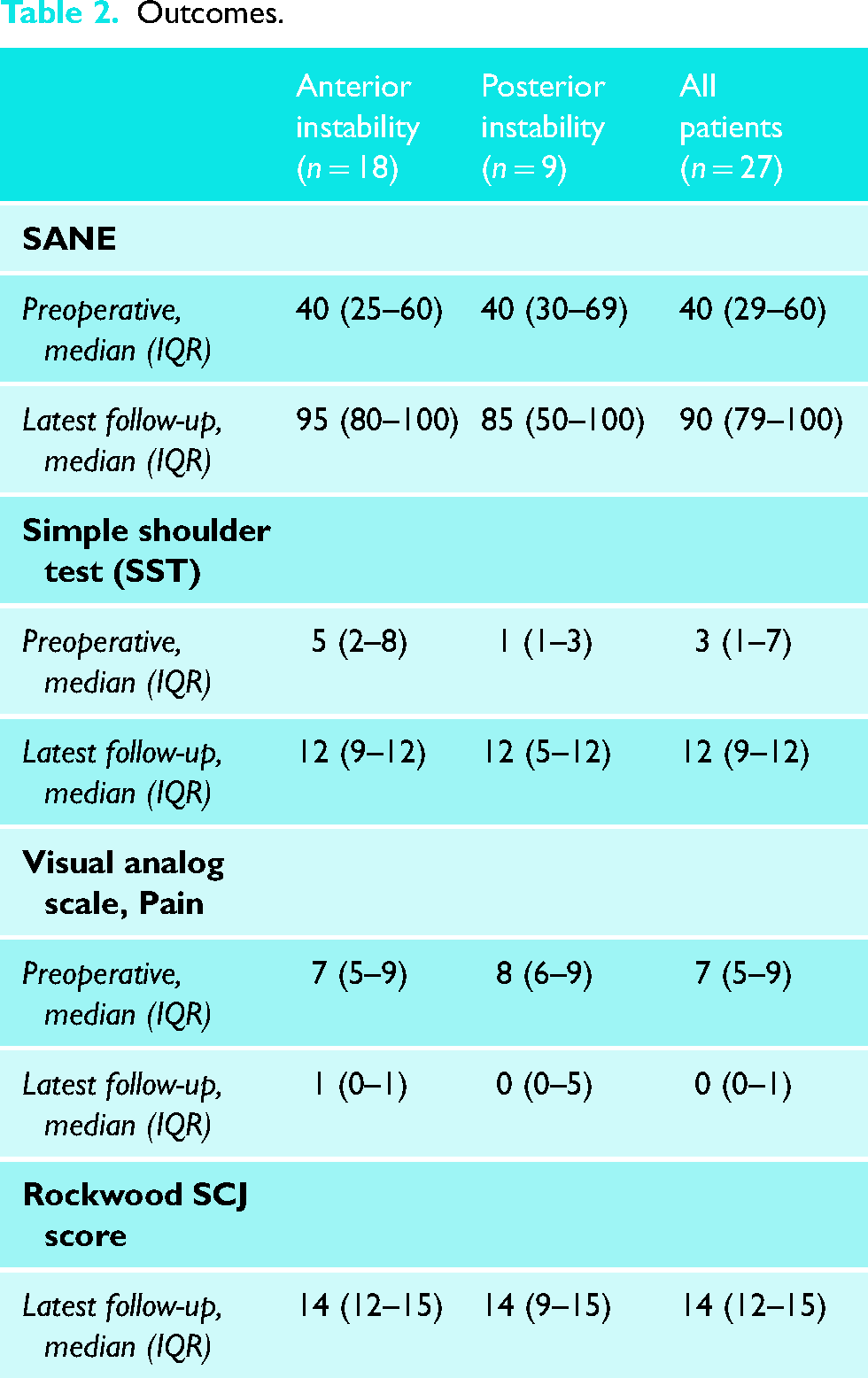
Minimum 2-year outcomes for tendon graft reconstructions for SCJ instability: Clinical outcome measures are shown in Table 2
SANE scores improved from a median of 40 to 90 at latest follow-up (P < .0001). SST scores improved from a median of 3 positive responses at baseline to a median of 12 on a 12-point scale (P < .0001). VAS scores for pain decreased from a median of 7 to 0 points (P < .0001). One patient with an initial diagnosis of anterior instability underwent reoperation for recurrent instability; there were no additional reoperations related to the SCJ reconstruction. Three patients did not achieve a minimum 30% of maximum possible improvement (MPI) in SST scores (11%); of these, 1 was the aforementioned patient who underwent reoperation, and 2 patients were in the posterior instability group.
One patient underwent reoperation for instability after a motor vehicle accident. A total of 3 patients had persistent symptoms and did not achieve a minimum 30% MPI in SST scores. One patient, a farmer with an active worker's compensation claim, had continued difficulty with overhead activity at latest follow-up. He reported that he would, however, recommend the surgery to a friend or family member. Another patient had previously undergone a 5-cm medial clavicle resection at an outside institution with subsequent difficulty with dysphonia, stridor, and neck pain. Following a technically successful reconstruction procedure, pain and functional limitations unfortunately persisted.
Clinical improvement and stability at a minimum of 2 years after surgery
In this series, patients who underwent tendon graft reconstruction for SCJ instability had significant clinical improvement with regard to patient-reported pain and functional outcome measures. There was 1 reoperation for recurrent instability. Most patients (89%) achieved a minimum 30% MPI in patient-reported outcomes.
Discussion
Over the last decade, there has been renewed interest in reconstructive techniques for the patient with severe symptoms and chronic SCJ instability. In 2014, Uri et al. 8 reported a case series of 32 reconstructions using a SCM transfer technique, in which a segment of the proximal SCM was detached, looped around the clavicle, and secured to the sternum with nonabsorbable suture. Notably, these authors preserved the medial clavicle if no evidence of arthritis was noted. Postoperative instability was observed in only 2 patients, with otherwise excellent improvement in patient-reported outcomes. Bak and Fogh 7 reported 27 reconstructions using autograft tendon secured with a suture anchor, also with improvements in patient-reported outcomes and with 2 complications requiring reoperation.
In 1938, Bankart 16 described a technique for reconstruction of the unstable SCJ using fascia lata autograft passed through bone tunnels in the clavicle and manubrium. Most recent clinical series have used a variation of this technique using autograft or allograft tendon passed through bone tunnels. As shown in Table 3, these series demonstrate significant improvements in patient-reported outcomes at follow-up periods ranging from 1 to 5 years and reoperation rates ranging from 0% to 17%. The present study demonstrates similar findings in one of the largest case series to date, with statistically significant improvements in patient-reported outcomes and pain in addition to a low reoperation rate.
Selected published outcomes, open treatment of sternoclavicular instability with tendon reconstruction.
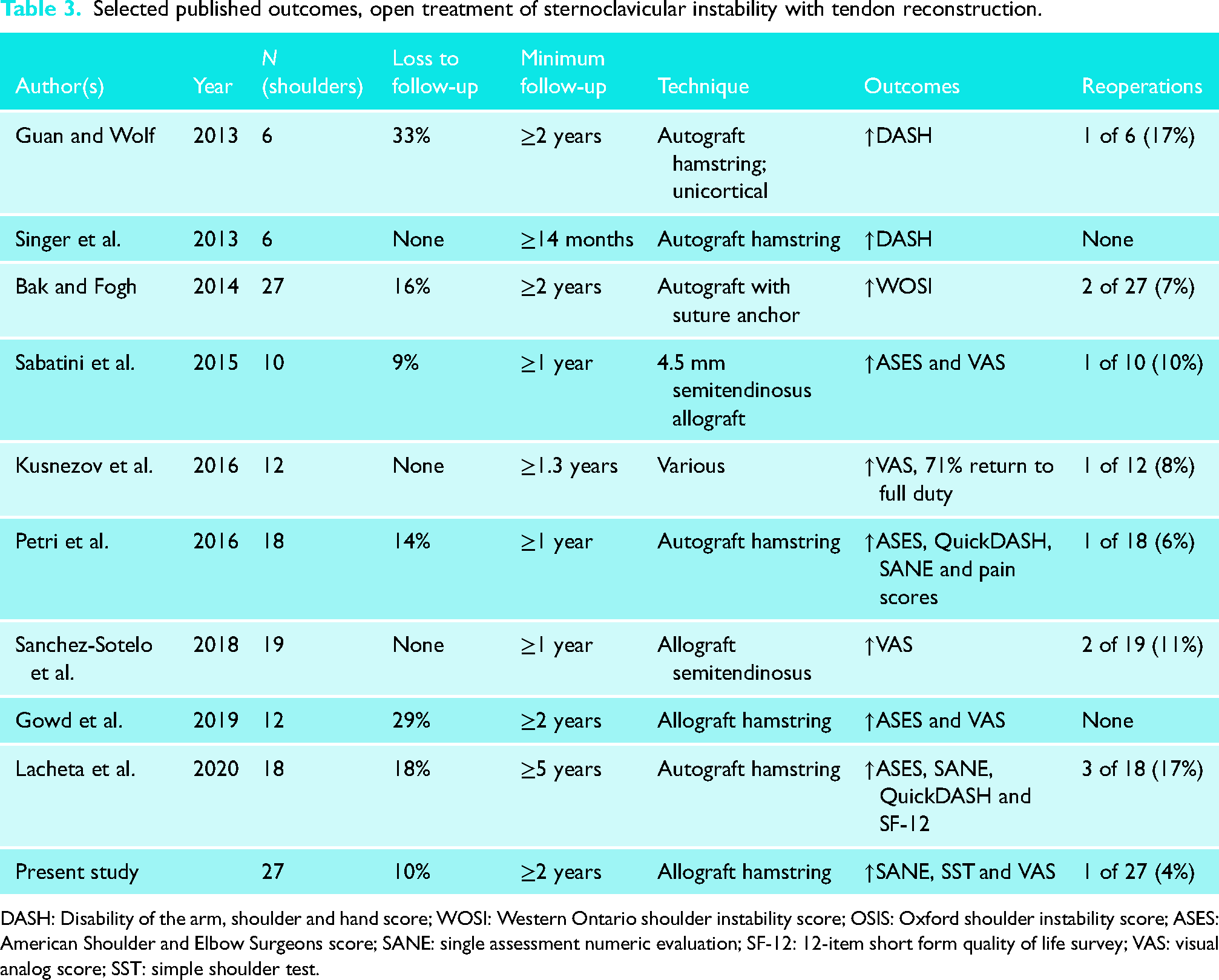
DASH: Disability of the arm, shoulder and hand score; WOSI: Western Ontario shoulder instability score; OSIS: Oxford shoulder instability score; ASES: American Shoulder and Elbow Surgeons score; SANE: single assessment numeric evaluation; SF-12: 12-item short form quality of life survey; VAS: visual analog score; SST: simple shoulder test.
In this series, resection of the medical clavicle was kept to a minimum, generally less than 5 mm. This is in contrast to prior authors, who often recommended substantial resection of the medial clavicle. 17 Biomechanical testing by Katthagen et al. 18 has supported a “minimalist” approach to resection, with a 5-mm resection parallel to the joint line providing adequate joint decompression. A clinical outcome study by the same research group confirmed a low rate of post-traumatic or post-reconstruction arthritis at minimum 5-year follow-up. 5 This mirrors the experience of the senior author, who has not observed long-term sequelae of inadequate resection. Conversely, the sequelae of excessive resection can be challenging to manage. 19
Clinical reports to date regarding tendon graft reconstruction for posterior instability have been limited to very small case series. A recent systematic review 4 identified only 11 previously published cases of tendon graft reconstruction for chronic posterior SCJ instability, with the largest series 20 reporting outcomes of 4 cases. All 4 of these patients returned to military duty with improvements in pain and range of motion; however, patient-reported outcome measures were not included in this study. This makes it difficult to counsel patients regarding the expected outcomes after this procedure. In our series, there were no reoperations or major complications among 9 patients with reconstruction performed for posterior instability. However, 2 of these 9 patients did not reach 30% MPI in their SST score at latest follow-up. The reasons for this disparity in outcomes are not clear and require further study.
Limitations
Limitations of this study include: (a) the lack of long-term clinical and radiographic follow-up to ascertain whether the minimalist resection strategy in chronic instability cases with concomitant SCJ arthritis results in symptomatic arthritis, (b) the lack of additional patient-reported outcome measures, such as the American Shoulder and Elbow Surgeons score or quality of life measures, and (c) the fact that all surgeries were performed in a quaternary referral practice that may not be generalizable to other practice settings.
In conclusion, patients who underwent tendon graft reconstruction for SCJ instability had good functional outcomes and a high level of return to work and sport. The presented techniques for reconstruction of anterior and posterior instability allow for safe tunnel placement with durable 2-year outcomes.
Footnotes
Contributorship
JSS did conceptualization, methodology, project administration, supervision, writing the original draft, reviewing and editing. KMP did conceptualization, formal analysis, investigation, methodology, project administration, writing the original draft, reviewing and editing. WJW did formal analysis, investigation, methodology, writing the original draft, reviewing and editing. All authors approved the final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval (IRB# STUDY00008239) was granted by the University of Washington Human Subjects Division for a retrospective review of a longitudinal, prospectively compiled outcomes database.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
JSS.
Informed consent
Informed consent was waived by the University of Washington Institutional Review Board (IRB#STUDY00008239).