
Abstract
Background:
Hip and groin pain is a common complaint among athletes. Few studies have examined the epidemiology of hip and groin injuries in collegiate athletes across multiple sports.
Purpose:
To describe the rates, mechanisms, sex-based differences, and severity of hip/groin injuries across 25 collegiate sports.
Study Design:
Descriptive epidemiology study.
Methods:
Data from the 2009-2010 through 2013-2014 academic years were obtained from the National Collegiate Athletic Association Injury Surveillance Program (NCAA ISP). The rate of hip/groin injuries, mechanism of injury, time lost from competition, and need for surgery were calculated. Differences between sex-comparable sports were quantified using rate ratios (RRs) and injury proportion ratios (IPRs).
Results:
In total, 1984 hip/groin injuries were reported, giving an overall injury rate of 53.06 per 100,000 athlete-exposures (AEs). An adductor/groin tear was the most common injury, comprising 24.5% of all injuries. The sports with the highest rates of injuries per 100,000 AEs were men’s soccer (110.84), men’s ice hockey (104.90), and women’s ice hockey (76.88). In sex-comparable sports, men had a higher rate of injuries per 100,000 AEs compared with women (59.53 vs 42.27, respectively; RR, 1.41 [95% CI, 1.28-1.55]). The most common injury mechanisms were noncontact (48.4% of all injuries) and overuse/gradual (20.4%). In sex-comparable sports, men had a greater proportion of injuries due to player contact than women (17.0% vs 3.6%, respectively; IPR, 4.80 [95% CI, 3.10-7.42]), while women had a greater proportion of injuries due to overuse/gradual than men (29.1% vs 16.7%, respectively; IPR, 1.74 [95% CI, 1.46-2.06]). Overall, 39.3% of hip/groin injuries resulted in time lost from competition. Only 1.3% of injuries required surgery.
Conclusion:
Hip/groin injuries are most common in sports that involve kicking or skating and sudden changes in direction and speed. Most hip/groin injuries in collegiate athletes are noncontact and do not result in time lost from competition, and few require surgery. This information can help guide treatment and prevention measures to limit such injuries in male and female collegiate athletes.
Hip and groin pain is a common complaint among athletes of all ages and has been estimated to account for 5% to 6% of all sports injuries. 31,49 The cause of hip and groin pain is often multifactorial, including bony and soft tissue abnormalities that can occur intra- or extra-articularly in both the acute and chronic overuse settings. 4,13,20,35,49 A study by Packer and Safran 47 in 2015 suggested that there may be a genetic predisposition toward hip abnormalities, with white patients noted to have higher rates of hip injuries, such as femoroacetabular impingement (FAI), than Asian patients. Additionally, there is evidence that younger athletes participating in high-impact sports have an increased risk of developing cam-type deformities and eventual osteoarthritis. 3,42 Historically, many hip injuries in athletes have been neglected because of a lack of specific diagnostic criteria and undefined treatment modalities. 13 However, recent developments in magnetic resonance arthrography, hip arthroscopic surgery, and biomechanics have led to advances in the diagnosis and treatment of nonarthritic hip and groin conditions. 13,35 Additionally, recent studies on hip and groin diseases such as FAI and athletic pubalgia have demonstrated improved surgical outcomes. 24,31,52,57 The advancement in our understanding of hip and groin pathoanatomy, in addition to improved treatment modalities, has generated an increased interest in research related to hip injuries in young athletes.
Despite promising developments, there are still many factors complicating our understanding of the epidemiology of hip injuries. One major issue is the difficulty of diagnosis, particularly in the acute setting, because many hip disorders present with overlapping signs and symptoms that are nonspecific and difficult to assess. 4,49,52 Complex pathomechanical interactions within the hip joint and the central watershed location of the hip often result in a vague clinical picture without an obvious diagnosis. 20 Athletes can also develop a compensatory secondary dysfunction such as trochanteric bursitis, which further complicates the clinical picture. 13 Additionally, the role that sports participation plays in the development of chronic hip and groin injuries remains unclear, with some studies indicating that hip pathoanatomy may be influenced by sports participation during adolescence. 30,43,56 More research on the nature and patterns of hip injuries in young athletes is necessary to provide better options for prevention, earlier diagnosis, and more effective treatment modalities.
Prior studies have examined the biomechanical demands placed on athletes to determine which sports are more likely to cause athletic hip injuries. 7,14,18,20,43 There have also been epidemiological studies of hip injuries in athletes in all 4 of the major American sports (baseball, football, basketball, and ice hockey). 9,15,16,28 To our knowledge, however, a large epidemiological study of hip injuries in college athletes in the United States has not been previously undertaken. The identification of hip abnormalities in younger athletes is important, as it allows for early detection and intervention that may slow or prevent the progression to advanced stage disease. An enhanced understanding of the epidemiology of hip injuries in college-aged athletes is therefore critical. The purpose of this study was to describe the epidemiology of hip injuries occurring within the National Collegiate Athletic Association (NCAA) during the 2009-2010 through 2013-2014 academic years using the NCAA Injury Surveillance Program (ISP).
Methods
After obtaining institutional review board exemption from Drexel University, this study was approved by the NCAA Research Review Board. Data were obtained from the Datalys Center for Sports Injury Research and Prevention, an independent nonprofit research organization that manages the NCAA ISP. More in-depth information regarding the methods of the NCAA ISP during the 2009-2010 through 2013-2014 academic years has been previously described 33 and are summarized below.
Data Collection
ISP data were derived from a sample of amateur varsity sports teams that voluntarily participated in the data collection. Participating institutions included all collegiate levels (Divisions I-III). The proportion of NCAA member schools that reported data to the ISP varied by sport, ranging from 0.66% in men’s tennis (5/760 schools) to 13.24% in men’s ice hockey (18/136 schools). 33 At participating programs, an athletic trainer (ATC) reported injury data to the Datalys Center either via his or her school’s own electronic health records or the Datalys Center’s in-house injury surveillance tool. Of note, the 2009-2010 through 2013-2014 data set used in this project included non–time-loss (NTL) injuries, unlike prior datasets that only included injuries resulting in time loss (TL).
For each injury event, the ATC filled out a standardized reporting document that included detailed information on all the variables describing the injury and exposure, such as the number of athletes participating in the session, event type (ie, competition or practice), body part, and mechanism of injury. The mechanism of injury was selected from a preset list of options, including player contact, surface contact, equipment contact, contact with an out-of-bounds object (eg, wall or fence), no apparent contact (ie, rotation about planted foot), overuse, and other/unknown. The ATC also logged any time lost from competition and whether the athlete required surgery. Of note, there was no routine confirmation of the injury diagnosis by a physician.
After all the data were recorded, they were then deidentified and transferred to an aggregate database hosting all national data. Multiple human and automated verification processes were used to ensure that data were consistent and no invalid values were included. For this study, data were pooled from all the sport-specific data sets to provide information on hip and groin injuries in the NCAA ISP database.
Definitions
A reportable injury in the ISP was defined as an injury that (1) occurred as a result of participation in an organized intercollegiate practice or competition and (2) required attention from an ATC or physician. 33 A reportable athlete-exposure (AE) was defined as 1 student-athlete participating in 1 NCAA-sanctioned practice or competition in which he or she was exposed to the possibility of an athletic injury, regardless of the time associated with that participation. 33 The data included all preseason, regular-season, or postseason practices or competitive games. Any injuries and exposures that occurred outside of these times, such as during summer conditioning or individual workouts, were excluded.
Statistical Analysis
Data were analyzed using Excel 2016 software (Microsoft). Statistical analyses included calculation of the overall rate of hip injuries, the rate of hip injuries in each individual sport in both competition and practice, and the rate of injuries across sex-specific sports. These rates were calculated as the ratio of injuries per 100,000 AEs. Rate ratios (RRs) and injury proportion ratios (IPRs) were calculated to quantify the differences in injury rates between each sex-specific sport and in competition versus practice; 95% CIs were calculated to assess statistical significance, with any CI not containing the value 1.00 considered statistically significant. Further calculations investigating the mechanism of injury, time lost from competition, and need for surgery across sports and sexes were also performed.
Results
Overall Frequencies and Rates
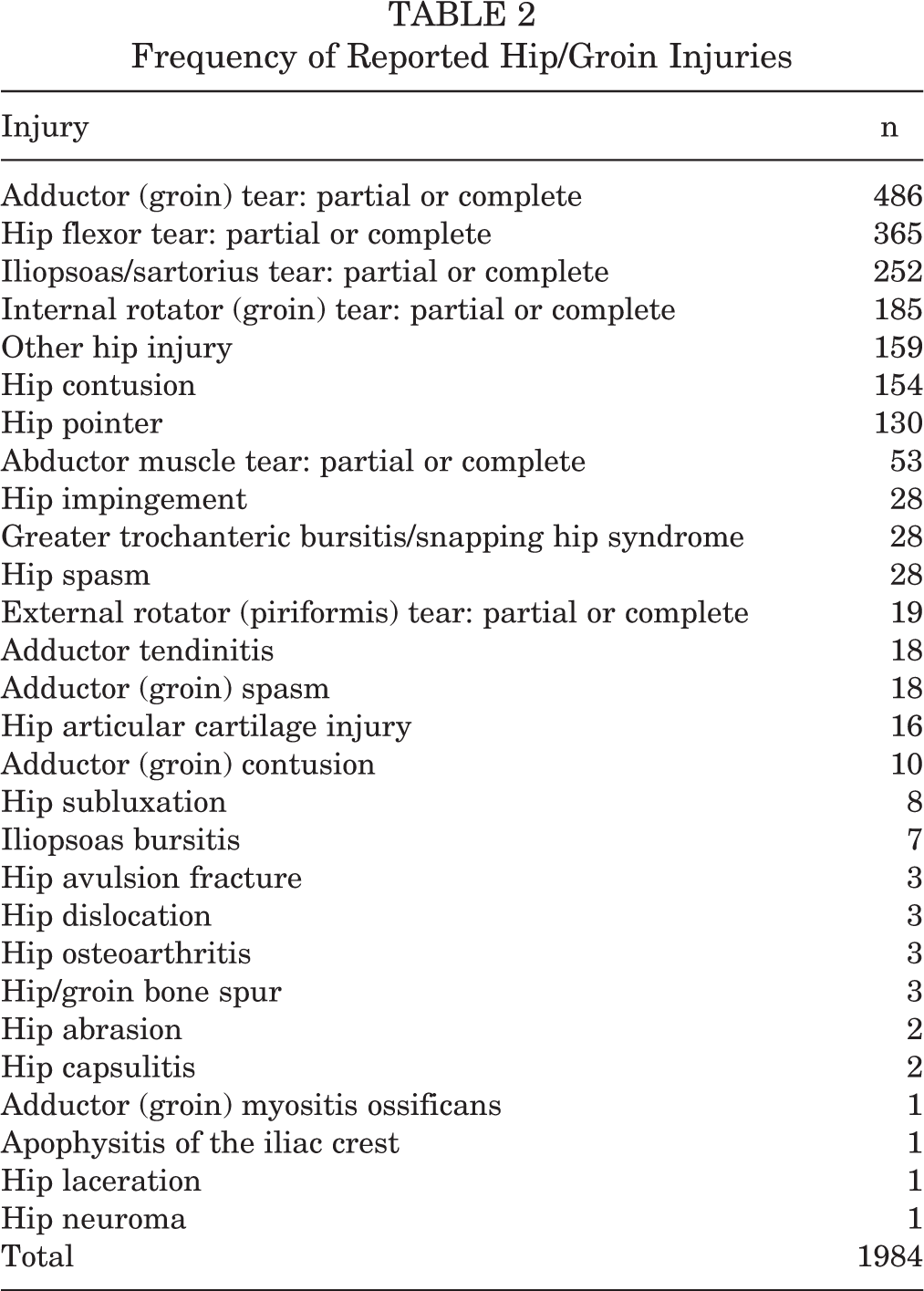
In total, 1984 hip/groin injuries were reported in 25 NCAA sports during the 2009-2010 through 2013-2014 academic years, resulting in an overall hip injury rate of 53.06 per 100,000 AEs (Table 1). The annual incidence of hip/groin injuries increased every academic year, starting at 315 injuries in 2009-2010 and rising to 495 injuries in 2013-2014. The most commonly reported injuries were an adductor/groin tear (n = 486), hip flexor tear (n = 365), iliopsoas/sartorius tear (n = 252), and internal rotator/groin tear (n = 185) (Table 2). The sports with the highest rates of hip injuries per 100,000 AEs were men’s soccer (110.84), men’s ice hockey (104.90), and women’s ice hockey (76.88). Although most hip injuries occurred during practices (66.83%) versus games (33.17%), the overall rate of injuries during games was significantly higher (RR, 2.18 [95% CI, 1.99-2.39]). The sport with the highest ratio of injuries in competition was men’s outdoor track (RR, 5.66 [95% CI, 2.86-11.19]), while the sport with the highest ratio of injuries in practice was men’s indoor track (RR, 0.29 [95% CI, 0.04-2.13]). In sex-comparable sports (basketball, cross-country, lacrosse, ice hockey, indoor track, outdoor track, soccer, swimming and diving, and tennis), hip injury rates per 100,000 AEs differed greatly, with men being affected more than women (59.53 vs 42.27, respectively; RR, 1.41 [95% CI, 1.28-1.55]). Additionally, women had a similar rate of hip injuries per 100,000 AEs in competition versus practice (42.17 vs 42.30, respectively; RR, 1.00 [95% CI, 0.82-1.21]), whereas men were much more likely to get injured in competition than during practice (138.91 vs 44.22, respectively; RR, 3.14 [95% CI, 2.82-3.50]).
Hip/Groin Injury Rates per 100,000 Athlete-Exposures by Sport

Frequency of Reported Hip/Groin Injuries
Mechanism of Injury
The most common hip and groin injury mechanisms were noncontact (48.4% of all injuries), overuse/gradual (20.4%), and player contact (13.0%) (Figure 1). Men’s cross-country had the highest proportion of injuries due to noncontact (71.4%), women’s swimming had the highest proportion of injuries due to overuse/gradual (70.0%), and men’s wrestling had the highest proportion of injuries due to player contact (38.5%). Across all sex-comparable sports, men had a larger proportion of injuries due to player contact than women (17.0% vs 3.6%, respectively; IPR, 4.80 [95% CI, 3.10-7.42]). In contrast, women had a larger proportion of injuries due to overuse/gradual than men (29.1% vs 16.7%, respectively; IPR, 1.74 [95% CI, 1.46-2.06]).

Distribution of the mechanism of injury for hip and groin injuries in 25 sports.
Time Loss, Injury Severity, and Surgery
Overall, 56.7% of hip injuries were NTL injuries, 39.3% were TL injuries, and 4.0% were unknown (Figure 2). Of all TL injuries, 5.9% were severe (defined as ≥14 days of time lost). Only 1.3% of all hip injuries (n = 25) required surgery. The sports with the largest proportion of NTL hip injuries were women’s swimming (90.0%), women’s tennis (85.7%), and women’s softball (77.4%). On the other hand, the sports with the largest proportion of severe injuries included women’s outdoor track (19.4%), men’s wrestling (11.5%), and women’s cross-country (10.3%). The sports with the largest proportion of injuries requiring surgery included women’s field hockey (6.7%), women’s lacrosse (5.4%), and men’s wrestling (3.9%). While there were a relatively high number of surgical procedures in men’s football (n = 7) and men’s ice hockey (n = 6), the overall proportions of injuries requiring surgery were still relatively low (1.2% and 2.0%, respectively).

Distribution of time lost from competition due to hip and groin injuries in 25 sports.
Across all sex-comparable sports, women had a higher proportion of NTL injuries than men (62.5% vs 54.2%, respectively; IPR, 1.15 [95% CI, 1.07-1.25]). In contrast, men had a higher proportion of severe injuries than women (6.2% vs 5.1%, respectively; IPR, 1.22 [95% CI, 0.81-1.83]) and a higher proportion of injuries requiring surgery than women (1.4% vs 1.0%, respectively; IPR, 1.35 [95% CI, 0.54-3.36]), although neither of these differences was statistically significant.
Discussion
Hip and groin injuries can result from participation in a variety of sports. Our data provide a deeper understanding of the incidence and clinical implications of these injuries occurring at the collegiate level. Through the 25 NCAA sports included in this study, a total of 1984 hip injuries were reported between the 2009-2010 and 2013-2014 academic seasons, resulting in an overall hip injury rate of 53.06 per 100,000 AEs. While several studies examining the incidence of hip and groin injuries in collegiate and professional athletes have previously been reported, it is difficult to directly compare these studies because of varied definitions of what constitutes a hip and groin injury and how best to measure the rate of occurrence. In a recent study of hip and groin injuries in National Basketball Association players, the rate of injuries was reported to be 3.26 per 1000 AEs; however, the definition of hip and groin injuries included the pelvis, hip, and thigh, and AEs were limited to games only. 28 Another study found the rate of intra-articular hip injuries in ice hockey players to be 1.81 per 1000 player-game hours, but the definition of hip injuries was narrowly focused, and the incidence rate metric used was different than that utilized in this study. 15 In 2008, Feeley et al 16 reported that hip and groin injuries accounted for 3.1% of all injuries in professional football players; however, they did not calculate the injury rate. The closest comparable study to our data was in professional baseball players, in which the rate of hip and groin injuries was found to be 1.2 per 1000 AEs across the major and minor leagues. 9 Prior studies on hip and groin injuries in collegiate athletes have used the NCAA ISP database, but these studies only focused on a specific sport and used older data, and many did not address sex differences within the same sport. 1,2,10 –12,34 To our knowledge, this study is the first to provide an overall incidence rate across a wide range of sports with a consistent metric of hip and groin injuries per 100,000 AEs.
Among all sports, an adductor/groin tear was the most common injury reported, comprising 24.5% of all hip injuries. This is consistent with prior studies that have demonstrated that an adductor/groin injury is a common acute injury in athletes, particularly in multidirectional sports such as soccer. 8,44,45,54,60 In a systematic review of groin injuries in sports, Maffey and Emery 40 found that groin strain rates ranged from 0.2 to 5.2 injuries per 1000 participation hours, and they were most common in sports that involved quick acceleration, sudden changes of direction, and overstretching the leg in abduction and external rotation, such as ice hockey and soccer. This is in contrast to chronic hip and groin pain in athletes, in which prior studies have shown that the hip joint itself is the most common site of injury. 5,50
Across the 25 collegiate sports included in this analysis, the highest rates of hip injuries per 100,000 AEs were in men’s soccer (110.84), men’s ice hockey (104.90), and women’s ice hockey (76.88). This is consistent with prior studies of athletic hip and groin injuries, which have shown that such injuries are common in sports that require kicking, sudden changes in direction, twisting, turning, and rapid acceleration and deceleration. 48,51,53,55 Many studies have shown that hip injuries are extremely common in soccer players, with estimations ranging from 8% to 18% of all soccer injuries. 19,54,59 Ice hockey involves all of the risk factors for hip injuries, with the exception of kicking, and has the additional biomechanical demands of skating, which place high tensile and compressive forces on the hip while accelerating and decelerating. 10 There are also the added risks of checking and avoiding being checked as well as the chronic muscle imbalances that develop around the hip in skaters. 10 What is less clear is the explanation for the discrepancy in injury rates between men and women in ice hockey and soccer. Some of the differences in ice hockey could be explained by the lack of checking in the women’s game, which may decrease the likelihood of contact injuries. 10 Our data support this explanation, showing a higher proportion of noncontact injuries in women's ice hockey compared with men’s ice hockey (59.8% vs 44.8%, respectively) and a very small proportion of player contact injuries in comparison with men’s ice hockey (2.3% vs 13.1%, respectively).
In sex-comparable sports, men had a significantly higher rate of hip and groin injuries per 100,000 AEs compared with women (59.53 vs 42.27, respectively; RR, 1.41 [95% CI, 1.28-1.55]). There are several potential explanations. In addition to the rule differences between some male and female sports, there are differences in playing styles. This is suggested by the finding that the dominant mechanism of injury for men was contact, while for women, it was gradual/overuse. It is also important to consider anatomic differences between male and female hips and the consequent alteration in biomechanical demands. These differences are most evident in soccer, in which prior studies have shown that men have more hip injuries while women have more knee injuries. 23,46 Previous research into the cause and rate of anterior cruciate ligament injuries in men versus women has shown different biomechanics as well as functional differences in task performance. 6,17,25,32,38 Similar mechanisms may be present in the hip to account for differences in injury rates. For example, prior studies have suggested that anatomic differences in female hips, such as a lower prevalence of cam-type deformities, may help protect against some types of hip injuries. 21,22,29,36,39,41 Another important consideration in sex-related injury discrepancies is the impact of the female athlete triad, which may also help explain the increased number of overuse injuries in female athletes. 27
When analyzing the length of time lost and the severity of injury, some interesting patterns emerge. Overall, 56.7% of hip injuries were NTL injuries, 39.3% were TL injuries, and 4.0% were unknown. This finding would seem to indicate that most hip and groin injuries are minor and result in little to no time lost from competition. However, there may be confounding factors, such as a more cautious approach to hip injury management. In their epidemiological study of hip and groin injuries in NCAA ice hockey players, Dalton et al 10 suggested that the recent increased awareness of hip injuries may have prompted coaches and ATCs to remove athletes from competition for minor hip issues, which may not have been considered injuries in the past.
Of the TL injuries, 5.9% were severe, defined as ≥14 days missed from athletic participation. The sports with the highest proportion of severe hip and groin injuries were women’s outdoor track (19.4%), men’s wrestling (11.5%), and women’s cross-country (10.3%). This further supports prior research, which has demonstrated that running is the most common sport associated with chronic groin pain in women. 5,26 However, there have been very few studies on hip and groin injuries in wrestling. In a retrospective review of 5595 sporting injuries in secondary school athletes over a 4-year period, Lam et al 37 found that of 264 wrestling injuries, none were in the hip/groin/thigh region. Other studies in wrestlers have been limited to case reports. 58,61 Our study indicates that while the overall rate of hip and groin injuries in wrestlers is low (33.02/100,000 AEs), many of these injuries are severe, requiring significant time lost from competition.
Among all hip and groin injuries, the proportion requiring surgical intervention was low (1.3%). The sports with the largest proportion of injuries requiring surgery included women’s field hockey (6.7%), women’s lacrosse (5.4%), and men’s wrestling (3.9%); however, the sample size of hip injuries was fairly low in all of these sports, and more data are required to make meaningful conclusions. Although men’s football and ice hockey had a higher number of hip injuries that required surgery (n = 7 and 6, respectively), the overall proportion of injuries requiring surgery was still relatively low (1.2% and 2.0%, respectively).
There are limited data from the literature on the prevalence of sports-related hip injuries requiring surgery. In 2013, Jackson et al 28 evaluated hip injuries in professional basketball players. The authors found that only 22 of 2852 injuries (0.8%) required surgery over a period of 24 years. 28 However, their study excluded offseason surgery and thus is probably not an accurate representation of the total burden of surgical hip injuries in basketball players. In studying professional baseball players, Coleman et al 9 found that 5.0% of minor league players and 7.8% of major league players required surgery for hip and groin injuries. In a systematic review of groin injuries in sports, Tyler et al 60 found that the incidence of surgery for adductor groin injuries in Major League Soccer players was 0.18 per 1000 hours of playing time. To our knowledge, our study is the first to quantify the proportions of athletic hip and groin injuries requiring surgery across multiple collegiate sports. The low number of surgical procedures in our data set relative to the studies of professional athletes cited above suggests that FAI and other hip/groin injuries may only become symptomatic once athletes are older and have participated in sports for a longer period of time.
Limitations
This study provides a broad overview of hip and groin injuries in a large sample of NCAA athletes participating in a wide range of sports. However, there are several limitations that must be considered when analyzing our findings. The NCAA ISP only includes data from a sample cohort of high-level college-aged competitive athletes and thus may not be generalizable to a wider population of older, younger, or less competitive athletes. Additionally, there is no standardized, specific, and reliable set of diagnostic criteria for many hip and groin injuries, which may lead to lower interrater reliability between ATCs, especially given the complexity and subjectivity of the diagnosis of these injuries in the acute setting. Further, while the macroscopic perspective offered by the database provides an interesting view of the overall epidemiology of hip/groin injuries, it also has inherent limitations for the sideline physician because the level of granularity is restricted by the deidentified nature of the data. We were therefore unable to provide sample characterization (eg, age, sex, number of participants) as done in traditional epidemiological studies. Another important limitation is the consistency of ATC reporting and representation across schools. While the NCAA ISP allows schools to use data imported directly from their electronic medical record system, which likely improves reporting consistency, participation is voluntary and does not have mandated, standardized reporting rules and regulations. Finally, the sample sizes varied greatly between sports and were possibly too small in certain sports to have statistical significance when compared with sports with a larger sample size.
Conclusion
Hip and groin injury rates, mechanisms of injury, and severity vary by sport, sex, and exposure (competition vs practice). In our study of 25 NCAA sports during the 2009-2010 through 2013-2014 academic years, we found that the most common injury mechanism was noncontact, especially in women. Most injuries did not result in time lost from competition, and few required surgery. A better understanding of such patterns will help formulate new injury prevention strategies and treatment modalities and decrease the risk of hip and groin injuries among collegiate athletes. Team physicians should have a heightened sense of awareness for possible hip/groin injuries in sports that require rapid changes in speed, direction, and acceleration, such as ice hockey and soccer. Additionally, it is important to coordinate the care of these athletes with rehabilitation providers, as most of these injuries require nonsurgical care. With many factors contributing to the incidence of hip/groin injuries, physicians and trainers must tailor treatments to the individual needs of the athlete.
Footnotes
Acknowledgment
The NCAA ISP data were provided by the Datalys Center for Sports Injury Research and Prevention. The ISP was funded by the NCAA. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the Datalys Center or the NCAA. The authors thank the many ATCs who have volunteered their time and effort to submit data to the NCAA ISP. Their effort is greatly appreciated and has had a tremendously positive effect on the safety of collegiate athletes.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.P.P. has received hospitality payments from Zimmer Biomet and had medical textbooks purchased by DePuy Synthes. M.K.M. has received hospitality payments from Arthrex, Zimmer Biomet, and Tornier and has received educational support from Arthrex.
Ethical approval for this study was waived by the Drexel University Office of Research.