
Abstract
Background:
After rotator cuff repair, some patients have ongoing problems significant enough to warrant presentation to a clinic for reassessment.
Purpose/Hypothesis:
The purpose of this study was to determine whether this cohort of patients was more likely to have a healed rotator cuff. We hypothesized that patients who had an unscheduled postoperative visit were more likely to have a healed rotator cuff than those who did not have an unscheduled postoperative visit.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 321 consecutive patients who underwent arthroscopic rotator cuff repair were evaluated; of these, 50 patients had an unscheduled return to clinic that included an ultrasound assessment of the cuff repair within 4 months postoperatively. Repair integrity was evaluated in all patients at 6 months postoperatively via ultrasonography.
Results:
The failure-to-heal rate was greater in patients who had an unscheduled assessment (8/50; 16%) than in those who did not (14/275; 5%) (P = .01). The patients most likely to have a repair failure were those who were assessed before 2 weeks and after 12 weeks (7/18; 39%) compared with those who were assessed between 3 and 12 weeks (1/32; 3%) (P = .001). The failure-to-heal rate was very low in patients who had an unscheduled assessment with a tear size smaller than 4 cm2 (0/34; 0%) compared with those with tear sizes greater than 4 cm2 (8/16; 50%) (P < .0001, Fisher exact text).
Conclusion:
Patients who had an unscheduled clinic visit after rotator cuff repair had a 16% chance of a failed healing response, whereas those who did not have an unscheduled visit had a 5% rate of failed healing. The risk of a failed healing response was greater if the tear was larger than 4 cm2, if patients presented within 2 weeks following surgery, or if they presented after 12 weeks postsurgery.
Rotator cuff tears are among the most common disorders affecting the shoulder. Patients with torn rotator cuffs often experience pain and difficulty with overhead activities. Surgical reattachment of the torn tendons is generally recommended for symptomatic full-thickness rotator cuff tears, 5 and arthroscopic rotator cuff repair has been regarded as an effective procedure with respect to providing patient satisfaction, restoring functional capacity, and reducing pain. 1,15,16 Some patients continue to have persistent pain or experience trauma to their shoulder after their rotator cuff repair and may visit their physician for reassessment, concerned that they have retorn their rotator cuff. At our institute, the standard practice in this scenario is to perform a follow-up ultrasound assessment to assess rotator cuff integrity postoperatively. 13 However, to our knowledge, the prognosis of patients presenting in this fashion is unknown.
The purpose of this study was to determine whether patients who underwent unscheduled examination and ultrasonography were more likely to have healed tendons or more likely to have retorn their rotator cuff. We hypothesized that patients who had an unscheduled postoperative visit were more likely to experience healing of their repair compared with patients who followed the normal course of recovery.
Methods
Following ethics approval at our institution, we performed a retrospective study involving prospectively collected data.
Inclusion and Exclusion Criteria
Patients were included in this study if they had undergone arthroscopic repair of a primary rotator cuff tear (defined as any tear that had not previously been surgically treated) and had an ultrasound examination within 6 months postoperatively to determine repair integrity. Excluded were those who had an isolated subscapularis tear; rotator cuff repair with an interpositional polytetrafluoroethylene (PTFE) patch; revision or partial rotator cuff repair; irreparable rotator cuff tear; glenohumeral arthritis (of grade 2 or greater); concurrent fracture of the humerus, scapula, or clavicle; arthroplasty; arthroscopic glenohumeral joint stabilization; biceps tenodesis; calcific debridement; or other concurrent procedures.
Grouping of Patients
Post hoc, patients were assigned to the “early ultrasound group” if, because of pain, they had an unscheduled postoperative assessment and ultrasound examination within 4 months of their rotator cuff repair. The control group consisted of all patients who did not have an unexpected postoperative appointment or ultrasound examination during the same time period but had a routine ultrasound assessment of their repair at 6 months postoperatively.
Operative Procedure and Rehabilitation
Operative procedures and rehabilitation were performed as previously described by McNamara et al. 12
Following appropriate visualization, intra-articular assessment, and location of the tendon tear with an arthroscope, tears were debrided and partial-thickness tears were converted to full-thickness tears by use of an arthroscopic shaver (either 4.0 or 5.5 mm in diameter). Repairs were visualized from within the glenohumeral joint (undersurface 19 ), from within the subacromial bursa (bursal 18 ), or via both approaches. Repair was conducted with sutures and knotless suture anchors (OPUS SmartStitch and OPUS Magnum-2 knotless anchor; ArthroCare) in a single-row inverted mattress configuration. No acromioplasty, coracoacromial ligament release, or bursectomy was performed in undersurface repairs. Anteroposterior and mediolateral tear measurements were calculated intraoperatively by visually comparing the known diameter of the shaver with the tear. Before and after partial-thickness tears were converted to full-thickness tears, tear thickness was estimated on visualization of the torn area, whereby a full-thickness tear was denoted as 100% torn.
Postoperatively, the patients were immobilized for 6 weeks with use of a sling with a small abduction pillow (UltraSling; DJO Global). Patients completed a progression of rehabilitation exercises closely monitored by their physical therapist for 4 to 6 months. They followed a standardized, gradually progressive, home rehabilitation program. 7 Pendulum exercises were started on the first day after surgery. On postoperative day 8, passive forward flexion, external rotation, and abduction exercises of the shoulder were begun. At 6 weeks, active shoulder motion and isometric strengthening were started. At 12 weeks postoperatively, patients were allowed to commence overhead activities and lift more than 5 kg of weight. They were encouraged to return to full activities at 6 months. Patients were prohibited from taking any nonsteroidal anti-inflammatory medications for 6 months postoperatively.
Patient Assessment
All aspects of patient assessment, including preoperative assessment, shoulder function, range of motion, and strength, were performed as previously outlined 12 at 1 week, 6 weeks, 12 weeks, and 6 months postoperatively. Ultrasound examination was routinely conducted preoperatively and 6 months postoperatively. Patients who required an unscheduled postoperative visit to the clinic (ie, the early ultrasound group) received an additional ultrasound examination and clinical assessment at that time.
Preoperative Assessment
At initial presentation, each patient completed a questionnaire that asked when the problem began, whether it was related to a specific traumatic injury, and whether it was work related.
Shoulder Function
In addition to the above, patients completed a standardized questionnaire that was based on the L’Insalata Shoulder Rating Questionnaire 9 and appraised patient-ranked shoulder stiffness using a Likert scale (ranked as “not at all,” “a little,” “moderately,” “quite,” and “very” and scored from 0 to 4). The questionnaire was completed preoperatively and at 1 week, 6 weeks, 12 weeks, and 6 months postoperatively.
Range of Motion
Examiners measured passive shoulder range of motion preoperatively and at 6 weeks, 12 weeks, and 6 months postoperatively. The ranges of external rotation, forward flexion, abduction, and internal rotation were determined visually according to a previously validated protocol. 14 The examiners were not blinded to patients’ operative and clinical data.
Shoulder Strength
Examiners tested the strength of shoulder external rotation, internal rotation, adduction, lift-off, and abduction in the scapular plane (supraspinatus) with a handheld dynamometer according to validated protocols 4 preoperatively and at 6, 12, and 24 weeks postoperatively.
Rotator Cuff Integrity
Ultrasound examination of the rotator cuff was performed at 6 months postoperatively by a single experienced musculoskeletal ultrasonographer who was blinded to the clinical results. 3,8 Real-time ultrasound examination was performed using either a Logiq 9 or Logiq E9 machine (General Electric) with a 12-MHz linear transducer according to a standardized protocol, and the location, size, and thickness of any tear of the rotator cuff were recorded on a standardized form. 3 A failure to heal was defined as a rotator cuff repair with an identifiable hypoechoic gap on ultrasonography. This assessment was made irrespective of the original tear size. 3,8,17
Statistical Analysis
Comparisons were made within the overall cohort and within the respective early ultrasound and control groups by use of Pearson chi-square test. Comparisons between the early ultrasound and control groups were made at each time point using unpaired Student t test for continuous variables that had a normal distribution and Mann-Whitney tests for categorical data. In the subgroup analysis, a Fisher exact test for dichotomous data was conducted to determine whether the independent variable affected the dependent variable. Bivariate Pearson and Spearman tests for correlation were conducted to determine a relationship between different variables taken from the preoperative, intraoperative, and postoperative data for the overall cohort. Multiple logistic regression analysis was performed to identify variables that independently affected rotator cuff healing and shoulder pain in the overall cohort. For the respective analyses, repair integrity and examiner-assessed range of motion were the dependent variables, and all demographic and preoperative, patient-ranked, examiner-assessed strength and intraoperative data already previously mentioned were included as potential independent variables. The level of significance was set at P < .05 for all statistical analyses.
Results
Patient Demographics
Between July 2013 and December 2016, a total of 654 consecutive arthroscopic rotator cuff repairs were performed by a single surgeon (G.A.C.M.). Of these, we excluded 4 for isolated subscapularis tears; 73 for rotator cuff repair with an interpositional PTFE patch; 84 for revision rotator cuff repair; 40 for the presence of glenohumeral arthritis that was grade 2 or greater; 9 for concurrent fracture of the humerus, scapula, or clavicle; 27 for concurrent shoulder arthroplasty; 18 for concurrent glenohumeral stabilization; 32 for concurrent calcific debridement; 7 for concurrent biceps tenodesis; 24 for other concurrent procedures; and 11 for incomplete data. This left a study cohort of 321 patients and a total of 325 shoulders.
There were 189 male and 132 female patients, with a mean ± standard error of the mean (SEM) age of 59.2 ± 0.9 years (range, 30-91 years). Intraoperatively, 63% of the shoulders were noted to have a full-thickness tear and 37% had a partial-thickness tear, with a mean tear-size area of 3.3 ± 0.5 cm2 (range, 0.3-25 cm2). An undersurface 19 repair technique was used in 74% of the repairs, while 19% were bursal 18 and 4% required both approaches. The average number of anchors needed for repair was 2 (range, 1-7). The mean operative time, defined as the time from initial incision to when the final suture anchor was deployed and cut, was 15 ± 0.6 minutes (range, 4-100 minutes). The overall nonhealing rate was 6.8% (22 failures to heal out of 325 repairs).
Of the 325 shoulders in the study, there were 275 in the control group and 50 in the early ultrasound group. No significant differences were found between the 2 groups with regard to age, sex, tear size, tear thickness, operative time, or anchors (Table 1). The average time for patients in the early ultrasound group to return for a repeat ultrasound assessment was 9 ± 5 weeks (range, 1-17 weeks). Thirty-one of the 50 patients in the early ultrasound group presented after experiencing a traumatic incident to their shoulder.
Characteristics of the 2 Study Groups a
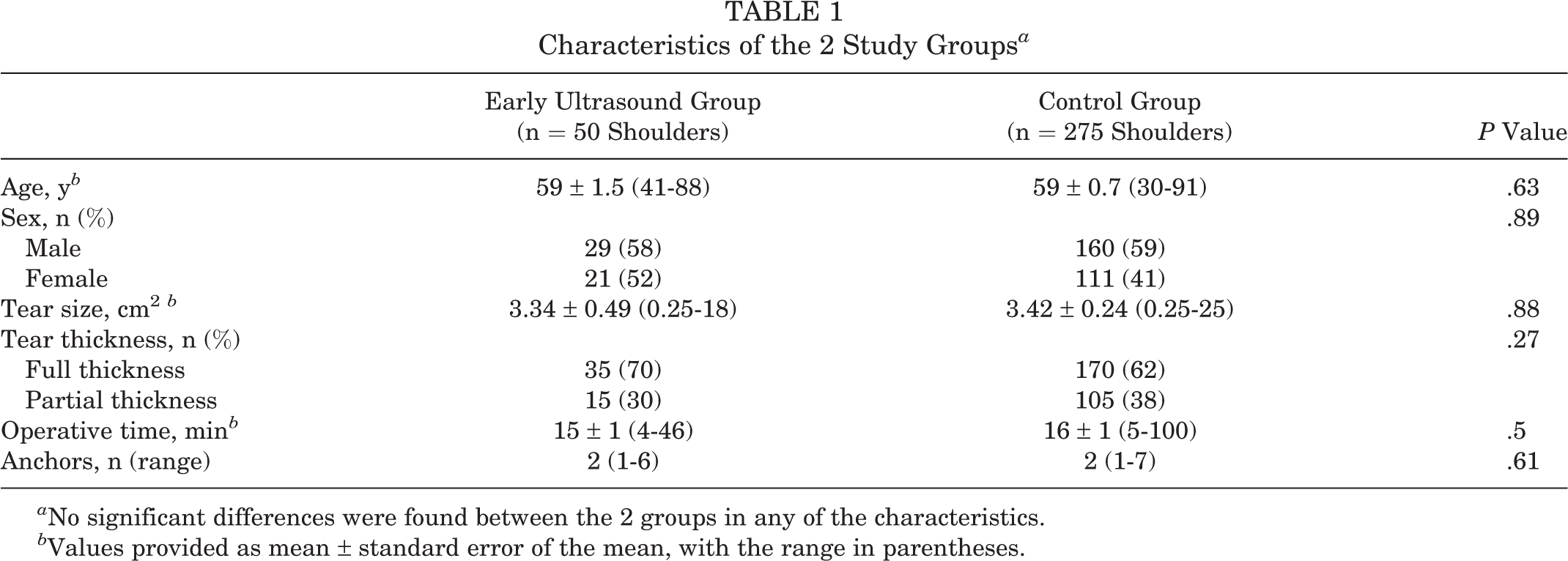
a No significant differences were found between the 2 groups in any of the characteristics.
b Values provided as mean ± standard error of the mean, with the range in parentheses.
Repair Integrity
Nonhealed repairs were found in 16% (8/50) of the shoulders in the early ultrasound group and 5% (14/275) of the shoulders in the control group by 6 months postoperatively (P = .01) (Figure 1). For the entire cohort, the average time for identification of the patient’s loss of repair integrity was 16 weeks postoperatively. Thirty-one of the 50 patients in the early ultrasound group reported a traumatic incident prior to their unscheduled visit; 4 of these 31 patients had a nonhealed repair. In the remaining 19 patients who did not report a traumatic incident prior to their unscheduled postoperative visit, there were 4 nonhealed repairs (P = .46).

Failure-to-heal rate in the control group and the early ultrasound group. *P < .05, Fisher exact test.
Failure to Heal Within the Early Ultrasound Group
Although the patients in the early ultrasound group underwent ultrasound assessments at various times within 4 months of their operation, the nonhealing rate was highest in those assessed between 13 and 16 weeks and before 2 weeks (Figure 2). By 6 months, only 1 of 32 patients who presented between 3 and 12 weeks had failure to heal. Patients presenting between 3 and 12 weeks (1/32; 3%) had a significantly lower nonhealing rate compared with those presenting between 13 and 16 weeks (5/11; 45%) (P = .0005) and before 2 weeks (2/7; 29%) (P = .02).
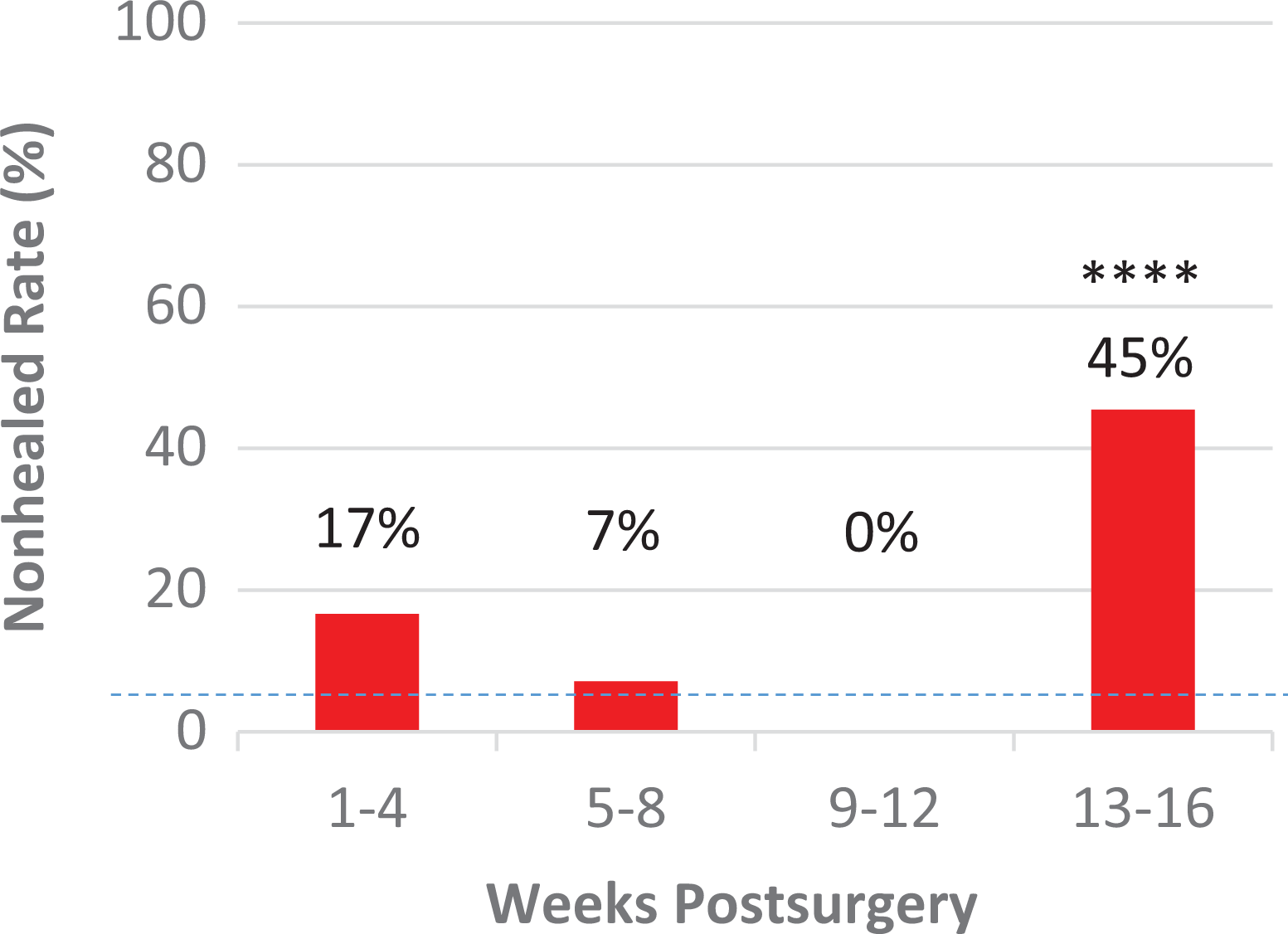
Relationship between failure-to-heal rate and time elapsed before patients in the early ultrasound group had an unscheduled visit to the clinic. The dashed line represents the failure-to-heal rate in the control group (5%) for comparison. ****P < .0001 compared with control group, Fisher exact test.
Within the early ultrasound group, patients who had a failed repair had larger tear sizes on average (7 ± 0.8 cm2) than those whose repairs healed (3 ± 0.5 cm2) (P = .0003). This was further exemplified by the correlation between failure to heal and tear size (r = 0.516, P = .0001). For tear areas smaller than 4 cm2, both the early ultrasound group (0 failures to heal out of 34 shoulders) and the control group (3 repair failures out of 193 shoulders) had low incidences of nonhealing. However, for patients with tear areas larger than 4 cm2, those in the early ultrasound group (8/16; 50%) had a higher failure-to-heal rate than patients in the control group (11/80; 14%) (P = .01) (Figure 3). Of the 5 patients presenting between 13 and 16 weeks who had tendons that did not heal, the average tear size was 7 cm2, while the remaining 6 patients who presented between 13 and 16 weeks had an average tear size of 2 cm2.

Frequency distribution of tear sizes within (A) the early ultrasound group and (B) the control group and the amount of repair failure within each range of tear sizes. The labels within the columns represent the nonhealing rate within that range of tear size. *P < .05 when comparing the columns in the early ultrasound group to its corresponding column(s) in the control group via Fisher exact test.
Pain
When asked, “How is your shoulder overall?” patients in the early ultrasound group reported lower levels of overall satisfaction with their shoulder compared with those in the control group, especially from 6 weeks postoperatively (P = .03) (Figure 4A).

Comparison between the early ultrasound (US) group and the control group: (A) overall patient satisfaction with the shoulder, (B) frequency of extreme pain, (C) frequency of pain during activities, (D) level of pain at rest, and (E) level of pain during overhead activities. For patient satisfaction, 0 = very bad and 4 = good; for pain frequency, 0 = never and 4 = always; for levels of pain, 0 = none and 4 = very severe. *P < .05, **P < .01, ***P < .001, ****P < .0001.
Compared with the control group, the early ultrasound group tended to experience pain more often. Patients in the early ultrasound group had a higher frequency of extreme pain at 1 week (P = .02), 6 weeks (P = .004), 12 weeks (P < .002), and 6 months (P < .0001) (Figure 4B). Patients in this group also experienced greater frequency of pain during activities at 6 weeks (P = .04), 12 weeks (P = .04), and 6 months (P < .0001) (Figure 4C). In addition, the early ultrasound group had greater levels of pain at rest at 1 week (P = .04), 6 weeks (P = .004), and 6 months (P = .02) (Figure 4D) and also had greater levels of pain with overhead activities at 6 weeks (P = .01), 12 weeks (P = .0006), and 6 months (P < .0001) (Figure 4E).
Examiner-Assessed Passive Range of Motion
In general, the control group acquired greater range of motion than the early ultrasound group over the course of the postoperative period. By 12 weeks, the control group had greater range of motion in abduction (P = .03) (Figure 5A), external rotation (P < .01) (Figure 5B), and forward flexion (P = .0029) (Figure 5C). At 6 months, the difference between the groups widened further as the control group had greater range of motion in abduction, external rotation, and forward flexion (P < .0001 for all).

Comparison of passive range of motion between the early ultrasound (US) group and the control group in (A) abduction, (B) external rotation, and (C) forward flexion. *P < .05, **P < .01, ***P < .001, ****P < .0001, Mann-Whitney U test.
Strength
By 12 weeks, the control group was stronger in external rotation than the early ultrasound group (P = .02). At 6 months, the control group had greater strength in supraspinatus abduction testing (P = .003) (Figure 6A), adduction (P = .005), lift-off testing (P = .04), and external rotation (P = .02) (Figure 6B).
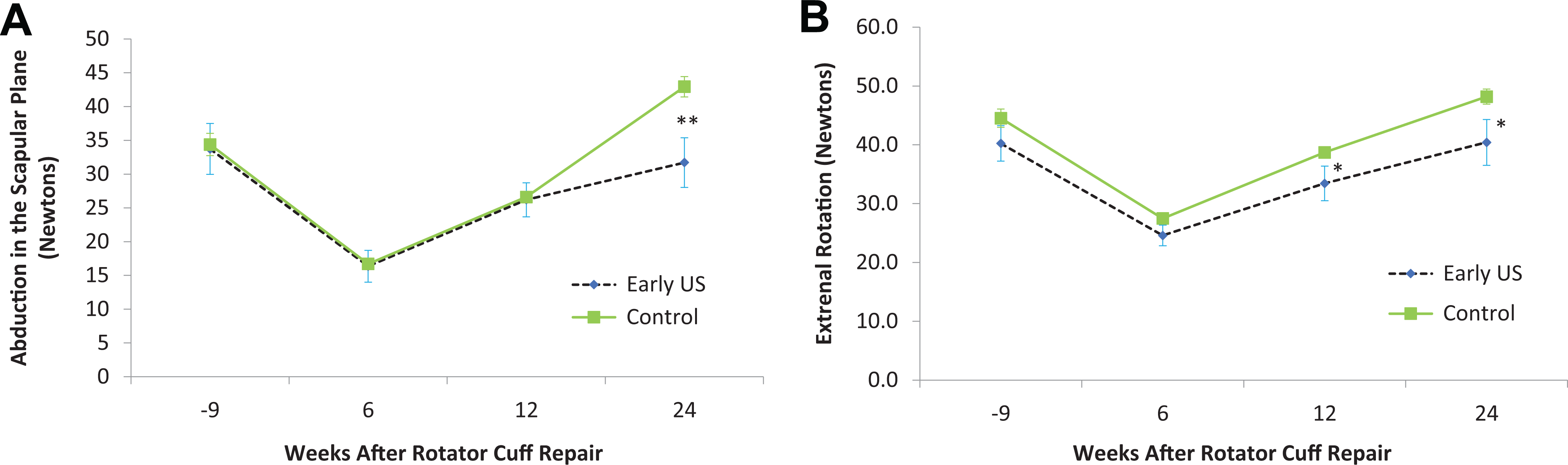
Comparison of strength between the early ultrasound (US) group and the control group in (A) abduction in the scapular plane and (B) external rotation. *P < .05, **P < .01.
Discussion
This study evaluated the clinical outcomes of patients who underwent arthroscopic rotator cuff repair and had an unscheduled clinic visit during their first 4 months postoperatively. No specific instructions were provided to induce these patients (16% of our study cohort) to present for an unscheduled visit. On average these patients experienced more frequent and severe pain and lower overall satisfaction with the status of their shoulders compared with those who did not have an unscheduled visit. We did not analyze other potential factors for an unscheduled visit, such as distance from the clinic or workers’ compensation status. In this group, there was a low incidence of loss of rotator cuff repair integrity in patients who had a tear area smaller than 4 cm2 (0/34; 0%) and who presented between 3 and 12 weeks (1/32; 3%). However, of patients with unscheduled clinic visits, those who presented to clinic earlier, between 0 and 2 weeks (2/7; 29%), or later, between 13 and 16 weeks (5/11; 45%), had higher rates of nonhealing compared with the overall cohort nonhealing rate of 7%. Furthermore, of those who had an unscheduled clinic visit, patients with a tear size larger than 4 cm2 were much more likely to have failure of the repair at 6 months following surgery (8/16; 50%) in contrast to those with a tear size smaller than 4 cm2 (0/34; 0%).
To our knowledge, this is the first study to analyze repair integrity in patients who return to clinic postoperatively with concerns about their shoulder. Yeo et al 21 found that postoperative pain at 6 weeks, 3 months, and 6 months was positively associated with smaller tears and higher rates of tendon healing. However, increased pain levels before 2 weeks or between 12 and 16 weeks may be a sign of a nonhealed cuff repair.
The low failure-to-heal rate (3%) in those presenting between 3 and 12 weeks with pain is consistent with the hypothesis that between 6 weeks and 3 months, a proliferative healing response occurs along with higher levels of neoangiogenesis, a known marker of tendon healing, which is accompanied by proliferation of pain-sensitive nerve fibers. 11,20 Moreover, in those presenting to clinic between 3 and 12 weeks, the only repair failure occurred in a patient who had a tear size of 9 cm2, who stopped using his immobilization sling after only 2 weeks (against standard protocol) and who chose to take anti-inflammatory medications to self-treat his shoulder pain. All 3 of those factors were potentially important contributors to the failure of his tendon to heal.
The relationship between tear size and repair integrity has been well documented in previous studies 2,6,10 and is consistent with our results. The current study also showed that larger tear size was an important factor in failure to heal. In the patients in our cohort with tears larger than 4 cm2, there were 19 repair failures out of 96 shoulders (20%); for tears smaller than 4 cm2, there were 3 failures in 229 shoulders (1.3%). Larger tear size also may explain why the failure-to-heal rate was high in patients presenting between 13 and 16 weeks and within 2 weeks. Patients returning between 13 and 16 weeks with a nonhealed tendon had an average tear size of 7 cm2, compared with 2 cm2 in the 5 patients of this subgroup whose tendons were intact. Furthermore, in this subgroup, 5 of the 11 patients had tear sizes larger than 4 cm2, and all 5 of these patients had a repair failure. Also at risk were those who presented within 2 weeks of their repair and had a larger tear; the 2 patients who had a loss of repair discovered at 2 weeks had tear sizes of 6 cm2 and 8 cm2.
An important limitation of this study was its retrospective cohort design. Furthermore, only 50 patients were sampled in the experimental group. A larger sample size may have increased the chance of acquiring further statistically significant results during multiple logistic regression analysis and multivariate analysis while also reducing type II errors. Furthermore, the ultrasonographer was not blinded to the fact that certain patients had an unscheduled visit. Another limitation was that workers’ compensation status, distance to clinic, and other demographics were not analyzed, as they may have affected the patients’ decision to present for an unscheduled postoperative visit. Finally, the fact that the surgeries were performed primarily by one surgeon and the ultrasound assessments were interpreted by one ultrasonographer may affect the applicability of our results to other clinics and hospitals.
The strengths of this project included the clear inclusion and exclusion criteria and the organized, standardized collection of patient-ranked and examiner-assessed data for every patient. Furthermore, all ultrasound assessments were performed by one experienced shoulder ultrasonographer, and all surgeries were performed by a single, skilled surgeon, which enhances the study’s internal validity.
Conclusion
This study shows that patients who have an unscheduled postoperative visit due to pain tend to have a higher nonhealing rate than those who follow the normal course of recovery. However, of those who had an unscheduled postoperative visit, the patients presenting before 2 weeks and between 13 and 16 weeks, and those with a tear larger than 4 cm2, were more likely to have a nonhealed rotator cuff by 6 months after surgery. In contrast, patients who had an unscheduled postoperative visit between 3 and 12 weeks (97% intact) and who had tears smaller than 4 cm2 (100% intact) had a higher chance of having an intact rotator cuff at 6 months postoperatively.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: G.A.C.M. has stock/stock options in National Day Surgery–Sydney, is a paid consultant for Smith & Nephew, and receives research support from Smith & Nephew.
Ethical approval for this study was obtained from the SESLHD Hospital Human Research Ethics Committee.