
Abstract
Background:
Quantifying glenohumeral bone loss is key in preoperative surgical planning for a successful Bankart repair.
Hypothesis:
Simple radiographs can accurately measure bone defects in cases of recurrent shoulder instability.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
A true anteroposterior (AP) view, alone and in combination with an axillary view, was used to evaluate the diagnostic properties of radiographs compared with computed tomography (CT) scan, the current gold standard, to predict significant bone defects in 70 patients. Sensitivity, specificity, and positive and negative predictive values were evaluated and compared.
Results:
Detection of glenoid bone loss on plain film radiographs, with and without axillary view, had a sensitivity of 86% for both views and a specificity of 73% and 64% with and without the axillary view, respectively. For detection of humeral bone loss, the sensitivity was 8% and 17% and the specificity was 98% and 91% with and without the axillary view, respectively. Regular radiographs would have missed 1 instance of significant bone loss on the glenoid side and 20 on the humeral side. Interobserver reliabilities were moderate for glenoid detection (κ = 0.473-0.503) and poor for the humeral side (κ = 0.278-0.336).
Conclusion:
Regular radiographs showed suboptimal sensitivity, specificity, and reliability. Therefore, CT scan should be considered in the treatment algorithm for accurate quantification of bone loss to prevent high rates of recurrent instability.
Keywords
Traumatic anterior shoulder instability affects up to 1.7% of the population, 10,36 and half of these patients will develop symptoms of chronic instability and significant functional deficits. 23 The essential anatomic reason for recurrent instability is detachment of the anterior labrum and the anteroinferior glenohumeral ligament, known as the Bankart lesion. Surgical treatment may involve reattachment of the Bankart lesion, and since the 1990s, the procedure has been carried out arthroscopically with suture anchors. The rate of failure, or dislocation rate, is reported to be from 10% to 50%. 7,8,17 Burkhart and De Beer 11 were the first to describe one of the underlying causes of failure: a concomitant bone defect on the glenoid. The “inverted pear deformity,” which represents a loss of at least 25% of the width of the inferior glenoid, contributes to a loss of bony support. 26 Authors such as Cho et al, 16 Armitage et al, 1 and Cetik et al, 15 among others, 4,28,30 have described the importance of bone loss of the posterior humeral head (the Hill-Sachs lesion) as another contributing factor in failure of an arthroscopic Bankart repair. However, no consensus has been found in either the quantification methods or the threshold. 21,25,26,32,39 The Instability Severity Index Score, described by Balg and Boileau, 5 includes bone loss of the anteroinferior glenoid and the posterior humeral head as a means of quantifying the risk for failure of an arthroscopic Bankart repair. The Instability Severity Index Score combines bone loss with other risk factors for failure and informs the treatment approach for patients with recurrent anterior shoulder instability. 5 A higher score indicates that an alternative procedure such as a Latarjet or an additional procedure such as a remplissage should be considered as part of surgical planning. 18
Preoperative identification and quantification of these bone lesions can be difficult, leading to challenges associated with surgical decision making. Imaging, particularly radiography, can potentially underestimate bone defects. Nonetheless, in an international survey of 197 surgeons published in 2016, only 27% said that they requested computed tomography (CT) scanning in their evaluation of patients with recurrent instability. 38 The disadvantage of CT scans is the additional radiation exposure, and it has been suggested that CT be used only if the alternative imaging modalities fail to provide sufficient diagnostic information. 22 Although it is universally acknowledged that the recognition of glenohumeral bone loss is a key component of surgical decision making, no universally accepted preoperative approach to quantifying bone loss exists, which leads to a high degree of subjectivity in this analysis. 9
The primary objective of this study was to evaluate the diagnostic properties of radiographs, including the sensitivity, specificity, and positive and negative predictive values of a true anteroposterior (AP) view, alone and in combination with an axillary view, to predict significant bone defects; CT scan was used as a gold standard. The secondary objectives were, first, to evaluate the inter- and intraobserver reliabilities of these views for the identification of bone loss involving the glenoid and humerus and, second, to identify radiographic and patient characteristics associated with significant bone loss.
Methods
Participants
Participants were drawn from a consecutive series of patients with recurrent traumatic anterior shoulder instability, treated between 2008 and 2012, who had been used to validate a French-language version of the Western Ontario Shoulder Instability questionnaire. 19,24 Additional participants were drawn from a further consecutive series of patients with recurrent traumatic anterior shoulder instability who had been treated between 2012 and 2013 by the senior author (D.M.R.). According to Landis and Koch, 27 a kappa between 0.61 and 0.80 is considered substantial agreement. To detect a kappa of 0.70 between 2 readers, 70 patients were required (α = .05, β = 0.20).
Patients identified for inclusion in the study had a glenohumeral true AP and axillary lateral radiograph as well as a CT scan of the affected shoulder (helical CT acquisition; thickness, 1.25 mm; interval, 0.625 mm). Additional inclusion criteria were age older than 16 years and an ability to provide informed consent. Individuals with open growth plates visible on radiograph and those missing any of the 2 radiograph views or CT scan were excluded from the study. Ethics committee approval was obtained for the study, and all patients provided informed consent.
Each surgeon was asked to classify the bone defect of the glenoid and humeral head separately and to describe it as either absent, present but not clinically significant, present and clinically significant, or unable to assess. The surgeons were then asked to provide a subjective opinion on whether the glenoid or humeral head bone loss independently put the patient at risk for failure of an arthroscopic Bankart repair, as defined by the Instability Severity Index Score. 5
Radiograph Standard Method
The axillary view was taken with the patient standing with the arm abducted at 90° and the shoulder in neutral rotation. The beam was directed in the axilla. For the true AP view, the beam was directed in line with the plane of the glenoid joint surface with the humerus in internal rotation and maximal external rotation (Figure 1).
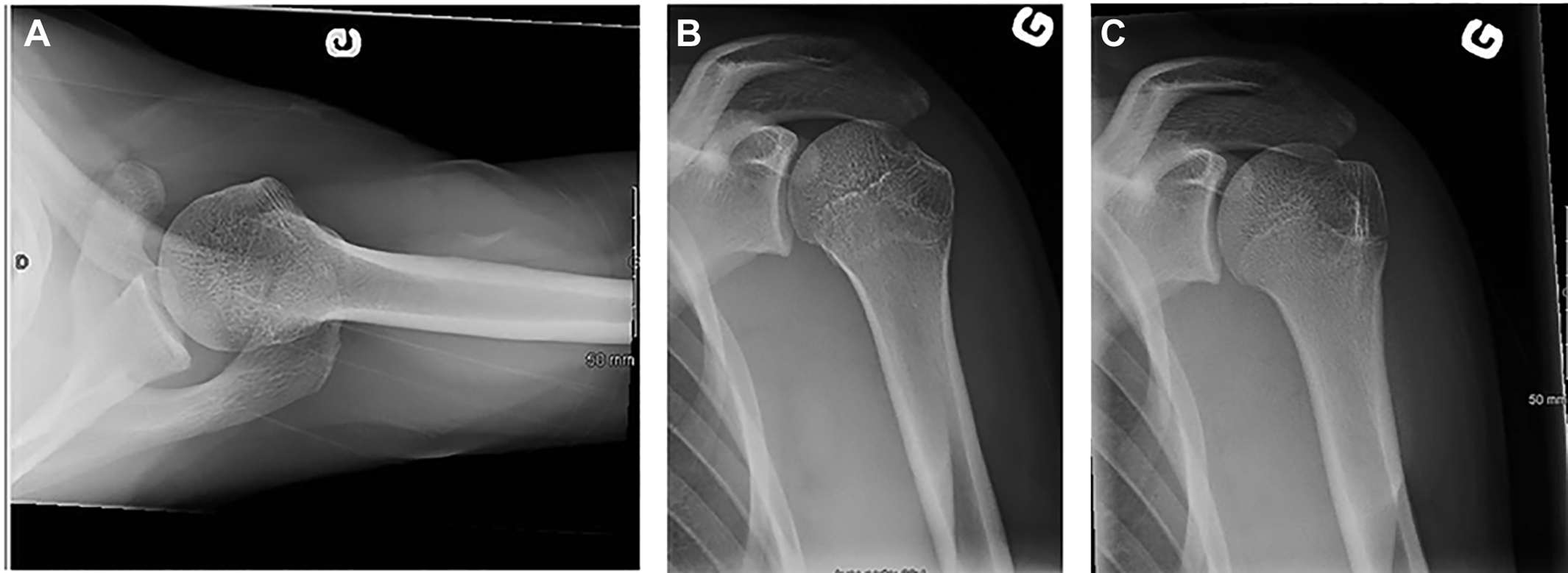
(A) Axillary view. (B) Anteroposterior view of the glenoid with the humerus in internal rotation and (C) maximal external rotation.
CT Evaluation and Bone Loss Calculation
An engineer trained in musculoskeletal imaging assessment evaluated the CT scans of the 70 patients by using CATIA software (CATIA V5R21; Dassault Systèmes). Two methods were used to calculate glenoid bone loss—the surface area method (Figure 2) and the glenoid ratio method 6 (Figure 3)—while the humeral ratio method 21 (Figure 4) was used to calculate humeral bone loss. En face views of the glenoid on 3-dimensional (3D) CT were used to calculate glenoid bone loss, and axial CT views of the humerus were used to calculate humeral bone loss, according to the published method. The mean value of the 2 methods for calculating glenoid bone loss was used. Bone loss/expressed as a percentage was calculated for the glenoid and humerus independently and was classified as absent, present but not clinically significant (bone loss ≤20% on the glenoid and/or humerus), or present and clinically significant (bone loss >20%). 21

(A) Example of a 24-year-old male with significant bone defect. (B) The surface area method measures bone defect as the surface area of missing bone. On a 3-dimensional reconstruction of a scapula, the formula is A2/A1 × 100%, where A1 is the entire surface area of the best-fit circle and A2 is the surface area of the bone defect.

The glenoid ratio method is an estimation of the missing bone surface using values R and d in a formula (d/R) (Barchilon et al 6 ).

The humeral ratio method (W/di) (Hardy et al 21 ) uses an axial view of the humerus. Di is the diameter, W is the width, and De is the depth of the bone defect.
Reliability Assessment
For the purposes of assessing inter- and intraobserver reliability, de-identified digital radiographs of the 70 patients were analyzed twice: The first viewing showed the glenohumeral true AP view and the second viewing was of both the true AP and axillary lateral views. The 2 presentations were reviewed by 4 fellowship-trained shoulder surgeons (F.B., M.J.B., D.M.S., P.L.) who were blinded to the patients’ clinical history and CT scan findings. The surgeons reviewed the 2 presentations at 2 separate intervals, approximately 1 week apart. The order of the radiographs was randomly altered between the first and second readings by a research assistant.
Statistical Analysis
The test characteristics for detecting bone defects, including sensitivity, specificity, and positive and negative predictive values, were determined for the true AP with and without an axillary view. In addition, the number of clinically significant bone defects missed on plain radiography was determined.
Kappa statistics were used to determine the inter- and intraobserver reliability of plain radiographs for the detection of bone loss. Landis and Koch 27 characterized a kappa of 0.41 to 0.60 as moderate, 0.61 to 0.80 as substantial, and 0.81 to 1 as almost perfect agreement. Radiographic performance will be compared to the gold standard, the CT-scan, as well as by sensitivity and specificity, to be classified as low or high. 34
The degree of association between the presence of significant bone defects and demographic and radiographic data was determined by Pearson correlation coefficients and the Mann-Whitney U test.
Results
Demographics
A total of 121 patients were reviewed for this study; 6 patients did not have the required radiographs, 31 did not have a CT scan, and 14 did not meet the inclusion criteria, leaving a total of 70 participants with preoperative imaging. The participants were 62 men and 8 women with recurrent anterior shoulder instability, with a mean age of 27 years (range, 16-63 years); the dominant side was involved in 34 patients. Forty-seven patients recalled the time of their first dislocation, and in this group the mean time between first dislocation and radiograph completion was 78 days (range, 0-495 days). The mean number of dislocations and subluxations was 16 (range, 2-100).
Sensitivity, Specificity, and Positive and Negative Predictive Values
Analysis of the CT scans revealed that 6 patients had ≥20% bone loss involving the glenoid and 25 patients had ≥20% bone loss on the humeral side. The presence or absence of clinically significant bone loss on the glenoid or humerus on plain radiographs was determined by consensus of the reviewers’ independent evaluations. If perfect consensus was not achieved, bone loss was considered present or absent when there was more than 50% agreement on the evaluation (Tables 1 and 2).
Sensitivity and Specificity of Glenoid Bone Loss Detection on Plain Radiographs Compared With CT Scans a

a AP, anteroposterior; AX, axillary; CT, computed tomography; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
b Sensitivity, 85.7%; specificity, 63.5%.
c Sensitivity, 85.7%; specificity, 73.0%.
Sensitivity and Specificity of Humeral Bone Loss Detection on Plain Radiographs Compared With CT Scans a
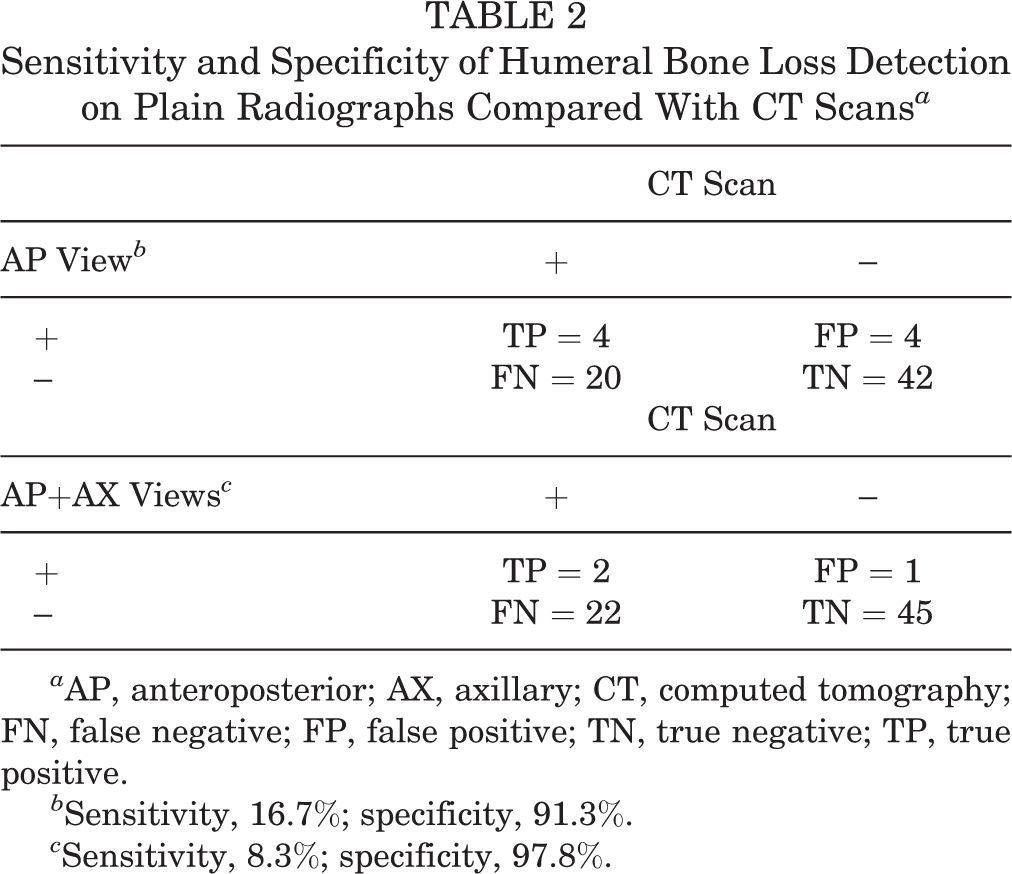
a AP, anteroposterior; AX, axillary; CT, computed tomography; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
b Sensitivity, 16.7%; specificity, 91.3%.
c Sensitivity, 8.3%; specificity, 97.8%.
For detection of glenoid bone loss on plain radiographs, the sensitivity was 86% both with and without the axillary view, and the specificity was 73% with and 64% without the axillary view. For detection of humeral bone loss, the sensitivity was 8% and 17% with and without the axillary view, respectively, and the specificity was 98% and 91% with and without the axillary view, respectively.
Inter- and Intraobserver Reliability
Glenoid Bone Loss
The mean intraobserver reliability was moderate for glenoid detection, with κ = 0.503 for true AP view and κ = 0.473 for true AP + axillary views. The mean intraobserver reliability was κ = 0.7 for true AP and 0.633 for true AP + axillary views (Table 3).
Intraobserver and Interobserver Reliabilities for Plain Radiographic Detection of Bone Defects on the Glenoid and the Humerus Using True AP View and True AP and Axillary Views a
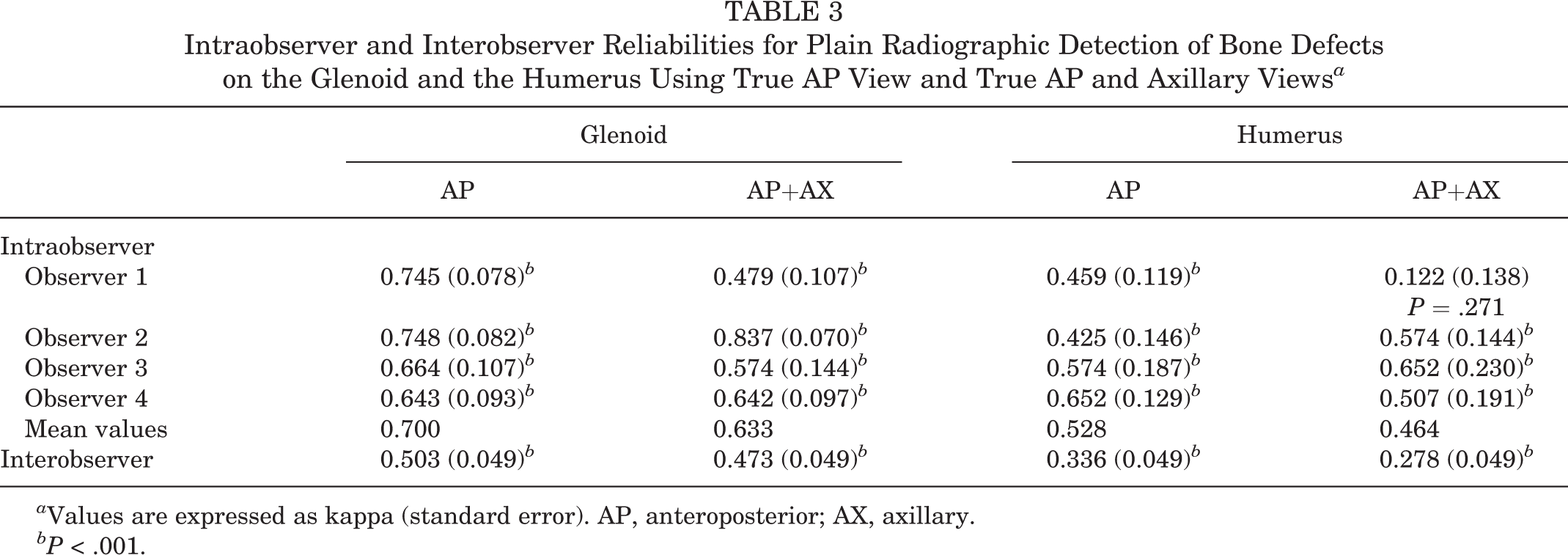
a Values are expressed as kappa (standard error). AP, anteroposterior; AX, axillary.
b P < .001.
Humeral Bone Loss
The reliability of plain true AP radiographic assessment between evaluators was poor, with κ = 0.336 for true AP view and κ = 0.278 for true AP + axillary views. A slightly higher mean value was observed for intraobserver reliability (κ = 0.528 for true AP and κ = 0.464 for AP + axillary views) (Table 3).
Predictors of Severity of Bone Loss
Using the CT-based methods of quantifying bone loss on the glenoid and humerus, we observed no statistical differences for any of the 3 methods between males and females according to the Mann-Whitney U test: glenoid area method (7% in females, 9% in males, P = .7); glenoid ratio method (5% in females, 8% in males, P = .7), and humeral area method (7% in females, 8% in males, P = .3).
Age was not associated with the severity of the bone defect (glenoid area, r = –0.165, P = .173; glenoid ratio, r = –0.131, P = .283, humeral area, r = 0.095, P = .432).
The number of dislocations was moderately related to the degree of bone loss on the glenoid side (r = 0.424, P = .001 for the glenoid area method; r = 0.505, P = .001 for glenoid ratio method). The association was not statistically significant with the humeral area method (r = 0.178, P = .181).
Discussion
The main purpose of this study was to determine the diagnostic properties, sensitivity, and specificity of standard AP radiographs, with and without axillary view, to identify significant bone loss on the glenoid and humeral sides in a population known for recurrent shoulder instability, using the CT scan as the gold standard. Our goal was to emphasize the need for detailed preoperative radiological examination in this population, with the hope of eventually minimizing misdiagnosis and diminishing postoperative recurrences. According to our results, regular radiographs would have missed 1 instance of significant bone loss on the glenoid side and 20 on the humeral side.
Tauber et al 37 reported that approximately 50% of their revision cases had bony glenoid rim defects, demonstrating that a nonreconstructed bony glenoid rim plays a major role in postoperative failure. Interestingly, Bigliani et al 7 asserted that CT arthrography gave the best overall visualization of the fracture and yielded the highest diagnostic accuracy rate in their study, as did Milano et al. 29
Bushnell et al 13 stated that recent literature has identified unrecognized large bony lesions as difficult to diagnose and a primary cause of arthroscopic reconstruction failure for instability, as well as a major cause of recurrent instability. Those authors also mentioned a limited sensitivity in detecting the bony lesions. 14
Thus, we assumed that standard radiological imaging was insufficient for detecting bone loss after recurrent dislocation of the shoulder, as found in these previous studies.
At the beginning of the study, we supposed that the addition of the axillary view to the AP view would enhance the diagnostic properties for both sensitivity and specificity. The results have shown that this hypothesis is invalid. The possibility that sensitivity is relatively low because of the low number of actual positives in the series, causing the magnitude effect of 1 false negative to therefore be high, should also be considered.
Interestingly, the results are quite different for humeral bone loss. As anticipated, the sensitivity was low (8%-17%) and the specificity high (91.3%-97.8%). These results show that radiography alone cannot be used to detect bone loss on the humeral side. Once again, our primary hypothesis was invalidated; the axillary view did not help the evaluators determine significant bone loss when added to the AP view. This also applies to the intraobserver and interobserver reliabilities, which were not significantly different from those obtained with the addition of the axillary view. Perhaps the eye of the evaluator does not need this additional information and can rely simply on the AP view.
The degree of bone loss was correlated with the number of previous dislocations on the glenoid side, but for unknown reasons this did not seem to be the case on the humeral side. Further investigation is needed to explore the causes for this discrepancy. 29
This study has some limitations, beginning with the method of evaluation, which was based on observation. We realize that with the kappa statistic, the fidelity of our results may be compromised by the subjectivity of the evaluators. To help minimize this we chose evaluators with significant experience in the studied domain, and the statistical tests used were appropriate for the intended goals of this study. Also, the prevalence of significant bone loss on the glenoid side was relatively low. Our findings may have been different if we had used a lower threshold for bone loss. Another limitation is the absence of a combined evaluation of bone defect or the glenoid track concepts that have been reported as useful tools in the recent literature. 20,31,35 However, these methods are not commonly used in regular surgical practice, as opposed to static 3D-CT scans and radiographs. Some authors have advocated for specific plain radiographic views (eg, West Point view) as a means of better detecting bone loss, which was not addressed in this article. Finally, the participants who were recruited for this study were taken from a database of a specific population, thus we must be sure not to generalize them to a population with different demographic data. Indeed, the cases studied were taken from a tertiary center in upper limb surgery and may not reflect the patients in other centers.
When we compare our results with other studies, we do appear to come to the same conclusion. Auffarth et al 2,3 indicated that radiographs appear to be inferior to CT scans for evaluating osseous lesions after a primary dislocation. Those authors also suggested performing a CT scan of the shoulder after primary dislocation to apply the correct treatment early and potentially avoid further dislocations. Multiple radiographic studies for the evaluation of glenoid bone loss are available; however, the 3D reformatted CT scan provides the most accurate assessment of bone deficiency or combined glenoid and humeral head defects. 12,30,33 Although outside the scope of this analysis, other studies have shown that 3D MRI could be equivalent to CT scan in bone loss quantification, meaning that CT scan or MRI could be used interchangeably. 40
Like us, other authors and recent studies demonstrate that radiographs of the shoulder may falsify osseous lesions in dislocated shoulders. To our knowledge, this study is the first investigation to evaluate the sensitivity and specificity of radiography using the AP view, both alone and in combination with the axillary view, and comparing the results with CT scan.
This leads us to novel and interesting questions regarding the increased cost analysis of a CT scan. Is the use of CT justified by a decreased overall cost if it prevents more recurrence? It is also becoming clear, based on the work of multiple centers, that plain radiographs are not sufficient as part of the scoring system. Would it be wise for us to consider an enhanced scoring system to evaluate the need for Latarjet surgery or an arthroscopic Bankart procedure with or without remplissage?
Conclusion
Intraobserver and interobserver reliabilities in the assessment of plain films for the detection of bone loss were moderate to substantial for glenoid bone loss and poor to moderate for humeral bone loss. Given the suboptimal sensitivity and specificity of the plain films even with axillary view for the detection of significant bone defects, CT scan should be routinely considered in the treatment algorithm for accurate quantification of bone loss to minimize the rate of recurrent instability.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: D.M.R. is a consultant for Bioventus and Wright Medical. The Hôpital du Sacré-Cœur de Montréal receives institutional funding from Arthrex, ConMed, Depuy, Linvatec, Smith & Nephew, Stryker, Synthes, Tornier, Zimmer, and Wright Medical.
Ethical approval for this study was obtained from the Hôpital du Sacré-Cœur de Montréal, Montréal, Québec, Canada (CÉR: 2012-783).