
Abstract
Background:
Arthroscopic stabilization is the most broadly used surgical procedure in the United States for management of recurrent shoulder instability. Latarjet coracoid transfer has been considered a salvage surgical procedure for failed arthroscopic repairs or cases of significant glenoid bone loss; however, with recent literature suggesting reduced risk of recurrent instability with Latarjet, several surgeons have advocated its broader utilization as a primary operation for treatment of shoulder instability.
Purpose:
To determine trends in shoulder stabilization techniques used in the United States.
Study Design:
Cross-sectional study.
Methods:
A retrospective analysis of a publicly available national insurance database was performed to identify shoulder stabilization procedures performed over 9 years (2007-2015). The following Current Procedural Terminology codes were searched: 29806 (arthroscopic stabilization), 23455 (open capsulolabral repair), 23466 (open capsular shift), 23462 (Latarjet coracoid transfer), and 23460 (open anterior capsulorrhaphy with other bone block augmentation). Outcomes of interest included (1) trends in the use of each technique throughout the study interval, (2) age and sex distributions of patients undergoing each technique, and (3) regional predilections for the use of each technique.
Results:
Arthroscopic stabilization was the most broadly used shoulder stabilization procedure in the database (87%), followed by open Bankart (7%), Latarjet (3.2%), open capsular shift (2.6%), and alternative bone block procedure (0.8%). Throughout the study period, the incidence of arthroscopic stabilization and Latarjet increased (8% and 15% per year, respectively); the incidence of open capsular shift remained relatively constant; and the incidence of open Bankart decreased (9% per year). Arthroscopic stabilization, open Bankart, and Latarjet each had similar sex-based distributions (roughly 70% male), while open capsular shift and alternative bone block were relatively more common in females (54% and 50% male, respectively). The incidence of arthroscopic stabilization and Latarjet were greatest in the South and lowest in the Northeast.
Conclusion:
Arthroscopic stabilization remains the most commonly utilized stabilization technique in the United States. The use of the Latarjet procedure is steadily increasing and now rivals open Bankart stabilization among the most commonly used open stabilization techniques.
Recurrent anterior shoulder instability is a disabling condition. Many surgical techniques exist for treatment of shoulder instability, including arthroscopic capsulolabral (Bankart) repair, open Bankart repair, Latarjet coracoid transfer, open capsular shift, and alternative bone block stabilization procedures (ie, iliac crest or allograft); however, the optimal surgical intervention to address recurrent instability remains controversial. In the United States, arthroscopic Bankart repair is currently the most broadly used shoulder stabilization procedure. 8,17 Arthroscopic Bankart repair is a minimally invasive technique that carries a low risk of complication and recurrence. A recent systematic review of >1700 patients revealed that arthroscopic Bankart repair offers short-term results comparable to open Bankart repair with regard to risk of recurrent instability (8.5% vs 8%) and return to sport (87% vs 89%). 10 Nevertheless, some surgeons continue to favor open Bankart for contact athletes and manual laborers owing to a longer interval to recurrence and a reduced recurrence rate among collision athletes. 7,11,14,18 For patients with a history of failed arthroscopic or open capsulolabral repair or those with clinically significant anterior glenoid bone loss, the Latarjet procedure is considered an excellent option. Notably, recent comparative trials have found that primary Latarjet coracoid transfer may result in a reduced rate of recurrent instability when compared with arthroscopic stabilization. 2,19 As a result of these data, some have advocated broader utilization of the Latarjet as the initial surgical technique for patients with shoulder instability.
The purpose of this study was to determine the current trends in utilization of shoulder stabilization techniques in the United States based on data from a large private-payer database. Specifically, we sought to determine (1) relative trends in the use of arthroscopic Bankart repair, open Bankart repair, Latarjet coracoid transfer, open capsular shift, and alternative bone block stabilization; (2) age and sex distributions of patients undergoing each technique; and (3) regional predilections for the use of each technique. We hypothesized that over the study interval, there would be an increase in the use of Latarjet and a corresponding decrease in the use of open Bankart repair.
Methods
A retrospective review of the PearlDiver database was performed to evaluate trends in shoulder stabilization procedures performed between 2007 and 2015. The PearlDiver database is a publicly available national database that is compliant with the Health Insurance Portability and Accountability Act (HIPAA). The database uses supercomputer technology to collate individual patient records associated with codes related to orthopaedic procedures per Current Procedural Terminology (CPT) and the International Classification of Diseases, Ninth and Tenth Revision (ICD-9 and -10). The database comprises cases covered under Humana and Medicare insurance policies. Because most patients with shoulder instability are young and athletic, we elected to specifically investigate the Humana database (excluding patients covered under Medicare). Of note, Humana insures 22.7 million people in the United States, including 12.1 million in the South, 5.6 million in the Midwest, 3.2 million in the West, and 1.8 million in the Northeast. The Humana database was queried to identify the number of patients who underwent surgery in the study interval with the following CPT codes: 29806 (arthroscopic stabilization), 23455 (open capsulolabral repair), 23466 (open capsular shift), 23462 (Latarjet coracoid transfer), and 23460 (open anterior capsulorrhaphy with other bone block augmentation; ie, iliac crest or allograft).
The primary data points that were extracted included year of surgery, patient age at the time of surgery (broken down into the following age groups: 10-14, 15-19, 20-24, 25-29, 30-34, 35-39, 40-44, 45-49, 50-54, and 55-59 years), patient sex, and the geographic region of the United States in which surgery was performed as defined by the US Census Bureau definition (divided into Northeast, South, West, and Midwest) (Table 1). The database did not permit distinction of primary and revision procedures. The total number of patients in the Humana database insured in each region were calculated and used as the “population at risk” to determine the regional incidence of each procedure per million insured.
States in Each Region of the United States (Defined by US Census Bureau Definition)

Linear regression analysis was used to calculate trends in the use of each surgical technique. A statistically significant trend was defined by r 2 > 0.6 and P < .05. A chi-square goodness-of-fit test was used to calculate differences in age and sex distributions and regional predilections for each procedure. Statistical significance was defined as P < .05. Statistical analyses were performed with SPSS (v 23; IBM).
Results
During the study period between January 2007 and December 2015, a total of 5985 shoulder stabilization procedures were performed per the Humana database of 22.7 million patients. Arthroscopic stabilization was the most commonly utilized procedure, performed in 87% of cases (n = 5157), followed by open Bankart in 7% (n = 432), Latarjet in 3.2% (n = 190), open capsular shift in 2.6% (n = 156), and alternative anterior bone block augmentation (including iliac crest or allograft reconstruction) in 0.8% (n = 50). Throughout the study interval, there were significant increases in the use of Latarjet coracoid transfer (increase of 15.4% annually, r 2 = 0.88, P < .001) and arthroscopic stabilization (increase of 7.9% annually, r 2 = 0.89, P < .001) (Figure 1). Throughout the study interval, there was a decrease in use of open Bankart (decrease of 9.1% annually; r 2 = 0.60, P < .001). There was no significant trend for open capsular shift (decrease of 3.5%; r 2 = 0.08, P = .45). At the beginning of the study interval (2007), open Bankart was performed >6 times as commonly as Latarjet (68 vs 11); however, by the end of the interval (2015), the 2 techniques were used in a similar number of cases (38 vs 35). Likewise, Latarjet was used less commonly than open capsular shift in 2007 and 2008 but outnumbered open capsular shift every year since 2011 and surpassing it by 58% from 2014 to 2015 (63 vs 40).

Trends in the use of arthroscopic stabilization, the Latarjet procedure, open Bankart, and open capsular shift between 2007 and 2015 (represented by dashed lines; percentages represent the proportion of each procedure performed in the year of interest).
There was no difference in proportion of male patients in the arthroscopic stabilization, Latarjet, and open Bankart cohorts (respectively, 70% [n = 3624] vs 69% [n = 131]) vs 68% [n = 295]; P = .69). There was a greater proportion of male patients in the Latarjet cohort than in the open capsular shift cohort (54% [n = 85], P = .007) and alternative bone block cohort (50% [n = 25], P = .02) (Figure 2). Arthroscopic stabilization and open Bankart were both performed most commonly among patients aged 15 to 19 years (22% and 20%, respectively) (Figure 3). Latarjet was performed most commonly among patients aged 20 to 24 years (16%), with 54% performed among patients 15 to 34 years of age. Open capsular shift was performed most commonly among patients aged 15 to 19 years (27%), with 54% performed among patients 15 to 34 years of age.

Sex distribution for procedures performed between 2007 and 2015: arthroscopic shoulder stabilization, Latarjet, open capsular shift, and alternative anterior bone block. P values represent difference in sex distribution as compared with arthroscopic stabilization.
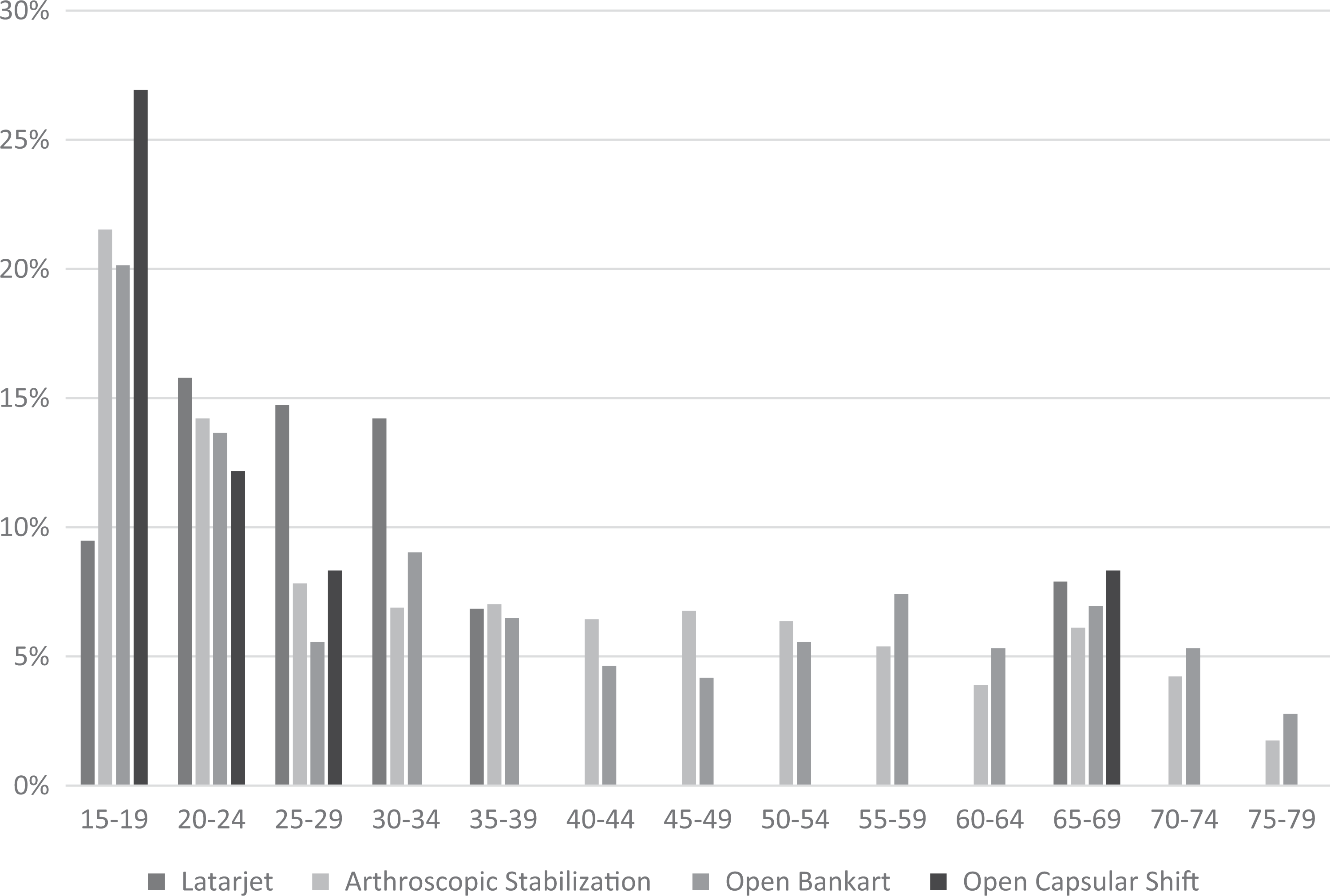
Age distribution for procedures performed between 2007 and 2015: Latarjet, arthroscopic stabilization, open Bankart, and open capsular shift. Age groups with <11 patients are not represented.
The incidences of Latarjet and arthroscopic stabilization were highest in the South (9.9 and 266.7 per million people, respectively) and lowest in the Northeast (1.7 and 16.1 per million people) (Figure 4). Of note, the incidence of Latarjet was greater in the South versus the Northeast and Midwest (P = .002 and P = .023) but not greater than the West (P = .677). The incidence of arthroscopic stabilization was greater in the South than each of the 3 other regions (P < .001).
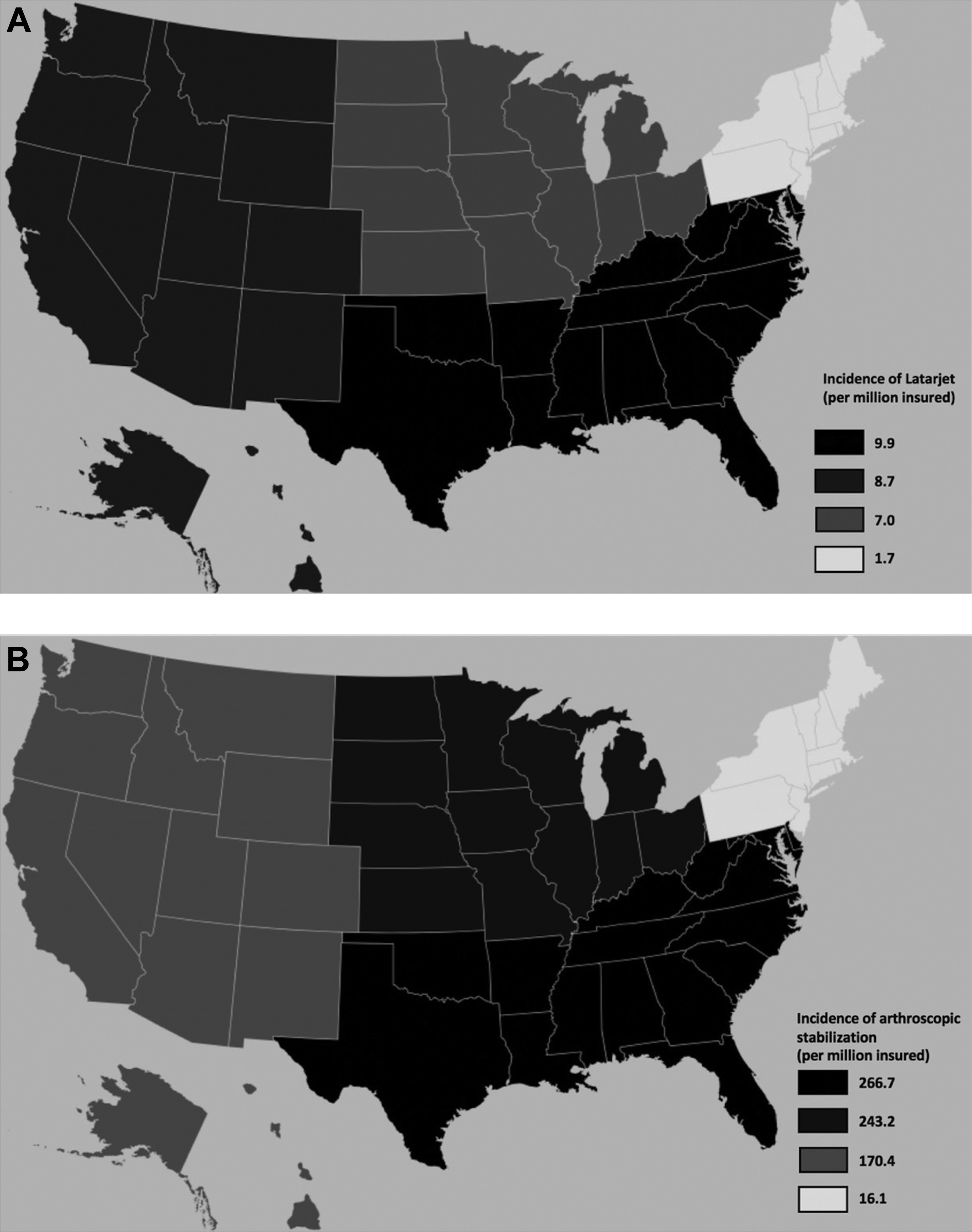
Incidence of the use of (A) Latarjet and (B) arthroscopic stabilization in each of the 4 regions represented in the PearlDiver database (incidence reported per million people in the insured population).
Discussion
The principal findings of this study indicate that there are (1) increasing trends in the use of Latarjet and arthroscopic stabilization and a decreasing trend in the use of open Bankart stabilization; (2) males between 15 and 34 years old represented the primary demographic group undergoing arthroscopic stabilization, open Bankart, and Latarjet, with relatively more females undergoing open capsular shift and alternative bone block augmentation; and (3) arthroscopic stabilization and Latarjet reconstruction are both performed at a higher incidence in the South and a lower incidence in the Northeast versus other regions.
An international survey of the European, American, and South African arthroscopy societies demonstrated that Latarjet is the preferred surgical technique by 72% of French surgeons while arthroscopic Bankart repair is favored by 90% of surgeons outside of France. 17 Although arthroscopic Bankart repair is the most commonly utilized shoulder stabilization procedure in the United States, recent literature from France advocates broader use of the Latarjet coracoid transfer for primary anterior shoulder stabilization owing to a reduced risk of recurrent instability. 2,3,19 The results from this study suggest that while use of the Latarjet procedure is increasing in the United States, arthroscopic stabilization remains the most commonly performed procedure.
The rise in use of the Latarjet procedure is likely multifactorial and can be attributed to favorable European literature, increased international collaboration that has promoted dissemination of European shoulder techniques in the United States, and increased literature on the importance of identifying and treating glenoid bone loss. The simultaneous decrease in the use of open Bankart is likely related to (1) the societal perception that arthroscopic surgery is preferred, (2) the reduced exposure to open soft tissue stabilization during training, and (3) the increased utilization of Latarjet for challenging cases that may have previously been treated with open Bankart.
One existing study in the literature used registry data to evaluate trends in shoulder stabilization techniques performed in the United States. Degen and colleagues 8 reported on trends in bone block augmentation procedures among recently trained orthopaedic surgeons based on data from the American Board of Orthopaedic Surgeons database. Their data included 7587 stabilizations performed between 2004 and 2013, of which 88% (n = 6707) were performed arthroscopically and only 0.95% (n = 72) involved bone block augmentation (the authors did not differentiate between Latarjet and alternative bone block procedure). Our study also indicates that arthroscopic stabilization remains the favored procedure; however, bone block augmentation is used more broadly than previously thought, constituting 4.0% of stabilizations in the study interval (of which 79% were Latarjet and 21% were iliac crest or allograft reconstruction). The greater number of bone block procedures revealed here may be partially explained by the fact that our study evaluated a more recent interval (2007-2015 vs 2004-2013). Of note, 33% (63 of 190) of the Latarjet procedures in our study were performed within the past 2 years. Additionally, our study may be more reflective of surgical trends at large, as Degen and colleagues 8 looked specifically at data from the American Board of Orthopaedic Surgeons part 2 examination, which includes cases performed by recently trained surgeons and may not be representative of practice patterns of more experienced surgeons. More experienced surgeons may feel more comfortable performing open stabilization techniques, including bone block augmentation, for patients who are appropriate candidates. Additionally, more experienced surgeons may see more revision cases that might necessitate Latarjet as a salvage option.
The demographic profile of patients undergoing arthroscopic stabilization, open Bankart, and Latarjet coracoid transfer was comparable, as all 3 procedures were most commonly used for men (around 70% of patients in each group) between the ages of 15 to 34 years (around 50% in each group). This demographic profile is comparable to what has been published in systematic reviews evaluating procedures for traumatic anterior instability (70%-80% male; mean age, 26-28 years). 1,12,13 Open capsular shift and alternative bone block procedures are used relatively more commonly for females than the other 3 techniques. The increased utilization of open capsular shift for females likely relates to the female predominance of generalized ligamentous laxity and multidirectional instability. 9,16 Systematic review data from studies evaluating procedures for multidirectional instability reveal a more even sex distribution (50% male). 6 Latarjet was used more commonly in older patients than the other techniques as it represented the only technique used most prevalently in patients 20-24 years of age (arthroscopic stabilization, open Bankart, and open capsular shift were all used most prevalently in patients 15-19 years of age). This likely relates to the fact that Latarjet remains most prevalent in the revision setting and among patients with a greater number of instability events (resulting in significant glenoid bone loss).
We hypothesized that the incidence of all shoulder stabilization techniques would be consistent throughout all regions of the United States. Interestingly, we found a significant increase in the use of arthroscopic stabilization and Latarjet in the South and a reduced incidence in the Northeast (including a 5-fold increase in the use of Latarjet in the South and West regions vs the Northeast). We surmise that this partially relates to the relative popularity of football in the South versus the Northeast. A 2014-2015 survey of high school athletic participation performed by the National Federation of State High School Associations revealed that each of the 9 states with the highest proportion of athletes participating in football reside within the South region (Figure 5). 15 Furthermore, 8 of the 9 states with the lowest proportion of athletes participating in football reside within the Northeast region. Multiple studies in the literature have demonstrated a high rate of shoulder instability related to football. Brophy and colleagues 5 reported that among players entering the National Football League Combine, 9.7% had a history of instability and 4.7% had prior shoulder stabilization surgery. Bonza and colleagues 4 demonstrated that high school football accounted for 59% of all high school shoulder injuries and that the rate of shoulder injury is far greater in high school football than any other high school sport, with an injury rate during competition nearly double that of wrestling, the second-most commonly implicated sport (16.2 vs 9.1 per 10,000 exposures). Certainly, other factors may contribute to the Southern predilection for shoulder stabilization procedures; perhaps surgeons in the Northeast are less likely to operate on first-time dislocators, and there may be differences in racial and age demographics among regions (particularly within the Humana database).

Percentage of high school athletes in each state who participate in football.
Limitations
The limitations of this study include the use of a private-payer database from a single insurance provider. This introduces sampling bias, as many athletes with alternative insurance providers are not captured in this analysis. Of note, many patients in the shoulder instability demographic may fall into the Medicaid population. The study is also reliant on accurate surgeon selection of CPT codes. Although the number of arthroscopic stabilizations is likely accurate, it is probable that some surgeons inadvertently mixed up codes 23455 and 23466 (open Bankart and open capsular shift) and 23462 and 23460 (Latarjet coracoid transfer and alternative bone block augmentation) owing to the similarity of procedures. The database is limited in the breadth of information that can be gleaned such that we cannot differentiate between primary and revision procedures, nor can we determine a rationale for bone block augmentation or an alternative open procedure (ie, high-risk demographic, significant glenoid bone loss, or revision procedure). The database offers no information regarding clinical outcomes or complications. Finally, we must caution that “popularity” should not be confused with “efficacy.” Selection of the appropriate surgical procedure should be based on clinical outcome studies and not on trends.
Conclusion
Arthroscopic stabilization remains the most commonly utilized stabilization technique in the United States. The use of Latarjet is steadily increasing and now rivals open Bankart among the most commonly used open stabilization techniques, although it remains a minority among total procedures performed. Arthroscopic stabilization, open Bankart, and Latarjet demonstrate a strong male predominance, while open capsular shift and alternative bone block augmentation are more evenly distributed. Arthroscopic stabilization and Latarjet are most common in the South and least common in the Northeast.
Footnotes
One or more of the authors declared the following potential conflicts of interest or source of funding: B.R.B. receives research support from Arthrex, ConMed Linvatec, DJ Orthopaedics, Ossur, Smith & Nephew, and Tornier and receives publishing royalties from SLACK Inc. N.N.V. receives research support from Arthrex, Arthrosurface, DJ Orthopaedics, Ossur, Smith & Nephew, Athletico, ConMed Linvatec, Miomed, and Mitek; receives publishing royalties from Arthroscopy and Vindico Medical-Orthopedics Hyperguide; has stock/stock options in Cymedica, Minivasive, and Omeros; is a paid consultant for Minivasive, Orthospace, and Smith & Nephew; and receives royalties from Smith & Nephew. A.A.R. receives royalties from Arthrex; is a paid consultant for Arthrex; is a paid speaker for Arthrex; receives research support from Arthrex, DJO Surgical, Ossur, and Smith & Nephew; and receives publishing royalties from Saunders/Mosby-Elsevier and SLACK Inc.
Ethical approval was not sought for the present study.