
Abstract
Background:
Proper rehabilitation after matrix-associated autologous chondrocyte implantation (MACI) is essential to restore a patient’s normal function without overloading the repair site.
Purpose:
To evaluate the current literature to assess clinical outcomes of MACI in the knee based on postoperative rehabilitation protocols, namely, the time to return to full weightbearing (WB).
Study Design:
Systematic review; Level of evidence, 1.
Methods:
A systematic review was performed to locate studies of level 1 evidence comparing the outcomes of patients who underwent MACI with a 6-week, 8-week, or 10/11-week time period to return to full WB. Patient-reported outcomes assessed included the Knee injury and Osteoarthritis Outcome Score (KOOS), Tegner activity scale, Short Form Health Survey–36 (SF-36), and visual analog scale (VAS) for pain frequency and severity.
Results:
Seven studies met the inclusion criteria, including a total of 136 patients (138 lesions) who underwent MACI. Treatment failure had occurred in 0.0% of patients in the 6-week group, 7.5% in the 8-week group, and 8.3% in the 10/11-week group at a mean follow-up of 2.5 years (P = .46). KOOS, SF-36, and VAS scores in each group improved significantly from preoperatively to follow-up (P < .001).
Conclusion:
Patients undergoing MACI in the knee can be expected to experience improvement in clinical outcomes with the rehabilitation protocols outlined in this work. No significant differences were seen in failure rates based on the time to return to full WB.
Articular cartilage injuries in the knee joint are common, with a prevalence of 32% in patients in their 20s undergoing knee arthroscopic surgery and 46% of patients in their 30s. 5,7 Articular cartilage has a limited capacity for spontaneous repair after an injury, 3 and if left untreated, full-thickness cartilage lesions can lead to symptoms such as pain, swelling, and joint dysfunction. 4 Several operative methods exist to treat these lesions, 25,30 although autologous chondrocyte implantation (ACI) has gained significant interest recently, with several clinical trials currently being conducted in the United States. 23
Third-generation ACI, or matrix-associated ACI (MACI), is performed in a 2-step process in which a patient undergoes knee arthroscopic surgery to obtain a biopsy of healthy cartilage. Chondrocytes from this biopsy sample are then cultured over several weeks and implanted into a collagen or hyaluronan-based scaffold before being cut to the shape and size of the patient’s chondral defect and fixed to the defect with fibrin glue. Favorable midterm to long-term outcomes have been demonstrated after MACI in the knee joint, with a 9.4% failure rate at a minimum 5-year follow-up. 31
A recent review showed that 13 of 22 studies of MACI in the knee joint either did not report or did not adequately describe their postoperative rehabilitation protocol. 2 Proper rehabilitation after MACI is essential to restore a patient’s normal function without overloading the repair site. 13 Thus, it is important to establish an effective rehabilitation protocol for health care providers and patients undergoing this procedure. The purpose of this systematic review was to evaluate the current literature to assess the clinical outcomes of MACI based on postoperative rehabilitation protocols, in particular the time to return to full weightbearing (WB). We hypothesized that no significant differences in clinical outcomes would be found based on the rehabilitation protocol.
Methods
A systematic review of multiple databases was performed. Two independent reviewers searched PubMed, Embase, and Cochrane Library up to February 9, 2017, using the search phrase “autologous chondrocyte knee rehabilitation.” A total of 339 studies were reviewed by title and/or abstract to determine study relevance based on inclusion/exclusion criteria. Inclusion criteria consisted of studies with level 1 evidence and a minimum 12-month follow-up in which clinical outcomes were compared between at least 2 groups of patients with different times until return to full WB. Studies were excluded if postoperative assessments were not used, if they were nonclinical or noncomparative studies, or if they were unrelated to the knee. Seven studies met inclusion and exclusion criteria (Figure 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Surgical Technique
Each study 8 –12,35,36 used a third-generation MACI product. This procedure is a 2-stage technique in which an arthroscopic approach is first used to harvest a sample of normal articular cartilage from a non-WB region of the knee. Chondrocytes are then isolated, cultured, and seeded onto a collagen or hyaluronan-based scaffold. At 3 to 8 weeks after the chondral biopsy, the second stage of the procedure involves mini-arthrotomy to implant the scaffold in the lesion site. The chondral defect is prepared by removing all damaged cartilage down to the subchondral plate and is then used to shape the scaffold, which is pressed into the lesion site and secured with a thin layer of fibrin glue. The graft is assessed for stability before the wound is closed. Two studies 8,12 performed the second stage of the MACI procedure either arthroscopically or through mini-arthrotomy. In addition to the 2 different MACI techniques, there was also a variety of matrix scaffold types and manufacturers used (Table 1). Two studies 35,36 did not use the same matrix in all patients.
Matrix-Associated Autologous Chondrocyte Implantation Products

Rehabilitation Protocols
Patients in all included studies were randomized into either a 6-week, 8-week, or 10/11-week time period before return to full WB (Table 2). Four studies 8,12,35,36 described a 6-week rehabilitation protocol consisting of an initial 2-week period of WB at 20%, followed by a progressive increase to full WB at 6 weeks postoperatively. Five studies 8 –12 described an 8-week rehabilitation protocol consisting of a 2-week period of WB at 20%, with a progressive increase to full WB at 8 weeks postoperatively. Two studies 35,36 described a 10-week rehabilitation protocol consisting of toe-touch WB for 4 weeks, followed by partial WB at 20% between weeks 4 and 6, 50% WB between weeks 6 and 8, and full WB by 10 weeks postoperatively. Three studies 9 –11 described an 11-week rehabilitation protocol consisting of a 5-week period of WB at 20%, with a progressive increase to full WB at 11 weeks. All 7 studies used continuous passive motion (CPM) as part of the rehabilitation process for all patients included. Five studies 8 –12 began CPM within 12 to 24 hours after surgery from 0° to 30° of flexion, and 2 studies 35,36 used CPM for 3 hours per day beginning 24 hours postoperatively from 0° to 40° of flexion.
Rehabilitation Protocols a

a Each study randomized patients into 2 of the following 3 rehabilitation protocols: 6-week, 8-week, or 10/11-week return to full weightbearing.
Outcomes
Outcome measures included patient-reported outcome scores, magnetic resonance imaging (MRI) findings, functional test results, and treatment failure. The Knee injury and Osteoarthritis Outcome Score (KOOS) 28 was used in 6 studies. 8 –11,35,36 Two studies 35,36 used the Tegner activity scale. 32 Four studies 8 –11 used the Short Form Health Survey–36 (SF-36) 34 and the visual analog scale (VAS) for pain frequency and severity. All studies used high-resolution MRI to assess graft adherence postoperatively. Four studies 8 –11 used the MRI composite score, 2 studies 35,36 used the MOCART (magnetic resonance observation of cartilage repair tissue) scoring system, 24 and 1 study 11 did not describe any MRI results beyond stating that there was no complete graft delamination in any patient as assessed by MRI. The 6-minute walk test, 16 a test to assess the maximum distance that each patient could comfortably walk in a 6-minute time period, and active knee flexion and extension were the most common functional tests used to assess patients postoperatively. Four studies 8 –11 reported 6-minute walk test results and measured active knee flexion and extension.
Methodology Assessment
The Modified Coleman Methodology Score (MCMS) 6 was used to evaluate study methodology quality. The MCMS has a scaled potential score ranging from 0 to 100. Scores of 85-100 are excellent, 70-84 are good, 55-69 are fair, and <55 are poor.
Treatment Failure
Five of the 7 studies reported treatment failure. Four studies 8,10 –12 defined treatment failure as complete delamination of the implanted graft and its resulting inability to withstand dynamic forces placed upon it during return to full WB, while 1 study 9 defined treatment failure as a subchondral bed devoid of any significant repair tissue. Two studies 35,36 did not report on treatment failure. Only the latest follow-up was used from each population sample group to assess treatment failure.
Statistical Analysis
A chi-square test was used to compare lesion locations and treatment failure rates between groups. For patient-reported outcomes, a weighted mean ± composite SD was calculated for each group, as previously described. 22 Preoperative and postoperative scores were compared within each group using a 2-samples independent t test based on unequal variance (http://www.openepi.com).
Results
The 7 studies included in the review had overlapping patients. Overall, there were a total of 3 separate patient samples, including 136 nonoverlapping patients and 138 nonoverlapping lesions.
Patient Demographics
Patient demographics are shown in Table 3. There were a total of 34 lesions treated with the 6-week protocol, 53 lesions treated with the 8-week protocol, and 51 lesions treated with the 10/11-week protocol. A total of 37 lesions were treated on the lateral femoral condyle and 101 on the medial femoral condyle. No significant difference was found between groups with regard to lesion location (P = .85). Although all patients were randomized to the different rehabilitation protocols, a trend was noted, with younger patients being randomized to the shorter duration protocols. Three studies 8,12,35 directly compared body mass index between study groups and found no significant differences.
Patient Demographics a

a Lesion size, age, weight, height, and BMI are all reported as mean ± SD (if available), with “total” reported as weighted mean. Only the nonoverlapping patient samples are included to avoid redundancy. BMI, body mass index; LFC, lateral femoral condyle; MFC, medial femoral condyle; NR, not reported.
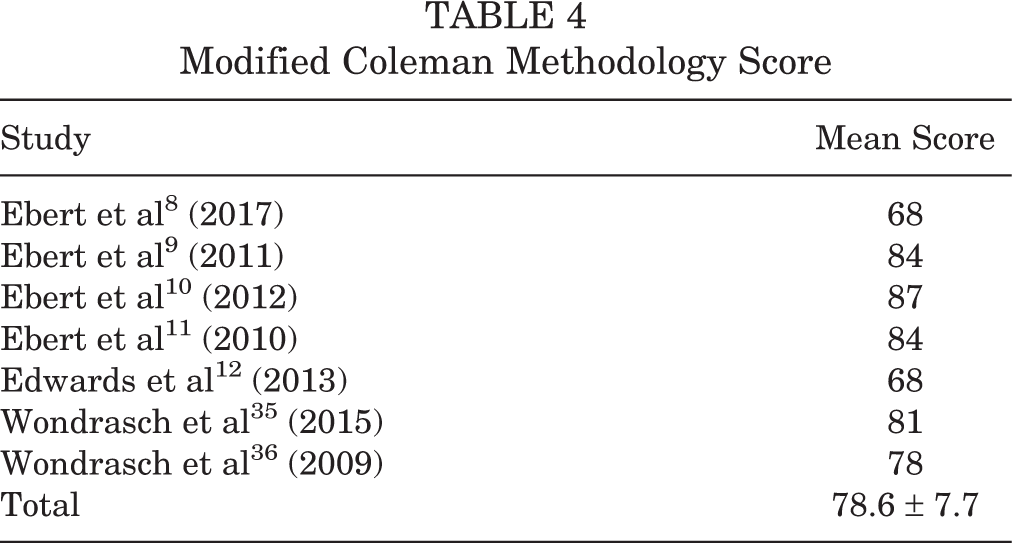
Modified Coleman Methodology Score
Table 4 shows the MCMS scores from the 7 included studies. One study 10 achieved an excellent score, 4 studies achieved good scores, and 2 studies achieved fair scores.
Modified Coleman Methodology Score
Treatment Failure
Overall, 6.5% of patients experienced graft failure (6 wk: 0.0%; 8 wk: 7.5%; 10/11 wk: 8.3%; P = .46) at a mean follow-up of 2.5 years (Table 5). Ebert et al 10 found that 5 patients experienced graft failure, including 2 patients at 2-year follow-up (8 wk: n = 1; 10/11 wk: n = 1) and 3 more at 5-year follow-up (8 wk: n = 1; 10/11 wk: n = 2). In addition to treatment failure, Ebert et al 10 reported that seven 8-week patients and six 10/11-week patients experienced graft hypertrophy as detected by MRI at 5-year follow-up. Studies did not report on the age or sex of the patients who failed treatment.
Treatment Failure a
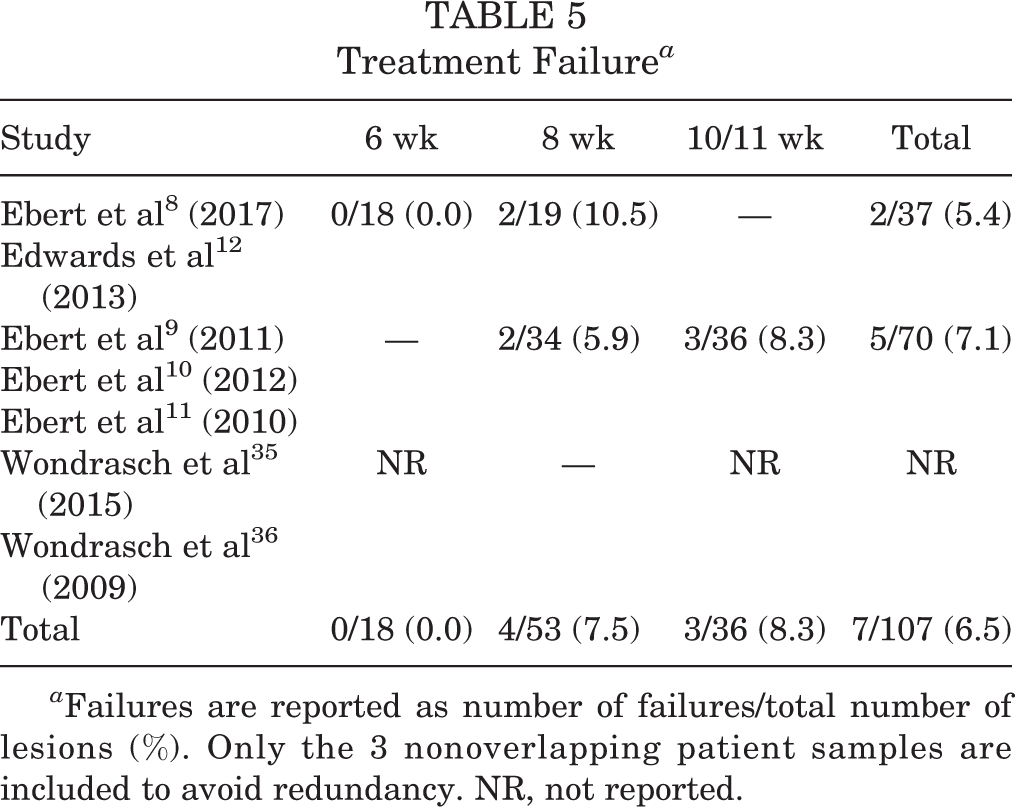
a Failures are reported as number of failures/total number of lesions (%). Only the 3 nonoverlapping patient samples are included to avoid redundancy. NR, not reported.
MRI Assessment
Two studies of overlapping patients 9,10 reported significant improvement (P < .0001) in the MRI composite score among the 8-week and 10/11-week rehabilitation groups from 3 months to 24 months postoperatively and then again from 24 months to 5 years (P < .05). However, there was no significant difference in improvement between the 2 groups at either time interval. Another study 8 found that 100% of patients in the 6-week group had MRI composite scores that were graded as good to excellent, compared with 78% in the 8-week group. Both groups experienced significant improvement (P < .0001) in the MRI composite score from 3 months to 24 months postoperatively, with no significant difference in improvement between groups. Edwards et al 12 found that 100% of patients in the 6-week group demonstrated good to excellent MRI composite scores, compared with 85% in the 8-week group. Both groups improved significantly (P < .001) from 12 weeks to 12 months postoperatively, with no significant difference in improvement between groups. Two studies of overlapping patients 35,36 reported that the 6-week and 10/11-week groups demonstrated significant improvements (P < .05) in the MOCART score from 4 weeks to 2 years postoperatively. However, from 2- to 5-year follow-up, both groups experienced significant decreases (P < .05) in the MOCART score. There was a significantly higher MOCART score in the 10/11-week group (67.2 points) compared with the 6-week group (59.7 points) at 4 weeks postoperatively (P = .022), with a normalization of scores by 1-year follow-up. Otherwise, no significant difference in improvement or regression was found between groups.
SF-36 and VAS
SF-36 and VAS scores are presented in Table 6. Significant improvement was noted from preoperatively to latest follow-up within each group for each of these outcomes (P < .0001).
SF-36 and VAS Scores a

a Scores are reported as mean ± SD and are taken from the latest postoperative evaluation for each nonoverlapping group of patients, with “total” reported as weighted mean ± composite SD. Significant improvements were found for each outcome in each group (P < .0001). MCS, mental component summary; PCS, physical component summary; SF-36, Short Form Health Survey–36; VAS, visual analog scale.
Knee Injury and Osteoarthritis Outcome Score
KOOS subscores are presented in Table 7. Significant improvement was noted from preoperatively to latest follow-up within each group for each of these subscales (P < .001).
KOOS Subscores a

a Subscores are reported as mean ± SD, with “total” reported as weighted mean ± composite SD. Significant improvements were found for each outcome in each group (P < .001). ADL, activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; NR, not reported; QOL, quality of life; SR, sports and recreation.
Tegner Activity Scale
Two studies of overlapping patients 35,36 identified no significant differences in the Tegner score between 6-week and 10/11-week groups at 2- or 5-year follow-up (time effect: P = .394; group effect: P = .204). Both groups demonstrated improvement in the Tegner score from preoperative values, and a mean score of 4.0 was found for both groups at the 2- and 5-year follow-up periods.
Functional Tests
Functional test results are presented in Table 8. Significant improvement was noted from preoperatively to latest follow-up within each group for each of these tests (P < .0001). No studies reported preoperative 6-minute walk test or range of motion results for the 6-week group, and therefore, mean improvement could not be calculated for this group.
Functional Test Results a

a Results are reported as mean ± SD, with “total” reported as weighted mean ± composite SD. Significant improvements were found for each outcome in the 8-week and 10/11-week groups (P < .0001). NR, not reported.
Discussion
Based on the results of this systematic review, patients undergoing MACI for articular cartilage lesions in the knee can be expected to experience improvement in clinical outcomes with the rehabilitation protocols outlined in this work. It should be noted that among the studies included that reported Tegner scores, a mean score of 4.0 was reported at follow-up, indicating that these were relatively low-activity patients. 35,36 Although it could not be proven in this review that any of the rehabilitation groups improved to a significantly greater extent than the others, allowing patients to bear full weight at 6 weeks postoperatively allows a quicker return to activity and should be recommended given the significant improvement in various outcomes reported among this group.
Proper rehabilitation after MACI is essential to restore a patient’s normal function without overloading the repair site. Several studies from the basic science literature have investigated the response of chondrocytes to mechanical stimuli. 15,20,27,29 The effects of dynamic loading on chondrocyte differentiation and cellular synthesis depend both on the frequency and duration of cyclic loading. 14 Elder et al 15 found that cyclic loading of chick limb bud cells embedded in agarose gel resulted in a doubling of the number of cartilage nodules compared with nonloaded controls, while static compression was found to have little effect on cellular differentiation. In addition to cellular differentiation, Quinn et al 27 found that dynamic compression of cartilage explants resulted in the stimulation of proteoglycan synthesis and pericellular deposition. Similarly, Sah et al 29 found that higher frequency dynamic compression of cartilage explants resulted in greater glycosaminoglycan synthesis. Conversely, joint immobilization has been shown to have a deleterious effect on cartilage synthesis in animal models as a result of decreased proteoglycan synthesis and increased proteolysis. 1,18,26 These findings stress the importance of early return to WB to stimulate cellular differentiation of the chondrocytes seeded into the collagen membranes used for MACI. However, returning to full WB too early after MACI may cause graft delamination or destruction.
Mechanical stimulation also has a beneficial effect on the integration of in vitro tissue-engineered implants with host tissue. 33 This is particularly important for a procedure such as MACI, which relies on integration between a patient’s healthy, native cartilage tissue and the chondrocyte-seeded collagen scaffold implanted into the defect site.
Clinically, CPM is frequently used immediately after articular cartilage procedures in the knee. Limited clinical evidence exists regarding the benefits of CPM on articular cartilage repair. 17,19 However, in animal models, CPM has been shown to promote neochondrogenesis and to significantly improve knee motion and cartilage quality. 19,21 All 7 studies from our review 8 –12,35,36 described using CPM early in the rehabilitation process, although the timing and range of motion used with CPM did not vary between groups in any particular study. Therefore, this review could not assess the role of CPM in rehabilitation after MACI.
Clearly, significant evidence exists supporting the benefits of early joint mobilization on articular cartilage quality and neochondrogenesis. Proper rehabilitation after MACI involves maintaining an important balance between restoring normal joint function and cartilage quality without overloading the repair site before complete repair and integration of the graft. It is unclear how long it takes for these matrix scaffolds to heal and integrate with the surrounding native cartilage tissue, although this likely depends on a number of factors, including the type of scaffold, the defect size and location, the chondrocyte density of the scaffold, patient age, and the WB status of the patient.
The strengths of this study include a comprehensive systematic review performed by 2 independent reviewers. In addition, only randomized controlled trials (level 1 evidence) were included. The limitations of this study should also be noted. In particular, although 7 studies were included, these included only 3 nonoverlapping patient samples. In addition, the rehabilitation period comparisons were skewed such that one group (with 5 studies included in this review) primarily compared 8 versus 10 weeks to full WB, whereas another group (with 2 studies in this review) compared 6 versus 10 weeks to full WB. Furthermore, these 2 groups treated lesions of different sizes. Different MACI scaffolds and surgical procedures (either arthroscopic surgery or mini-arthrotomy for the second stage of the MACI procedure) were included and grouped together to create a sample size large enough for clinical outcome comparisons. The mean follow-up duration differed between groups, which may have an effect on some of the outcomes assessed. The studies did not provide demographic information on the patients who failed treatment, and therefore, it was not possible to conduct a subanalysis based on these factors. Most studies did not report on the mean time from initial injury until treatment with MACI. All lesions included in this review were on the medial or lateral femoral condyle, and therefore, the results of this review are not indicative of chondral lesions treated on the tibial plateaus or in the patellofemoral joint. Finally, although rehabilitation protocols of the respective 6-week, 8-week, and 10/11-week groups were reflective of time to return to full WB, they were not otherwise identical.
Conclusion
Based on the findings of this systematic review, patients undergoing MACI for articular cartilage lesions in the knee can be expected to experience improvement in clinical outcomes with the rehabilitation protocols outlined in this work.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: E.C.M. is a paid consultant for Biomet and DePuy, receives royalties from Biomet and Elsevier, and receives research support from Biomet, Mitek, Smith & Nephew, and Stryker.