
Abstract
Osteochondral lesions of the talus (OLTs) are a difficult pathologic entity to treat. They require a strong plan. Lesion size, location, chronicity, and characteristics such as displacement and the presence of subchondral cysts help dictate the appropriate treatment required to achieve a satisfactory result. In general, operative treatment is reserved for patients with displaced OLTs or for patients who have failed nonoperative treatment for 3 to 6 months. Operative treatments can be broken down into cartilage repair, replacement, and regenerative strategies. There are many promising treatment options, and research is needed to elucidate which are superior to minimize the morbidity from OLTs.
Keywords
Osteochondral lesions of the talus (OLTs) are lesions of the articular cartilage of the talus and underlying subchondral bone. As such, the term encompasses a variety of pathologies, including: osteochondritis dissecans, osteochondral defects, and osteochondral fractures. Trauma accounts for the majority of OLTs, with an OLT occurring with over half of ankle sprains and a larger percentage of ankle fractures. 44,61 Given the large number of ankle injuries with potential for cartilage injury, OLTs are an important problem, and adequate treatment is necessary to reduce morbidity and allow patients to return to sport or activities of daily living.
OLTs are difficult to treat and remain a significant challenge for orthopedic surgeons for many reasons. First, the lesions have limited healing potential due to the poor regenerative capacity of articular cartilage and the poor blood supply of the talus. Many surgical procedures have been developed to overcome the limited healing potential. However, there have been few comparative outcome studies looking at these different treatments, and as such, there are no consensus guidelines on appropriate treatment. In general, operative treatment is indicated for lesions that remain symptomatic despite 3 to 6 months of nonoperative treatment or for displaced OLTs of any chronicity. Operative treatments can be grouped into 3 large categories: cartilage repair, replacement, and regenerative strategies. This article aims to review the pathophysiology, diagnosis, staging, and treatment of osteochondral lesions of the talus as well as to discuss controversies and future considerations surrounding the topic.
Pathophysiology
As OLTs encompass a range of disease, the pathophysiology is not singular. Osteochondritis dissecans is a focal, idiopathic lesion of the subchondral bone with risk for instability and disruption of the adjacent articular cartilage. 20 The dysfunction of the subchondral bone is thought to be vascular in nature, with osteonecrosis of the subchondral bone contributing to damage to the overlying cartilage. The vascular insult may be secondary to repetitive microtrauma or to a disruption of the anastomosing vessels between the cartilage and subchondral bone during development, but the exact pathophysiology is unknown. 47 The ankle is the third most common joint to be affected by osteochondritis dissecans after the knee and elbow. The incidence of osteochondritis dissecans of the talus is approximately 0.09%, and it most commonly affects those in the second decade of life. 4 Osteochondritis dissecans can be asymptomatic, but common symptoms include pain as well as mechanical symptoms such as locking or catching when cartilage detaches from the underlying defective subchondral bone.
Most OLTs, including osteochondral defects and frank osteochondral fractures, are secondary to trauma. Approximately 50% of ankle sprains and up to 73% of ankle fractures result in some level of cartilage injury, and there are over 2 million ankle sprains alone per year. 44,61,70 Classic teaching is that lateral OLTs are more likely due to trauma than medial lesions, with 94% of lateral lesions and 62% of medial lesions being caused by trauma. 66 The mechanism for traumatic impaction of the lateral talar dome is axial load combined with inversion and dorsiflexion, whereas axial load combined with plantarflexion, inversion, and possibly external rotation results in medial talar dome impaction. 8 Several large studies evaluating anatomic characteristics of OLTs found the majority of lesions to be located in the centromedial and centrolateral zones. 22,27 These studies also found that medial lesions tended to be deeper and associated with subchondral changes, which lends credence to the idea of a pathophysiology other than trauma being contributory to the development of some medial talar lesions. 8
Talar bone and cartilage are particularly vulnerable to developing osteochondral lesions secondary to several anatomic features. First, over 60% of the talus is covered by cartilage, which has poor intrinsic regenerative capacity due to its avascularity. As such, cartilage relies on nutrition from synovial fluid and from the subchondral bone. The fact that the talus has poor blood supply leads to a further diminished ability for talar cartilage to heal after injury. The blood supply to the talus comes from a complex anastomotic network between branches of the peroneal, posterior tibial, and anterior tibial arteries. This complex network from multiple vessels leads to watershed areas, with 1 cadaveric study showing relatively poor perfusion in the posteromedial, posterolateral, and mid-medial sections of subchondral bone on the 9-section anatomical grid. 45 Furthermore, the blood supply to the talar dome and overlying cartilage is retrograde, making it more tenuous in the setting of certain injuries. Last, talar cartilage is relatively thin compared to other weightbearing joints in the lower extremity. Shepherd and Seedhom 65 showed that the thickness of cartilage in cadavers was statistically significantly thinner in the ankle compared to the hip and knee. They found a thickness of 0.7 to 1.2 mm in the ankle compared to 1.5 to 2.6 mm in the knee. All of these factors make the talus particularly vulnerable to developing osteochondral lesions.
Evaluation and Diagnosis
Presentation of patients with OLTs varies and depends on many factors, including the etiology and acuity of their lesion. The most common symptoms associated with OLTs, including pain, swelling, and stiffness, are quite nonspecific. These symptoms are often exacerbated by weightbearing. In addition, mechanical symptoms such as locking and catching that are often associated with cartilage abnormalities in other joints occur infrequently with OLTs. Thus, clinicians must maintain a high degree of suspicion for these lesions as initial evaluation will often yield broad differential diagnoses. These include but are not limited to occult fractures, hindfoot coalitions or deformity, syndesmotic injury, lateral ankle instability, peroneal tendonopathy, impingement, and ankle or subtalar arthritis. 19
When there is concern for an OLT, the patient should be questioned about a history of trauma to the ankle. Physical examination may reveal an effusion, tenderness to palpation over the lesion, decreased range of motion, and pain with inversion or dorsiflexion. 49 Provocative tests, including anterior drawer and talar tilt, should be performed, and all examination maneuvers should be compared to the contralateral ankle. Radiographic examination with weightbearing anteroposterior, lateral, and mortise ankle views of the ankle joint should be performed. Advanced imaging with magnetic resonance imaging (MRI) or computed tomography (CT) scan may be necessary to visualize lesions not seen on radiographs or to further characterize lesions apparent on radiography.
Imaging and Staging
Weightbearing anteroposterior, lateral, and mortise radiographic views of the affected ankle are the recommended first line of imaging for evaluation of OLTs. Berndt and Harty 8 described the first classification of OLTs with radiography in 1959 (Table 1). In their original classification, stage I is a small area of subchondral compression, stage II is a partially detached osteochondral fragment, stage III is a completely detached osteochondral fragment without displacement from the fracture bed, and stage IV is a detached and displaced osteochondral fragment. 8
Staging Systems of Osteochondral Lesions of the Talus.

If radiographs are negative but an osteochondral lesion is still suspected, advanced imaging with MRI or CT scan is indicated. These imaging modalities each have pros and cons for evaluation of osteochondral lesions. However, MRI has a higher sensitivity for detecting OLTs and is thus the study of choice for detecting OLTs after negative radiographs. Verhagen et al 69 found MRI and CT scan to have sensitivities of 0.96 and 0.81, respectively, in identifying OLTs.
MRI provides excellent visualization of the articular surface and soft tissues, which is very helpful for characterizing OLTs. 17 However, with its demonstration of edema in the bone and cartilage, it may overestimate the size of OLTs or make it difficult to assess the true status of the bone and the exact dimensions of the osteochondral lesion. 19 In contrast, CT scans allow for better visualization of the state of the subchondral bone and the dimensions and locations of subchondral cysts. 73 Given the importance of these factors in determining the appropriate treatment, CT scans are helpful for preoperative planning and are likely the study of choice after radiographs demonstrate an osteochondral lesion that may require operative treatment. We recommend a patient-specific approach in choosing advanced imaging and recognize that some lesions may require both MRI and CT to adequately detect, evaluate, and treat them.
Multiple classification systems are based on advanced imaging. These are of historical importance and allow for uniform description of lesions, but they rarely guide treatment. These staging systems do not take lesion size into account, and lesion size is an important factor in determining the appropriate treatment as it has been associated with clinical outcome. Hepple et al 38 developed a classification system based on MRI in 1999. In this classification system, stage I is articular cartilage injury only; stage II is cartilage injury with bony fracture and is further broken down into acute or chronic based on the presence or lack of edema; stage III consists of a detached, nondisplaced bony fragment; stage IV involves displaced bony fragments with uncovered subchondral bone; and stage V lesions involve the presence of a subchondral cyst (Table 1).
Ferkel et al 26 developed a classification system based on CT scan in 1990. In this classification system, stage I entails intact roof/cartilage with a cystic lesion beneath it, stage IIA involves cystic lesions with communication to the surface, stage IIB involves an open surface lesion with an overlying fragment, stage III includes nondisplaced fragments with lucency underneath them, and stage IV lesions include displaced fragments (Table 1).
Despite advances in imaging technology, arthroscopy remains the most effective staging tool as it allows for direct visualization and probing of the lesions, which in turn provides the most complete evaluation to help guide treatment. The arthroscopic grading system is A, smooth and intact but soft; B, rough articular surface; C, fibrillations/fissures; D, flap present or bone exposed; E, loose, nondisplaced fragment; and F, displaced fragment (Table 1). 55
Treatment
The treatment of an OLT depends on the grade of the lesion, its chronicity, and the associated symptoms. Asymptomatic lesions are generally followed with serial radiographs to monitor for progression. Treatment is reserved for lesions that are symptomatic at presentation or become symptomatic. Patients with acute symptomatic lesions that are nondisplaced often are managed with a trial of nonoperative management. This generally consists of a period of 6 weeks of immobilization with a short leg cast or walking boot followed by a slow progression of return to activity. 4,8,54 Nonoperative treatment is effective in roughly 50% of these cases. 11,48 Lesions that become refractory to nonoperative treatment and remain symptomatic for more than 3 to 6 months should be considered for operative treatment. In contrast, acute lesions with displaced fragments should be considered for operative management without a trial of conservative treatment, as they have a lower chance for spontaneous resolution of symptoms. 11 Many operative techniques have been described to treat OLTs. They can be grouped into cartilage repair, cartilage regeneration, and cartilage replacement strategies (Table 2).
Classification of Operative Treatment Options for Osteochondral Lesions of the Talus.

Cartilage Repair Strategies
Cartilage repair strategies include bone marrow stimulation (microfracture) and retrograde drilling. Bone marrow stimulation is often described as the first line of treatment after failure of nonoperative measures. The technique involves perforation of the subchondral bone, allowing infiltration of bone marrow progenitor cells into the lesion (Figure 1). These cells stimulate repair, leading to the formation of fibrocartilage within the defect. Fibrocartilage is composed primarily of type I collagen rather than the type II collagen that makes up the majority of hyaline cartilage, and it is thus biomechanically and structurally inferior to natural cartilage. 52,58 However, this technique produces reliable clinical improvement with reduction of pain and increase in function in 65% to 90% of cases. 18,39,57,60,63

Microfracture technique. (A, B) Debridement of medial talar dome osteochondral lesion of the talus (OLT) to stable margins. (C) Microfracture performed. (D) Marrow elements seen exiting microfracture perforations.
Several factors have been studied as prognostic indicators for the success of bone marrow stimulation, including patient age, lesion chronicity, size, location and containment, and presence of subchondral cysts or associated joint degeneration. OLT size shows an inverse relationship with outcome after microfracture. Chuckpaiwong et al 15 studied 105 osteochondral lesions of the ankle (tibial and talar) treated with ankle arthroscopy, debridement, and microfracture. Lesion size was overwhelmingly correlated with successful outcome. No treatment failures were reported when lesions had an average (longitudinal and transverse) diameter less than 15 mm, while only 1 (3%) patient had a successful outcome with a lesion 15 mm or larger. A corroborative study by Choi et al 14 reported a cutoff of less than 150 mm2 based on MRI imaging for successful clinical outcome. Microfracture remains the gold standard for lesions measuring less than 1.5 cm2.
In addition, older lesions and lesions associated with ankle arthritis have been shown to have less reliable symptom improvement with microfracture than more acute, isolated lesions. 39,41 Lesions with underlying cysts may be associated with worse outcome after microfracture, although the data are mixed in these cases. One study reported a 53% poor clinical outcome with microfracture for cystic lesions, while 2 other studies found no significant difference in outcome scores between patients with cystic or noncystic lesions. 36,57,61 Similarly, data suggest that patients with uncontained (talar shoulder) lesions have worse clinical outcomes with microfracture. 12 Last, several studies have shown no correlation between patient age or lesion location (medial or lateral) with clinical outcomes. 7,12,13
When osteochondral lesions of the talus are associated with subchondral bone defects or cysts with intact overlying cartilage, retrograde drilling is a more effective reparative treatment option than microfracture as it is able to treat the pathology without disturbing the overlying, healthy cartilage. In these types of lesions, retrograde drilling has demonstrated improved patient functional outcomes and lack of lesion degeneration upon second-look arthroscopy. 3,40,41
Cartilage Regeneration Strategies
Cartilage regeneration strategies include autologous chondrocyte implantation (ACI), matrix-induced autologous chondrocyte implantation (MACI), and bone marrow–derived cell transplantation. These techniques are often employed after unsuccessful microfracture treatment or to treat larger lesions that are considered less amenable to microfracture.
ACI is a 2-stage procedure in which hyaline cartilage is harvested from the anterior aspect of the talus or a nonweightbearing portion of the knee in the first stage. 6,51 This cartilage is cultured to grow chondrocytes, which can be viable for longer than 1 year. 50 In the second stage of the procedure, these chondrocytes are delivered into the osteochondral lesion and kept in place by sewing a periosteal patch over the defect (Figure 2). The rationale is that these chondrocytes have the ability to regenerate new hyaline cartilage that can incorporate and fill the chondral lesion.
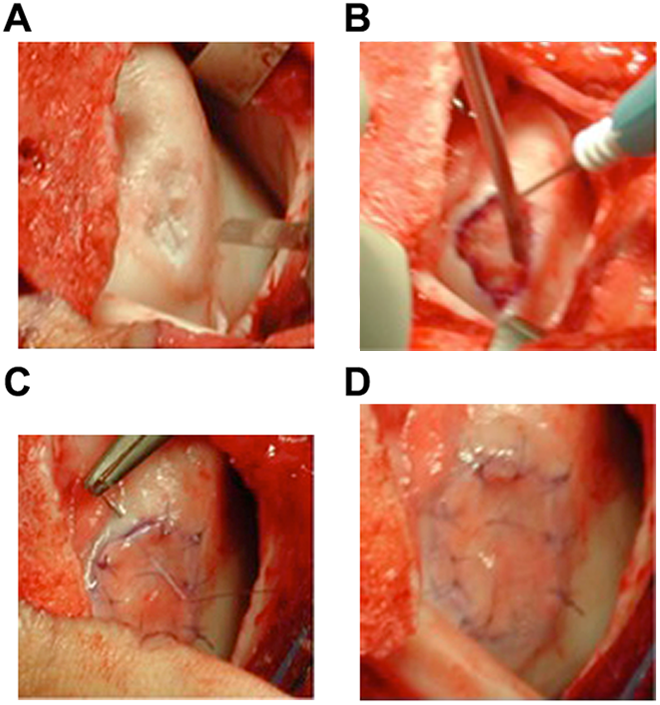
Autologous chondrocyte implantation (ACI). (A) Osteochondral lesion of the talus (OLT) (osteotomy performed). (B) OLT being debrided and chondrocytes being placed. (C) Periosteal patch being sutured over ACI. (D) Fibrin glue overlying ACI.
Favorable results have been reported with ACI. Several groups have reported improved functional outcomes and good to excellent patient-rated outcomes. 5,31,42,51,71 Of note, many of these studies reported these successful outcomes in the treatment of lesions that had previously failed microfracture. Unlike microfracture, lesion size has not been shown to affect the success of ACI. In fact, 1 study evaluating lesions with second-look arthroscopy and MRI found lesion size greater than 137 mm2 and age younger than 26 years to be associated with significantly better modified magnetic resonance scoring system (MOCART) scores. 43 Lesions that are focal and have a stable cartilage rim are more amenable to treatment with ACI. Thus, ACI is often used in lesions greater than 1 to 1.5 cm2 that do not extend into the shoulder.
MACI is a second generation of ACI where the use of a matrix replaces the periosteal patch in securing the implanted autologous chondrocytes. Although the procedure still remains a 2-stage procedure, the use of the matrix reduces operative time and morbidity and theoretically allows for more even chondrocyte distribution within the defect. 9 Outcomes have been favorable with MACI as well, with a meta-analysis reporting a mean success rate of 89% and multiple case series demonstrating increases in functional outcome scores after the use of MACI. 33,62 In addition, second-look arthroscopy has revealed healed articular surfaces, and postoperative MRI has suggested more normal-appearing cartilage tissue in patients undergoing MACI than those undergoing microfracture. 46,53,62
One of the major drawbacks of ACI and MACI is that they are 2-stage procedures. Autologous matrix-induced chondrogenesis (AMIC), which uses bone marrow–derived cells from various sources, attempts to achieve the same goal as ACI or MACI through a 1-step procedure. This technique combines microfracture with autologous iliac crest bone marrow aspirate concentrate (BMAC) or platelet-rich plasma (PRP) delivered on a collagen matrix scaffold in an attempt to form hyaline cartilage in the defect rather than the fibrocartilage that results with microfracture alone. Although data regarding AMIC are difficult to assess due to the variety of techniques it encompasses, the treatment has demonstrated an improvement in functional outcomes and arthroscopic evidence of growth of more normal-appearing hyaline cartilage than microfracture. 28,32,68 Giannini et al 29 compared the results of 56 patients receiving ACI to 25 patients treated with 1-step AMIC. Their group found no difference in the magnitude of improvement in outcome scores and reported similar MRI and second-look arthroscopy outcomes.
Cartilage Replacement Strategies
Cartilage replacement strategies include osteochondral autograft transfer (OAT, proprietary to Arthrex, Naples, FL), osteochondral allograft, and particulated juvenile cartilage allograft transplantation (PJCAT). These treatments are generally for lesions greater than 1 to 1.5 cm2 that are located in the shoulder or do not have a stable cartilaginous rim. OAT techniques involve replacing osteochondral lesions of the talus with hyaline cartilage harvested from the patient’s talus or nonweightbearing portion of the knee. The benefits of this procedure are that the grafts maintain their type II collagen, thus restoring a more normal cartilage surface to the defect. 30 This holds true even when used for defects larger than 3.5 cm2. 34 Several studies have shown improvement in pain and functional outcome scores when using this technique. 23,34,37,64,67 The presence of donor site morbidity remains the most significant disadvantage of this technique. 49,59
Osteochondral allograft transplantation is typically performed for treatment of large uncontained lesions of the shoulder of the talus. Osteochondral allograft transplantation includes both allograft plugs, which can be used as an alternative to autograft plugs, as well as bulk allograft. This technique involves fresh or fresh-frozen grafts harvested from human cadavers from licensed tissue banks. Fresh grafts have been shown to possess increased chondrocyte viability and less cartilage breakdown than fresh-frozen grafts and are thus considered superior. 24,25,72 The donor allograft is size matched on the basis of a CT scan of the recipient talus. This technique allows for treatment of large cystic lesions and has the advantage of being able to restore multiple dimensions of cartilage loss and to treat large lesions without donor site morbidity (Figure 3). It has shown promise, with studies demonstrating improvement in functional outcome scores and patient-reported satisfactory results in lesions with mean sizes as large as 6 cm2. 1,21 However, complications, including resorption, collapse, nonunion, and graft instability, are common. These complications result in a significant rate of failure, with a salvage arthrodesis rate of 13% to 33% in several case series. 10,35,56
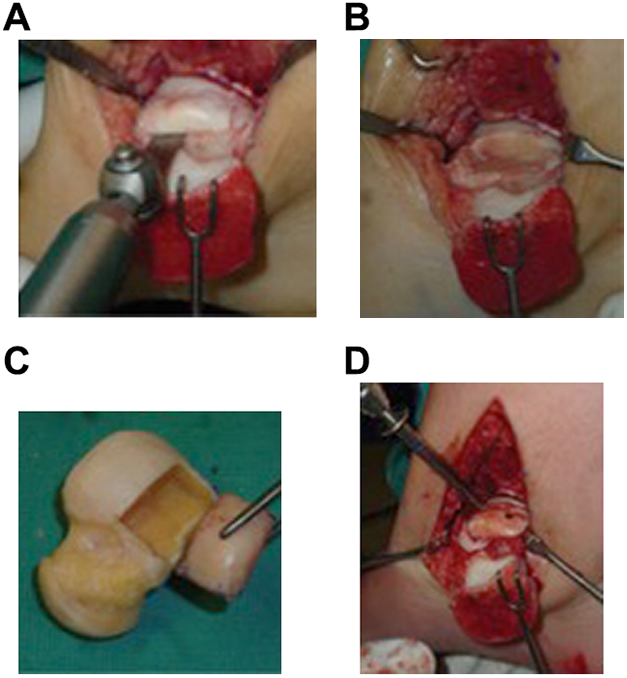
Osteochondral allograft transplantation. (A) Excision of talar shoulder lesion (osteotomy performed). (B) Talus with shoulder lesion removed. (C) Donor allograft with prepared graft removed. (D) Securing graft with 2 screws.
PJCAT involves the transplantation of fresh pieces of juvenile cartilage containing live cells within their natural extracellular matrices. The cartilage is obtained from deceased donors ranging in age from newborns to age 13 years. The particulated nature of the allograft makes delivery feasible through a smaller approach than osteochondral graft, thus, at times, avoiding the need for an osteotomy. It can even be accomplished all arthroscopically. 2 The graft is secured to the osteochondral lesion with fibrin glue in a single-stage procedure that does not have any donor site morbidity (Figure 4). One group presented a retrospective case series of 23 patients with a mean lesion size of 125 mm2 and depth of 7 mm who were treated with PJCAT delivered through both open and arthroscopic approaches. 16 They reported outcomes at follow-up of 16 months for visual analog scale (VAS) pain, American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot, and Foot and Ankle Ability Measure (FAAM) scores that were similar to published outcomes of patients treated with microfracture, ACI, and MACI. Although the indications for the procedure are not yet defined, these authors use PJCAT for lesions that have failed previous bone marrow stimulation or lesions greater than 15 mm in diameter. Although it is feasible to bone graft under particulated juvenile cartilage, the authors prefer structural allograft if significant bone grafting is needed. Disadvantages of PJCAT at this time include limited supply of allograft, the theoretical risk of disease transmission, and the lack of long-term data.

Particulated juvenile cartilage allograft transplantation. (A) Unstable medial talar dome osteochondral lesion of the talus. (B) Lesion debrided to stable margins. (C) Particulated juvenile cartilage allograft pieces were placed into the lesion bed. (D) The cartilage pieces were covered with fibrin glue.
Future Considerations
Although the many operative treatment options detailed above show promise in reducing the morbidity associated with osteochondral lesions of the talus, the data supporting these treatments largely come from smaller case series rather than comparative outcome studies or randomized controlled trials. As such, no strict criteria exist to help guide orthopaedic surgeons to the optimal treatment, and treatment must be tailored to each individual lesion and patient. In general, increasing lesion size is the most objective measurement, with increasing lesion size often requiring more advanced regenerative or replacement techniques rather than reparative ones. The presence of subchondral cysts and whether the lesion extends into the shoulder are other important considerations. Our algorithm for operative treatment choice is detailed in Figure 5. However, more comparative studies and randomized controlled trials are needed to better elucidate which treatment options are more effective for certain types of lesions and patients.

Algorithm for treatment of osteochondral lesions of the talus (OLTs). ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; MACI, matrix-induced autologous chondrocyte implantation; OAT, osteochondral allograft transplantation; PJCAT, particulated juvenile cartilage allograft transplantation.
In addition, more research is needed surrounding pathophysiology of osteochondral lesions of the talus. This may allow for the development of improved treatments and preventive treatment options to help decrease the incidence of OLTs. For example, injectable treatments that target the inflammatory cascade or promote natural chondrocyte repair or regeneration may be a future option to help prevent the development of OLTs after acute ankle injury.
Conclusion
Osteochondral lesions of the talus encompass a variety of pathologies that can cause significant morbidity to patients. Trauma is the most common cause for the development of these lesions, but OLTs can arise atraumatically as well. Patients typically present with nonspecific signs and symptoms such as effusion, pain, and decreased range of motion. Thus, clinicians must have a high index of suspicion to diagnose these lesions, and advanced imaging techniques are often required. Nondisplaced OLTs are often initially treated conservatively with protected weightbearing; however, a large percentage of patients will remain symptomatic and require operative treatment. There are a variety of operative techniques available to treat OLTs. These can be categorized into cartilage repair, cartilage regeneration and cartilage replacement techniques. Research shows promise with many of these techniques in reducing symptoms associated with the lesions. Given the lack of comparative outcomes research in the field, there are no specific criteria to direct orthopedic surgeons to the optimal option, and treatment must be tailored to each individual patient. More research is needed to elucidate which treatment options are superior and for which types of patients and lesions they should be directed.
Supplemental Material
Supplemental Material, FAO779559-ICMJE - Osteochondral Lesions of the Talus: Current Concepts in Diagnosis and Treatment
Supplemental Material, FAO779559-ICMJE for Osteochondral Lesions of the Talus: Current Concepts in Diagnosis and Treatment by John R. Steele, Travis J. Dekker, Andrew E. Federer, Jordan L. Liles, Samuel B. Adams, and Mark E. Easley in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.