
Abstract
Background:
The detection and management of chondral injuries of the hip, especially in a younger patient population, may preempt joint degeneration. Although the outcomes of preservation techniques have been well described for other weightbearing joints, such as the knee, evidence for hip joint preservation after procedures such as microfracture and autologous chondrocyte implantation remains in its infancy.
Purpose:
To evaluate outcomes of joint preservation procedures in the hip, including the success rate and patient-reported outcomes (PROs).
Study Design:
Systematic review; Level of evidence, 4.
Methods:
This review was performed using the terms “hip arthroscopy,” “microfracture,” “autologous chondrocyte implantation,” “fibrin glue,” “osteochondral transfer,” and variations thereof in 5 electronic databases, yielding 325 abstracts. After the application of eligibility criteria, 19 articles were included. Weighted means were calculated for PROs, and pooled estimates were calculated for age, follow-up, chondral lesion size, and success of hip preservation procedures with a random-effects proportion meta-analysis.
Results:
A total of 1484 patients (1502 hips) were identified across 19 studies (mean age, 38.0 ± 1.3 years; mean follow-up, 31.8 ± 9.6 months). Hip joint preservation techniques demonstrated a high success rate, ranging from 85.6% to 99.7%. The mean pooled chondral lesion size was 2.5 ± 0.3 cm2 (95% CI, 1.9-3.0 cm2). Microfracture was the most frequent technique, utilized by 11 studies, and demonstrated an 89.6% success rate (95% CI, 82.4%-96.7%). The highest pooled success rate was exhibited by autologous membrane-induced chondrogenesis in 3 studies (99.7% [95% CI, 99.0%-100.0%]). All PROs demonstrated a statistically significant increase postoperatively, including the modified Harris Hip Score, Nonarthritic Hip Score, and Hip Outcome Score–Activities of Daily Living and Hip Outcome Score–Sports-Specific Subscale (all P < .05). The visual analog scale for pain also demonstrated a statistically significant decrease of 37.2% (P < .05).
Conclusion:
Hip preservation procedures demonstrate a high success rate, with microfracture representing the most frequently utilized cartilage preservation technique in the peer-reviewed literature. PROs significantly improved after surgery. Further investigation of hip preservation modalities with long-term follow-up is required to create evidence-based clinical recommendations and treatment algorithms.
Keywords
The detection and management of chondral injuries of the hip, especially in the younger patient population, may prevent or delay hip joint degeneration. Long-term outcomes of cartilage defects within the hip result in pain, early degenerative changes, and the subsequent development of arthritis. 28,29 Although nonsurgical methods, such as physical therapy and activity modification, may have utility in the alleviation of symptoms such as pain and functional restrictions, hip joint preservation techniques that address the underlying issue have shown promising results. ∥
Multiple causes have been associated with chondral injuries of the hip, most notably femoroacetabular impingement (FAI) 2,4,7,17,28,29,44 as well as trauma, labral tears, arthritis, dysplasia, and osteonecrosis. In FAI, the pattern of chondral damage is determined by the pathological lesion of the hip and the resulting impingement that occurs. The asphericity of the femoral head results in impingement with the anterosuperior acetabulum and subsequent delamination of the chondrolabral junction. 40
The severity of defects of the articular surface occurs along a spectrum, progressing from superficial or partial-thickness disruptions to complex and full-thickness defects with underlying subchondral bone loss. 40 Superficial cartilage lesions have limited capacity to spontaneously heal if left untreated. The management options for an articular cartilage injury have proliferated, including microfracture, articular cartilage repair, autologous chondrocyte implantation (ACI), autologous osteochondral graft transplantation (also known as mosaicplasty), osteochondral allograft transplantation, and the use of fibrin adhesive. Surgeons are often unprepared for the management of such defects, as conventional magnetic resonance imaging demonstrates low sensitivity in the detection of cartilage lesions within the hip. Blankenbaker et al 5 demonstrated a sensitivity of 70% in detecting cartilage defects, which were identified during arthroscopic surgery, with other studies reporting values as low as 50%. 35,41
Despite the extensive peer-reviewed literature regarding the utility of these approaches for the other weightbearing joints such as the knee, evidence for hip joint preservation remains in its infancy. The purpose of this systematic review and meta-analysis was to assess outcomes of joint preservation procedures in the hip, including the success rate and change in patient-reported outcomes (PROs).
Methods
Search Strategy
This systematic literature review and meta-analysis was structured to adhere to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. In October 2017, an electronic search was completed utilizing 5 databases, including PubMed, Cochrane Library, Scopus, Web of Science, and Google Scholar. The following search terms were used: “hip arthrosc*,” OR “hip,” OR “arthroscopy” AND (“microfracture,” OR “autologous chondrocyte implantation,” OR “fibrin glue,” OR “osteochondral transfer”). The reference lists of the 19 studies that met the inclusion criteria were also reviewed.
Identification of Eligibility
To be eligible for inclusion, a study must have assessed hip joint preservation procedures in a patient population, with a minimum mean patient age of 18 years (adults), a quantifiable postoperative outcome measure, and a Coleman Methodology Score (CMS) greater than 50. A tiebreaker was designated in the case of any disagreement. Articles assessing preoperative conservative care techniques, case reports, and expert opinions were excluded (Table 1). Two authors (M.O. and A.A.M.) identified the appropriate articles for inclusion utilizing the title and abstract, which was followed by the full article as needed. A tiebreaker (T.S.L.) was designated in the case of any disagreement after the initial review.
Study Inclusion and Exclusion Criteria

Statistical Analysis
The method of data extraction and analysis followed the approach outlined by the Cochrane Handbook for Systematic Reviews of Interventions. 8 The evaluation of aggregate data from clinical studies was completed utilizing a random-effects proportion meta-analysis weighted for individual study size using OpenMeta[Analyst] software (Centre for Evidence-Based Medicine). Accordingly, studies that did not report ranges or SDs were excluded. Weighted means were calculated for PROs. Pooled estimates were calculated for age, chondral lesion size, and success rate of hip preservation procedures. The quality of the included studies was calculated using the CMS as determined by 2 reviewers (M.O. and A.A.M.). A third tiebreaker (T.S.L.) was designated in the case of any disagreement.
Results
Eligibility
Of the 261 articles assessed, 201 were excluded based on the title or abstract of the article, while 41 were excluded after a review of the full text. After application of the eligibility criteria, a total of 242 articles were excluded (Figure 1), and 19 articles were included (Table 2).

Study selection process (PRISMA diagram).
Characteristics of Included Studies a

a ACT, autologous chondrocyte transplantation; AMIC, autologous membrane-induced chondrogenesis; MACI, matrix-induced autologous chondrocyte implantation; NR, not reported.
b Median (range).
c Mean ± SD.
Quality of Included Articles
The mean modified CMS was 70.9 ± 6.3 out of a possible total score of 100 (Table 3). The enrolled studies scored particularly well on proportion with follow-up (4.4/5), diagnostic certainty (5.0/5), description of surgical technique (5.0/5), description of postoperative rehabilitation (5.0/5), and outcome criteria (9.9/10) based on the CMS.
Coleman Methodology Scores

Participants
In total, 1484 patients (1502 hips) were identified (mean age, 38.0 ± 1.3 years; 64.1% male, 35.9% female) with a mean follow-up of 31.8 ± 9.6 months. The proportion of patients undergoing bilateral hip preservation was 1.21%.
Outcomes After Hip Preservation Procedures
The success or failure of hip preservation procedures, indicated by the need for conversion to total hip arthroplasty (THA) or revision arthroscopic surgery/reoperation, was reported by 13 studies (68.4%) (Figures 2 –5). All hip joint preservation techniques demonstrated a high success rate (range, 85.6%-99.7%) (Table 4).

Success rate after microfracture. Ev, event; Trt, group.

Success rate after fibrin adhesive (with microfracture). Ev, event; Trt, group.
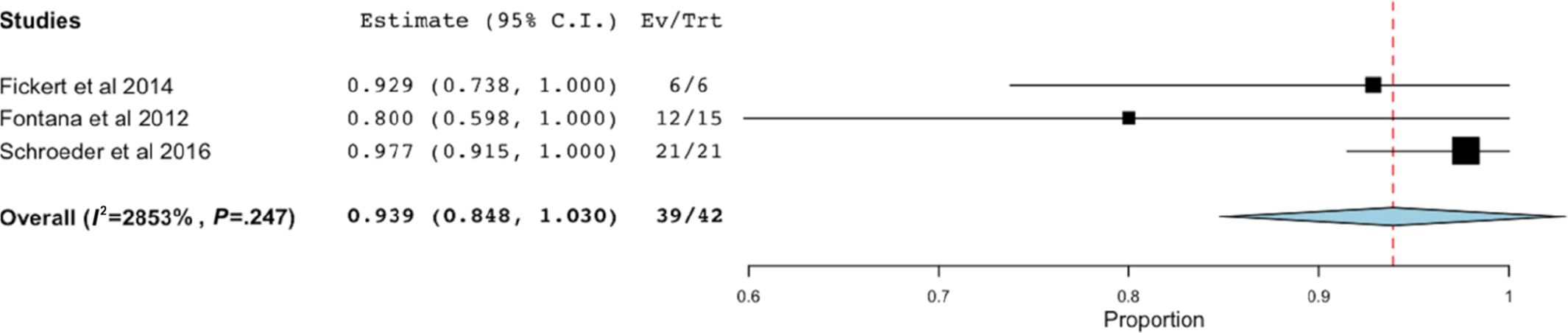
Success rate after autologous chondrocyte transplantation. Ev, event; Trt, group.

Success after autologous membrane-induced chondrogenesis. Ev, event; Trt, group.
Success of Hip Preservation Procedures a

a ACT, autologous chondrocyte transplantation; AMIC, autologous membrane-induced chondrogenesis; MACI, matrix-induced autologous chondrocyte implantation; THA, total hip arthroplasty.
b Assessed by only 1 study. 30
Chondral Lesions
The mean pooled chondral lesion size was 2.5 ± 0.3 cm2 (95% CI, 1.9-3.0 cm2; I 2 = 98.4%), and 93.7% were acetabular in location (Table 5). Two studies 6,9 determined that there was no difference in the success of the procedure between patients undergoing acetabular microfracture and those undergoing femoral microfracture. Additionally, lesion size had no correlation with PROs, but location did have an impact on PROs. 10,27 A lesion located anteriorly was associated with a higher modified Harris Hip Score (mHHS) and Nonarthritic Hip Score (NAHS), while wider lesions correlated with higher Hip Outcome Score (HOS)–Activities of Daily Living (ADL), HOS–Sports-Specific Subscale (SSS), and NAHS values at 2-year follow-up. 10
Lesion Size and Lesion Location a

a NR, not reported.
Microfracture
Microfracture was the most commonly utilized cartilage preservation technique, appearing in 11 articles (Table 6). In one of the studies that addressed failure, there were 2 (6.7%) patients who progressed to THA and 2 (6.7%) who underwent revision arthroscopic surgery. 9 In this study, the presence of loose bodies was more common in those who failed than those who succeeded (P = .018). 9 A second study had 6 (7.8%) patients who were converted to THA. 16 When assessing the fill of repair tissue at second-look hip arthroscopic surgery, a fill rate ranging from 91% to 96% was found. 24
Outcomes After Microfracture a
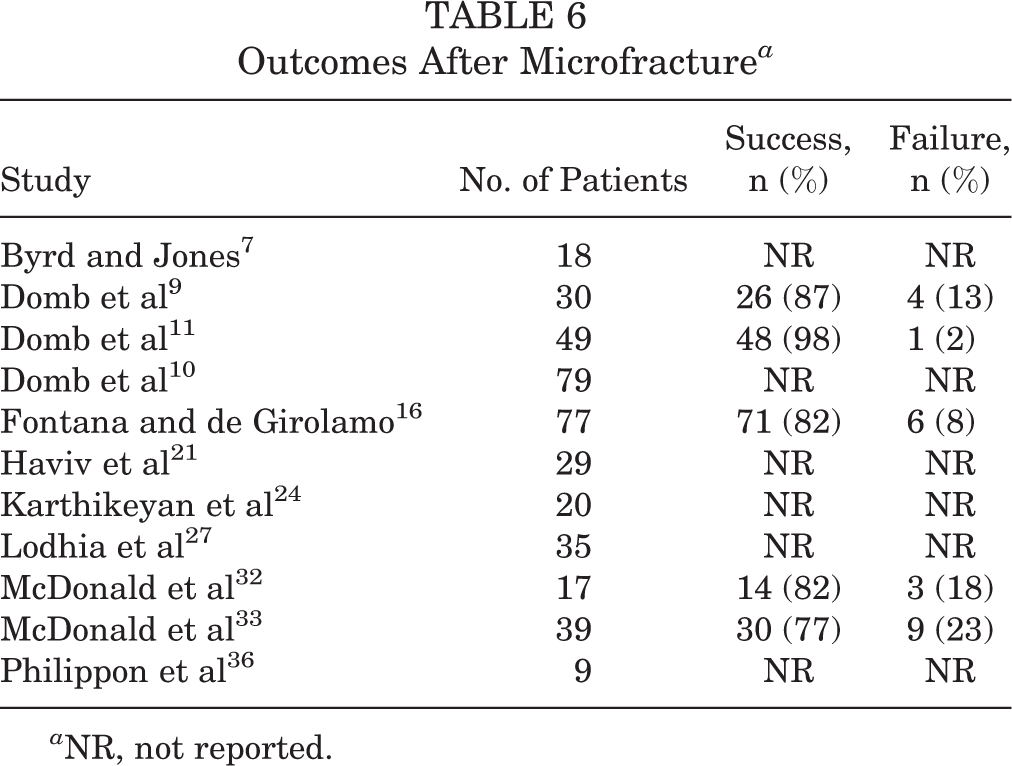
a NR, not reported.
With regard to return to sport, the number of lesions or their presence on weightbearing surfaces posed no increased risk of failure to return to sport. 33 Similarly, no difference was found based on age, number of seasons played before surgery, 32 or contact sport involvement. 33
Although results varied in the comparison of PRO improvements after microfracture compared with controls, 5,10,11,16,27,33 short-term improvements in microfracture patients slowly began to decline after the first postoperative year. 16 No statistically significant difference was found between athletes who underwent microfracture and controls for the likelihood of returning to sport.
Fibrin Adhesive (With Microfracture)
The use of fibrin adhesive resulted in significant improvement in the mHHS as well as pain and function subscales compared with baseline at a minimum 1-year follow-up in 2 studies (n = 62 patients). 38,42 Of a total of 8 patients requiring a reoperation, 5 (8.1%) underwent revision hip arthroscopic surgery and 3 (4.8%) underwent THA (Table 7).
Outcomes After Fibrin Adhesive

Autologous Chondrocyte Transplantation (ACT)
The pooled success rate of ACT was 93.9% (95% CI, 84.8%-100.0%) 13,15,37 (Table 8). Of the studies that reported on failure, no patient was converted to THA. 13,15,37 For PROs, a large lesion was found to result in a lower postoperative mHHS (P = .03) 13 and a lower Subjective Hip Value at 1 year postoperatively (R = –0.519). 37 Although patient age was found to have no effect on the PROs, women trended as scoring lower compared with their male counterparts. 37
Outcomes After Autologous Chondrocyte Transplantation a

a NR, not reported.
The difference between refixation and resection of the labrum had no effect on the postoperative PROs. 13 When comparing ACT with simple debridement, ACT demonstrated significantly better postoperative PROs at a mean of 6 years after hip arthroscopic surgery.
Autologous Membrane-Induced Chondrogenesis (AMIC)
The AMIC cartilage preservation procedure was assessed in 3 studies from the same institution, with a success rate of 100% and significant improvement in PROs compared with baseline 14,16,30 (Table 9). No patients were converted to THA. 14,16,30 One patient underwent a second hip arthroscopic procedure because of an unrelated event, at which time the cartilage fill was 100%. 30
Outcomes After Autologous Membrane-Induced Chondrogenesis
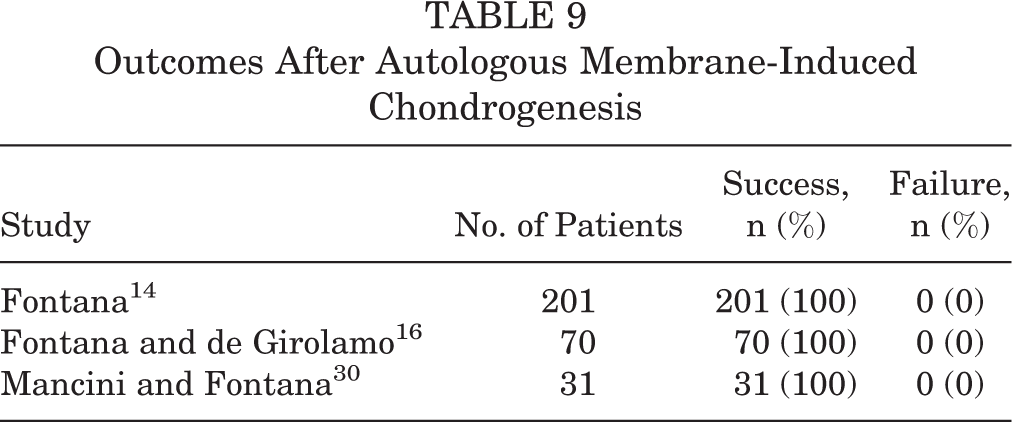
All 3 studies reported positive results at 5 years after AMIC for medium-sized chondral defects of the hip, which were 2 to 4 cm. 14,16,30 AMIC had better sustained improvement over the 5 years after surgery, 16 which is in contrast to microfracture, in which improvement slowly began to decline after the first postoperative year.
Matrix-Induced ACI (MACI)
Only 1 study addressed the MACI procedure. 30 This study reported a success rate of 100% (26/26), with no patients progressing to THA. The AMIC and MACI procedures were compared and were found to have no significant differences in postoperative PROs.
Meta-analysis of PROs
A total of 16 studies (84.2%) reported at least 1 PRO, which were available for microfracture, ACT, AMIC, and MACI. A statistically significant postoperative increase in scores was observed for microfracture (mHHS: 10.0%; NAHS: 13.3%; HOS-ADL: 23.0%; HOS-SSS: 57.6%; visual analog scale [VAS] for pain: 37.2%) (Figure 6), ACT (mHHS: 54.0%; NAHS: 41.6%; 36-Item Short Form Health Survey [SF-36] physical: 95.4%; SF-36 mental: 57.0%; International Hip Outcome Tool: 93.2%) (Figure 7), AMIC (mHHS: 26.7%), and MACI (mHHS: 83.9%) (Figure 8).
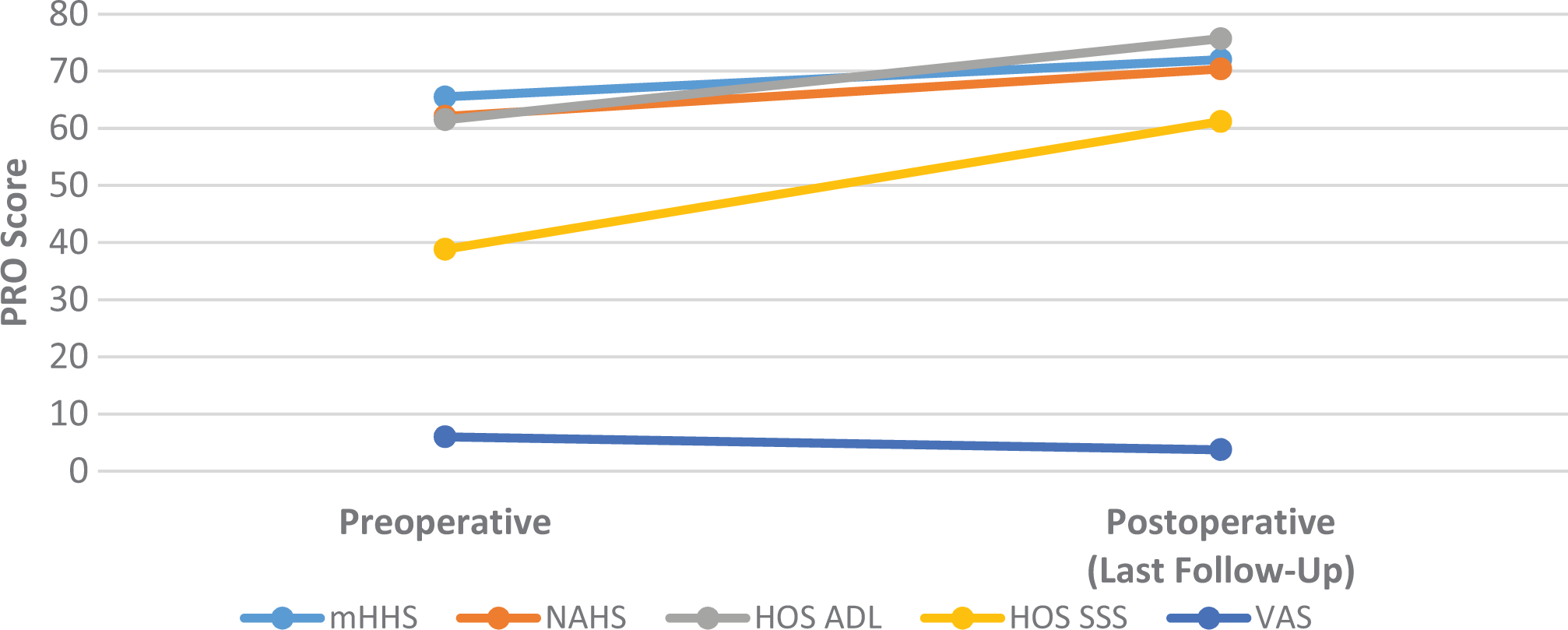
Change in patient-reported outcomes (PROs) after microfracture. ADL, Activities of Daily Living; HOS, Hip Outcome Score; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; SSS, Sports-Specific Subscore; VAS, visual analog scale.

Change in patient-reported outcomes (PROs) after autologous chondrocyte transplantation. *Reported by 1 clinical study. iHOT-33, International Hip Outcome Tool; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; SF-36, 36-Item Short Form Health Survey.

Mean aggregate change in patient-reported outcomes (PROs) per technique. *Reported by 1 clinical study. 30 ACT, autologous chondrocyte transplantation; AMIC, autologous membrane-induced chondrogenesis; MACI, matrix-induced autologous chondrocyte implantation.
Discussion
This systematic review and meta-analysis evaluated 19 clinical studies with a total of 1484 patients (1502 hips) to assess the outcomes of joint preservation procedures in the hip, including the success rate and PROs. The success rates ranged from 85.6% to 99.7%, with microfracture being the most commonly utilized cartilage preservation technique, appearing in 11 articles. ¶ The highest pooled success rates were found for AMIC (99.7%), ACT (93.9%), microfracture (89.6%), and fibrin adhesive use (85.6%). Only 1 study 30 assessed MACI, reporting a success rate of 100% (26/26). Given the overlap of CIs in the success rates across procedures, inferences regarding the superiority of any single approach are subsequently limited.
Although the mean pooled estimate for chondral lesion size was 2.5 ± 0.3 cm2, significant heterogeneity in size was found (I 2 = 98.4%). Most importantly, 2 studies 6,9 found no difference in the rate of success in patients undergoing acetabular microfracture in comparison with femoral microfracture. This implies that the findings regarding the success of this procedure could be extrapolated to cartilage damage to the hip in general.
Additionally, of the 16 studies that reported at least 1 PRO, a statistically significant increase was observed postoperatively after microfracture (Figure 6), ACT (Figure 7), AMIC, and MACI (Figure 8). The VAS score for pain also demonstrated a statistically significant decrease after microfracture of 37.2% (P < .05). However, given the heterogeneity of indications and patient selection between study types, no inferences can be made regarding the superiority of hip preservation techniques by an improvement in PROs.
The most commonly assessed treatment for cartilage preservation in the hip, microfracture, is a technique that attempts to stimulate the subchondral bone where the chondral defect resides by creating small holes. 34 The damage to the bone caused by this technique results in recruitment of growth factors and stem cells to facilitate chondral healing by the formation of a “super clot.” 19 The indications for microfracture in the hip, including minimal osteoarthritis and contained lesions <4.0 cm in size, have been inferred from the published knee literature. 20,24,25,36,39 Despite the favorable outcomes of microfracture in the hip, longer term studies are necessary to determine the utility of microfracture for chondral injuries of the hip. 12
Although microfracture appears to demonstrate successful outcomes in patients with minimal or no osteoarthritis, it does not appear to improve hips with advanced lesions. In a report by Horisberger et al, 22 on 20 patients with Outerbridge grade III or IV lesions of the acetabulum, 50% of the patients underwent or were scheduled for THA at a mean 3-year follow-up. Of note, Domb et al 10 determined that lesions located anteriorly were associated with higher mHHS and NAHS values, while wider lesions correlated with higher HOS-ADL and HOS-SSS as well as NAHS values at 2-year follow-up. Further research can be conducted to utilize this factor as a prognostic indicator of postoperative function.
Similar to microfracture, indications for ACI of the hip have been extrapolated from the knee, such as solitary chondral lesions 3,18,25,31,45 with no presence of osteoarthritis. 12 This approach works by culturing chondrocytes taken from the injured area. These cells are then grown for 2 to 6 weeks on a 3-dimensional membrane to create a viable chondrocyte membrane that can be transplanted to the defect’s location. This technique requires 2 distinct procedures: harvesting of the chondrocytes and transplantation of the grown membrane. 15 In comparison with ACI, MACI is a less frequently used cartilage preservation technique that can be completed arthroscopically. 23 However, it is currently available only for the repair of single or multiple symptomatic full-thickness cartilage defects of the knee in the United States. 43
AMIC offers similar benefits to ACT while only requiring 1 surgical procedure. In this technique, microfracture is first performed, after which a collagen membrane matrix is placed over the area of chondral damage. The stem cells that are recruited by microfracture are able to differentiate (stimulated by the growth factors released after microfracture) to allow for the development of more chondral tissue. 23
Last, fibrin adhesive is made from fibrinogen and thrombin and helps to promote the bonding of tissue. 1 In the hip, fibrin adhesive glues the delaminated cartilage to the subchondral bone after microfracture to recruit stem cells and growth factors to the area. 38 Despite the pooled success rate of 85.6%, the 2 studies reporting on this approach demonstrated varying success (93% and 74%) in 43 and 19 patients, respectively. 38,42
Significance and Limitations
To the best of our knowledge, this systematic review and meta-analysis represents the first comprehensive assessment of outcomes of joint preservation procedures in the hip. A limitation to this review includes the small number of studies (n = 12) that specifically reported the success and/or failure of hip preservation procedures at medium-term follow-up. Additionally, pooled estimates demonstrated wide CIs as a result of the limited number of studies meeting eligibility criteria. Accordingly, the rates of success or change in PROs should not serve as an indication regarding the superiority of one approach compared with another. As more evidence becomes available, narrower estimates will be made possible. Of note, the pooled estimate of chondral lesion size was reported to provide an estimate for the overall lesion size.
Another limitation arises from the lack of inclusion of PROs from all eligible studies secondary to missing data, such as SDs or CIs. Given the limitations from enrolled studies, the definition of success utilized in this meta-analysis and systematic review was set at a low bar (as failures being represented by the need for conversion to THA or revision arthroscopic surgery/reoperation), and future studies should include PROs to better assess results. Finally, variation in the inclusion criteria employed by the eligible studies represented a challenge in data aggregation and the meta-analysis process.
Of note, multiple studies were performed at the same institutions, introducing a source of potential bias. Additionally, concomitant procedures that were performed may have affected outcomes, despite the utilized methodology in statistical analysis. Finally, there were few comparison studies as well as second-look procedures or biopsies in the included studies.
Conclusion
Hip preservation procedures demonstrated a high success rate, ranging from 85.6% to 99.7%, and resulted in a significant improvement of PROs at more than 2-year follow-up. Microfracture was the most commonly utilized cartilage preservation technique. Further investigation of hip preservation modalities with long-term follow-up is required to create evidence-based clinical recommendations and treatment algorithms.
Footnotes
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.W.W. has received educational support from Smith & Nephew and has received hospitality payments from Smith & Nephew and Zimmer Biomet. J.R. is a consultant for Smith & Nephew and has received educational support from Smith & Nephew. T.S.L. is a consultant for Smith & Nephew and has received educational support from Arthrex.