
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are common in the National Football League (NFL). Limited literature exists regarding return to play (RTP) and the factors affecting RTP after ACL reconstruction in NFL players.
Purpose/Hypothesis:
To determine RTP rates after ACL reconstruction in NFL players and to ascertain which variables affect RTP in these players. We hypothesized that RTP in this population will be less than in the general population and similar to the limited studies published previously.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 92 NFL athletes who sustained ACL injuries requiring ACL reconstruction from 2013 to 2015 were retrospectively studied to determine rate of RTP and the variables affecting RTP.
Results:
Sixty-two percent (57/92) of NFL athletes returned to NFL game play prior to the end of the 2015-2016 postseason. ACL injuries were noted in 10 different player positions, with 81.5% of all injuries as isolated ACL injuries (75/92) and 18.5% with concomitant knee injuries. A significant difference in ability to RTP was found for players who sustained in-season injuries compared with those who sustained off-season/preseason injuries (P = .02). No significant differences in RTP were found for players who played less than 4 years in the NFL compared with those who played longer. The mean draft round of players who returned was 3.96, with the odds ratio favoring RTP at 4.44 (P = .003) for players drafted in the first 3 rounds of the NFL draft compared with those drafted in the fourth round or later. No significant differences were found with regard to playing surface, laterality, concomitant injury, previous ipsilateral or contralateral ACL reconstruction, final outcome of the game, or contact compared with noncontact injuries.
Conclusion:
The RTP rates we reported after ACL reconstruction in NFL players are similar to prior studies; however, running backs and wide receivers had lower rates of RTP than previously reported. As previously published, quarterbacks were found to have high RTP rates. Most ACL injuries take place during the preseason or early regular season. Early selection in the NFL draft was a strong predictor of ability to RTP.
The unique demands placed on the knees of elite athletes competing in the National Football League (NFL) require a highly competent, ligamentously stable knee. Anterior cruciate ligament (ACL) injuries are common in sports involving jumping, pivoting, and cutting such as American football. 2,5 ACL injuries are among the most common sporting injuries to the knee, 13 with data to suggest that as many as 8% of all participants at the NFL Combine have a history of ACL injury. 3,4 The sport of football may place a player at risk for ACL injury at a rate up to 10 times higher than other sports. 8 The ultimate goal of all players with an ACL injury is to return to their sport at as close to previous performance level as possible—one that is becoming more realistic with modern treatment methods, with some studies reporting a >90% rate of return to preinjury sporting level in the general population. 6,14,15 To return to such a level, ACL reconstruction is performed in an effort to maximize the functional capacity and stability of the ACL, 2 with many authors recommending reconstruction in young athletes desiring to continue athletic competition. 14
Multiple factors affect the ability to perform in an elite capacity after ACL reconstruction, including previous physical conditioning and access to optimal rehabilitation after surgery. 14 In professional sports, other factors such as roster and personnel needs as well as economic factors such as salary cap restrictions or costs spent on high-priced free agents or high draft picks likely also play a role in a player’s return to the field. Literature regarding the modifying factors surrounding ACL injury among NFL athletes is relatively sparse in comparison with data among other athletes and less competitive football players. 5,6,9,12,13 Certain variables, such as the player’s position, concomitant knee injury, draft round, and games played prior to injury, have been assessed, but many of these studies discussed limitations due to small sample size. 5,14 The purpose of this study was to provide a larger cohort from a different time period and validate previously assessed variables affecting return to play (RTP) in NFL athletes after ACL reconstruction. We believed that the RTP rate in this special subset of patients will be lower than that of the general population.
Methods
After receiving exempt status from our institutional review board, data were gathered from player databases on publicly accessible websites such as www.NFL.com, www.CBSSports.com, and www.ESPN.com, as well as post-game summaries on the same publically accessible websites. Information regarding each player’s age, years played in NFL, draft position, date of injury, site of injury, field surface, mechanism of injury, concomitant injury, previous reconstructions, player position, time of injury relative to game situation, and outcome of game on date of injury was also found on these websites. For inclusion in this study, each athlete was required to be an active member on an NFL roster at the time of injury, and the injury must have occurred after the 2013 Super Bowl, between the offseason/preseason prior to the 2013-2014 season, and the end of the 2014-2015 NFL postseason. For the purposes of this study, similar to previous investigations, return to play was defined as playing at least 1 down in a regular-season NFL football game during the 2013-2014, 2014-2015, or 2015-2016 NFL seasons after ACL reconstruction, 14 and at least 1 full NFL season had elapsed since reconstruction for all athletes included in this study. Athletes who sustained injuries or underwent ACL reconstruction after the 2014-2015 NFL season were excluded from this study because of insufficient follow-up time regarding RTP status. In cases in which sufficient data regarding variables for this study were unable to be found on the 3 websites provided, supplemental usage of NFL team websites and publicly accessible, reputable news sources such as online newspaper articles from individual cities and reports from NFL writers from ESPN, CBS Sports, NBC Sports, and FOX Sports were used to obtain data points.
Statistical analysis was done using logistic regression with SAS software (version 9.4; SAS Institute).
Results
A total of 92 NFL players met the inclusion criteria for this study. Seventy-four of these athletes (80.4%) sustained ACL injuries requiring ACL reconstruction early in the season, which was defined as the preseason through week 8 of the NFL season. Eighteen athletes (19.6%) sustained ACL injuries late in the season, defined as week 9 through the end of the NFL playoffs. Concomitant knee injuries were seen in 17 players (18.5%), while the other 75 NFL players (81.5%) were reported as having sustained isolated ACL injuries. Two players sustained ACL injuries in both seasons studied, 1 of whom was able to return to the field for the 2015-2016 season while the other was not. Both players sustained ipsilateral ACL injuries, with the second injury occurring to their previously reconstructed ACL.
The mean age of the 92 NFL athletes was 25.96 years at time of reconstruction, and the mean years played in the NFL prior to reconstruction was 3.89 years. Among our 92 athletes, ACL injuries were noted in 10 different player positions, with the greatest representation seen in wide receivers (WRs) at 19 (20.6%), representing a 5.3% incidence of injury among all NFL WRs; defensive linemen (DLs) at 16 (17.4%), a 4.6% incidence; linebackers (LBs) at 15 (16.3%), a 4% incidence; and offensive linemen (OLs) at 12 (13.6%), a 2.9% incidence (Table 1).
Return to Play by Positiona
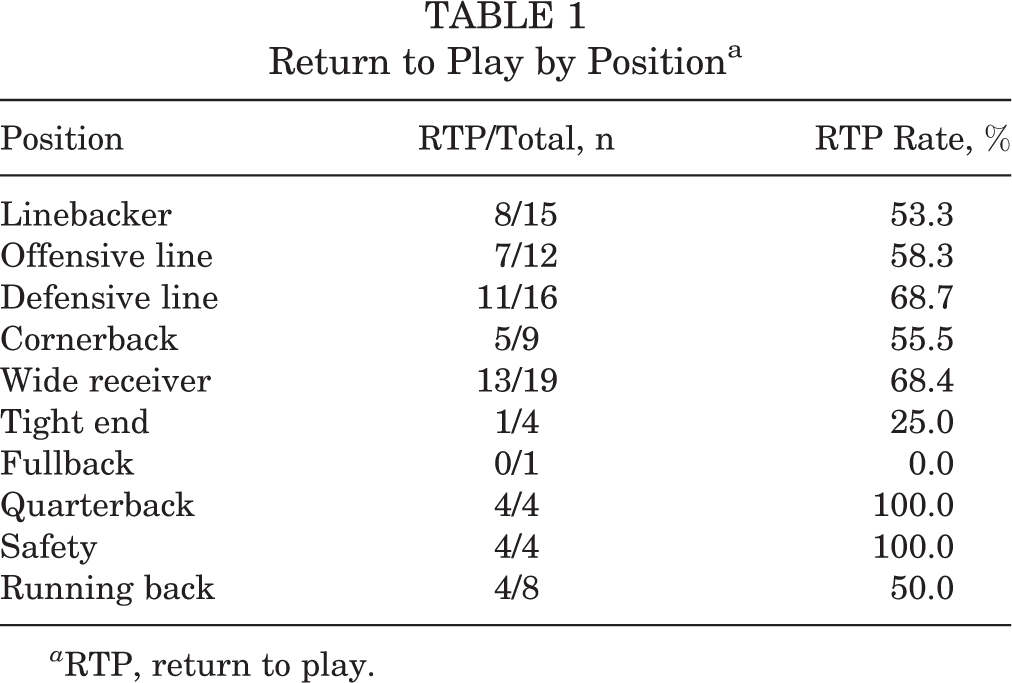
a RTP, return to play.
Of the 92 NFL players, 57 (62%) were able to return to the field during the allotted time period. All positions had a >50% RTP rate except for fullbacks (FBs) (0/1, 0%) and tight ends (TEs) (1/4, 25%). The greatest RTP percentage was seen among quarterbacks (QBs) and safetys (4/4, 100% for both), followed by DLs (11/16, 68.7%) and WRs (13/19, 68.4%), OLs (7/12, 58.3%), cornerbacks (CBs) (5/9, 55.5%), and LBs (8/15, 53.3%) (Table 1). There was no statistically significant difference in RTP rates whether the injury occurred during offensive, defensive, or special teams play. In addition, there were no significant differences in RTP rates between early-game injuries (those occurring in the first half) and late-game injuries (those occurring in the second half) or between early-season injuries (preseason through week 8) compared with late-season injuries (week 9 and beyond). However, when the season was stratified as preseason compared with in-season injury, players who sustained an in-season injury were 3 times as likely to RTP than those who sustained preseason injuries (odds ratio [OR], 3.0 [95% CI, 1.24-7.28]; P = .02) (Table 2). The mean number of years played in the NFL for RTP players was 3.84 years, compared with 3.97 years for non-RTP players (P = .83). Of athletes who played less than 4 years, 64% (34/53) were able to RTP, compared with 59% (23/39) of those who played more than 4 years, but no statistically significant difference was found between these groups (OR, 0.98 [95% CI, 0.84-1.15]; P = .61) (Table 2). There was a significant difference found for RTP in terms of whether the player was an early draft pick (rounds 1-3 of the NFL draft) compared with a late-round draft pick (rounds 4-7 or undrafted). Of those drafted in the first 3 rounds of the NFL draft, 81% were able to RTP, compared with 49% of players drafted after round 3. Players who were drafted early had 4.44-times rate in RTP ability (OR, 4.44 [95% CI, 1.67-11.82]; P = .003) (Table 2).
Comparison Between RTP and non-RTP groups a

a Boldfaced P values indicate statistical significance. ACL, anterior cruciate ligament; RTP, return to play.
b Insufficient data regarding 3 injured athletes.
c Insufficient data regarding 10 injured athletes.
d Insufficient data regarding 34 injured athletes.
e Forty-five injuries did not occur during National Football League game play.
f Insufficient data regarding 13 injured athletes.
g Insufficient data regarding 15 injured athletes.
h Insufficient data regarding 5 injured athletes, and 40 injuries did not occur during game play.
No significant differences in RTP rates were found with regard to playing surface, laterality, concomitant injury, previous ipsilateral or contralateral ACL reconstruction, final outcome of the game, or contact and noncontact injuries.
Discussion
Similar to previous studies, 6,7,14,15 our larger cohort was able to demonstrate a lower RTP rate among NFL players compared with the general population. Predicting and improving the ability to return to previous activity level after ACL reconstruction can be a powerful tool, especially in the high-demand, high-stakes environment of professional football. Previous studies have looked at different levels of competitive play in different sports, including football, rugby, soccer, bicycling, skiing, running, and tennis, with a range of quoted RTP rates from 18% to 100%. 1,2,5 –7,11,14,15 Recently, Shah et al 14 reported on 49 NFL players who underwent ACL reconstruction at a single institution and found a 63% rate in RTP ability. The results in our larger cohort, from a different time period, are very similar, with an overall RTP rate of 62%. When evaluating the RTP ability of WRs and running backs, this subset demonstrated a 63% RTP rate, while other studies have shown a much higher rate of 75% to 79%. 5,14 Interestingly, aside from validating the overall RTP rate among NFL players, we found QBs to have the highest RTP rate at 100%. This is consistent with previous studies demonstrating a 92% to 100% rate in QBs returning to their previous level of competition. This may reflect the high success rate of ACL reconstruction and RTP rate of this position, as studies have found an equal number of QBs at the NFL Combine enter the league with and without previous ACL injury, and there are no performance differences between those who have native or reconstructed ACLs. 3,4,11,14
Our study demonstrates that injury tends to occur early in the league year, with 80% occurring prior to week 8 of the season, similar to the recent study by Shah et al 14 in which the majority of injuries in that cohort also occurred during the preseason or early regular season. This may be a result of inadequate preseason conditioning versus players playing harder to earn positions that are more fluid in the preseason or early season. While an ACL injury is essentially a season-ending event, the early timing of the injury relative to an individual season allows a greater likelihood of readiness for the upcoming season. 10,11 The ability to RTP within 1 year has been reported clinically in multiple studies as well as basic science research. 6,10,13,14 Clinically, no differences in graft rupture risk compared with contralateral native rupture have been found at 12 months postoperatively; additionally, histologic studies have shown changes in grafts over this time as they mature and begin to resemble the native tissues. 6,10,13,14 We found statistical significance in RTP ability if the injury happened during the season compared with the preseason or off-season as well as in those players drafted in the early rounds of the NFL draft. Though several potential reasons for this disparity exist, one explanation is that some of the injuries that occurred during the preseason involved players who were later released. The injury may have affected these players’ abilities to earn a roster spot, as their recovery time did not allow them to compete with other players at their position. Higher drafted players also represent a larger investment for teams, making rehabilitation for these players more of a priority rather than looking for a replacement. The mean draft round of RTP players was 3.96 compared with 5.51 for non-RTP players. This compares favorably with previously reported draft rounds of 3.4 in players able to return and 6.4 in players who did not. 14 RTP rates could be affected in these individuals due to financial commitment and overall investment made to higher draft picks by various teams rather than actual surgical outcomes of the ACL reconstruction. Though this significant finding was reported in previous literature, the reason for greater RTP rates in early round draft picks is likely highly individualized and multifactorial. Therefore, this finding cannot be completely explained by the data alone without other context. Similar to Shah et al, 14 the mean number of seasons played in the RTP group compared with the non-RTP group was 3.84 and 3.97, respectively, with no statistical significance.
We found no significant difference in players with concomitant injuries or previous ipsilateral or contralateral reconstruction. Our rates of concomitant injury are low compared with previous publications. This finding is likely due to underreporting of intraoperative findings or more complex injury patterns by the publicly accessible data we queried. As such, we were not able to stratify the concomitant injury or the treatment for said injury. This lack of significant difference in RTP rates between players with and without concomitant injury is similar to the findings of Shah et al, 14 in which 75% of their cohort had concomitant injuries addressed at the time of reconstruction, with no significant difference in RTP rate for those who had an isolated ACL reconstruction.
Most of our injuries occurred on a grass playing field (83%), despite nearly half (48%) of NFL stadiums using artificial turf. This is in contrast to previous studies that have reported an increased risk of ACL tear on artificial surfaces. There was no significant association with RTP ability and playing surface. 8,9
Our study does have inherent weaknesses that may affect our findings. Unlike previous studies in which all procedures were performed at a single institution with access to specific patient and procedure information, our data were based solely on public information available on the Internet. 14 Thus, we do not know whether concomitant procedures were performed on these athletes. These may include, but are not limited to, cartilage restoration, differing techniques for ACL reconstruction, and concomitant injuries. As a result, this likely underreporting of concomitant injuries is conceded by the authors. Previous publications allowed a minimum of 2 full seasons to evaluate for potential RTP, while this study considered only the subsequent year for those players who were injured during the 2014-2015 NFL season. Because of this limitation, our study may underestimate the total number of athletes who are able to RTP. 14 We also did not report on longevity after reconstruction and were limited to a 2-year time frame. Previous studies, however, have found similar length of careers in the NFL with and without ACL reconstruction. 3,4 Although Shah et al 14 reported differences in the number of games and seasons played before and after injury, confounding is present. Injured players have already played a portion of their careers, and thus the lesser number of seasons and games played after surgery may be due to the natural process of players retiring at the end of their careers and not to inferiority of their reconstructed knees.
One of the strengths of our study is the large size of the cohort studied, nearly doubling the number of players available for review compared with prior reports. With 92 players available for review compared with 49 and 31 in previous studies dedicated to NFL athletes, we were able to validate previous findings, specifically the overall RTP rate among all positions, the high RTP rate for QBs, the lack of association between concomitant injuries or procedures with RTP ability, the high incidence of injury early in the season, and the RTP ability of early draft picks. 5,10,11,14 Our study, besides having increased power, is also more inclusive as all positions were evaluated and multiple surgeons and sports medicine teams were involved in treating these injuries, thus avoiding selection bias.
Conclusion
With a 62% RTP rate in the NFL, the return to previous activity level is not as high as seen in other sports or other levels of competitive play. 14 Our study provides a broad look at ACL injuries in the NFL, with associated outcomes as measured by RTP ability. The ability to return to sports was significantly associated with higher draft status and in-season injury. While RTP ability is likely multifactorial, this finding can be interpreted as players who achieved RTP both possessing more talent as well as representing a larger investment by teams. This creates a larger incentive to return to the playing field, both for the athletes involved and the organizations they represent.
Footnotes
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of Defense or United States government.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.T.L. is a teaching consultant for Cayenne and hold stock in Stryker.