
Abstract
Background:
Surgical management of anterior shoulder instability continues to evolve. The clinical effectiveness of arthroscopic Bankart repair with remplissage (REMP) in patients with increasing glenoid bone loss (GBL) has not been thoroughly compared with Latarjet.
Purpose/Hypothesis:
The purpose of this study was to compare 2-year outcomes of REMP versus open Latarjet in patients with >15% GBL. We hypothesized that there would be no difference.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A multicenter, retrospective study was performed on a consecutive series of patients who underwent primary REMP or Latarjet by 4 shoulder specialists between August 2013 and December 2019 for >15% GBL. Procedure performance was based on shared decision making between the surgeon and patient. Baseline and 2-year postoperative range of motion (ROM) and the following patient-reported outcomes (PROs) were collected: Western Ontario Shoulder Instability Index, Single Assessment Numeric Evaluation, and visual analog scale for pain. Return to sport, satisfaction, complications, recurrence, and revisions were reviewed.
Results:
A total of 47 patients were available for study, including 22 who underwent REMP and 25 who underwent Latarjet. Baseline demographic characteristics, ROM, and PROs were similar between the groups. Mean preoperative GBL (REMP 25.8% ± 7.8% vs Latarjet 25.1% ± 9.0%; P = .800) and off-track lesions (REMP 59.1% vs Latarjet 44.0%; P = .302) were similar. Postoperative change in external rotation favored Latarjet (10° ± 22° vs –4° ± 13°; P = .017). Postoperative PROs, return to the sports (86.4% vs 87.5%; P = .99), and satisfaction (95.5% vs 95.8%; P = .99) were similar between groups. There were no recurrent dislocations in either group. One infected hematoma was encountered in the Latarjet cohort.
Conclusion:
At short-term follow-up, the hypothesis was upheld. REMP and Latarjet provided similar outcomes for patients with >15% GBL, although REMP patients experienced slightly decreased external rotation. Although larger series and longer-term follow-ups are required, remplissage may be considered in patients with >15% glenoid bone loss.
Keywords
The lack of bony constraint in the glenohumeral joint has provided it with incredible mobility. This has been quite useful for daily activities, but it also has led to the glenohumeral joint’s being the most commonly dislocated joint of the human body. 17,19 Anterior instability is its most common form (90%) and is more prevalent in male patients, contact athletes, and military personnel. 17,19 This commonly leads to capsulolabral injury as well as bony (glenoid and humeral) defects. 10,17,26,36 Addressing these pathologies is imperative to decrease the risk of further dislocation, bony destruction, and patient morbidity over time. 5,16,36
The optimal surgical management of anterior shoulder instability continues to be debated. Although soft tissue concerns and patient characteristics influence treatment, actual surgical decision making is often dictated by bone loss and the glenoid track concept. The glenoid track equation has been popularized as a way for surgeons to determine whether a humeral Hill-Sachs lesion will fall off the glenoid track and result in anterior shoulder dislocation, an “off-track” lesion. 5,10,16,36,40 Although certainly not universal, a popular algorithm is to perform isolated Bankart repair for on-track patients with minimal bone loss, arthroscopic Bankart repair with remplissage (REMP) for off-track patients with subcritical bone loss, and open Latarjet for patients with critical glenoid bone loss (GBL). 36 However, the definition of critical bone loss is unresolved and can range from 15% to 25% GBL. 36,38,39 This comes in an era when there is increasing use of bony augmentation procedures, whether for primary or revision procedures. 7,20 REMP has been shown to be both safe and effective for patients who have subcritical bone loss when compared with isolated Bankart repair. 11,12,27,30,31 Investigators have noted similar results when comparing REMP and Latarjet for off-track patients with subcritical bone loss, and both procedures offer a low recurrent dislocation profile, although REMP may be associated with fewer complications. 2,4,13,15,24 Although REMP is increasingly recognized as a powerful tool in the shoulder surgeon’s armamentarium, it has not been adequately compared with Latarjet in patients with high levels of bone loss (ie, >15%), and one may consider whether its use could be expanded to patients with increasing GBL.
The purpose of this study was to compare 2-year outcomes of REMP versus open Latarjet in patients with >15% GBL. The hypothesis was that there would be similar functional outcomes and recurrence between the groups.
Methods
A multicenter, retrospective review was performed of prospectively collected data between August 2013 and December 2019, spanning 4 international sites on 3 continents. Inclusion criteria were primary surgery for anterior glenohumeral instability managed with either REMP or open Latarjet with >15% GBL and a minimum postoperative follow-up of 2 years. Exclusions were patients not entering the outcomes registry, patients with <15% GBL, patients who had revision surgery, and patients for whom baseline and/or postoperative functional outcome data were not available. Each patient was independently evaluated by the operating surgeon, who obtained history, physical, and imaging data in his or her own clinical practice, and surgical decision making was made with the patient without a predetermined algorithm or randomization to guide treatment for the study. Data were collected in a prospective fashion by individual surgeons and later compiled into a unified data collection set for statistical analysis. Institutional review board approval was obtained before the study began.
Clinical Assessment
Baseline characteristics recorded via questionnaire included sex, age, hand dominance, arm involved, and level of activity (none, recreational, overhead, contact, overhead and contact). Preoperative external rotation (ER) at the side, forward flexion, and internal rotation (IR) to the nearest estimated spinal level (T1 = 1, T12 = 12, L1 = 13, L5 = 17, etc.) were measured by the treating surgeon at each site as part of the routine clinical examination. Patient-reported outcome measures (PROs) included a visual analog scale (VAS) for pain, the Western Ontario Shoulder Instability Index (WOSI), and the Single Assessment Numeric Evaluation (SANE). Functional outcomes and range of motion (ROM) were reassessed at 2-year follow-up. Final follow-up information also included return to the same level of sport, patient satisfaction, and rates of recurrent instability and complications.
Bone Loss Assessment
Bone loss assessment included glenoid width and estimated GBL, Hill-Sachs lesion depth, Hill-Sachs interval (width), and subsequent calculation of on-track or off-track lesions as previously described. 5,10,16,21,36 Assessment was performed by the treating surgeon as previously described, but computed tomography was the imaging modality used rather than magnetic resonance imaging. 16,37 GBL measurements were specifically performed using 3-dimensional reconstructions and the method described by Giles et al 21 (male: 2/3 glenoid height + 5 cm; female: 2/3 glenoid height + 3 cm). The surgeons used their own clinical imaging software, and this was not standardized during the study.
Surgical Technique
Surgeries were performed by 4 surgeons at 4 different institutions (A.L., J.B., P.J.D., P.N.). Treatment choice was based on surgeon preference and clinical discussion. The 4 treating surgeons operated in 3 different continents but had completed the same arthroscopic shoulder fellowship, representing a similarity in surgical techniques.
REMP was performed by 2 of the 4 surgeons (P.N., P.J.D.). The technique included 3 or 4 anchors for the Bankart repair and 2 anchors for the remplissage. A mixture of knotted, knotless, and hybrid techniques was used. During remplissage, care was taken to pass sutures through the tendon and capsule only to avoid muscular damage to the posterior rotator cuff. 28 Postoperatively, the shoulder was placed in a sling for 6 weeks. The sling was then discontinued, and ROM and strengthening activities were commenced. Sports, contact or noncontact, were initiated at 6 months after surgery.
Open Latarjet was performed by 3 of the 4 surgeons (J.B., A.L., P.N.). The patients were placed in the beach-chair position with a deltopectoral approach and subscapularis split. The coracoid was then transferred to the anterior glenoid, with the inferior surface flush to the glenoid, and secured with 2 screws. 9,32 Before closure, the coracoacromial remnant was sutured to the capsule in an extra-articular fashion while the arm was held in 90° of abduction and 90° of ER. The patients’ postoperative rehabilitation and return to sport differed from REMP. The patients were placed in a sling for 2 weeks. Plain films were reviewed at 2 weeks, 6 weeks, and 3 months. The sling was discontinued, and ROM and strengthening activities were initiated. Noncontact sports were commenced at 6 weeks, and contact sports began at 3 months if plain films remained stable and symptoms allowed.
Statistical Analysis
To compare baseline characteristics and outcomes between the REMP and Latarjet cohorts, we used Pearson chi-square tests for categorical variables and independent-samples t tests for continuous variables. Paired t tests were performed to compare absolute preoperative and postoperative ROM and PRO scores within groups as well as relative improvement over time. SPSS software (IBM, version 28) was used for calculations. Continuous variables were presented as means and standard deviations, and categorical variables were reported with frequencies and percentages. Statistical tests were 2-sided, with P < .05 denoting statistical significance.
A post hoc power analysis showed that our study sample provided only adequate power (80%) to find large effect size differences (0.8) in outcome scores between groups.
Results
Patient Characteristics
A total of 47 patients met inclusion criteria and were available for follow-up at a mean of 2.3 years postoperatively (range, 2-4.5 years). The cohort included 25 patients who underwent REMP and 22 who underwent Latarjet. Patient satisfaction at 2-year follow-up was not available for 1 Latarjet patient. Baseline characteristics were similar for age, sex, athletic participation, and preoperative function. Mean preoperative GBL, Hill-Sachs width, and off-track lesions (59.1% vs 44.0% for REMP vs Latarjet, respectively; P = .302) also showed similarity, whereas Hill-Sachs depth was increased in the REMP cohort compared with Latarjet patients (9.3 ± 3.9 mm vs 5.6 ± 4.4 mm, respectively; P = .005) (Table 1). REMP patients had greater preoperative IR compared with Latarjet patients (T8 ± 2 vs T10 ± 2, respectively; P = .008).
Surgeon Performance per Procedure a

a REMP, arthroscopic Bankart repair with remplissage.
Patient-Reported Outcomes
Minimum 2-year postoperative PROs were similarly improved in both cohorts (Table 2). SANE, VAS, and WOSI had postoperative improvements that were statistically significant for both interventions, although the magnitude of difference in improvement between the procedures was not significant. The 2 cohorts experienced similar improvements in forward flexion and IR. REMP patients experienced a decrease in ER whereas the Latarjet group experienced an increase (–4° ± 13° vs +10° ± 22°, respectively; P = .017) (Table 3).
Characteristics of the Study Population a
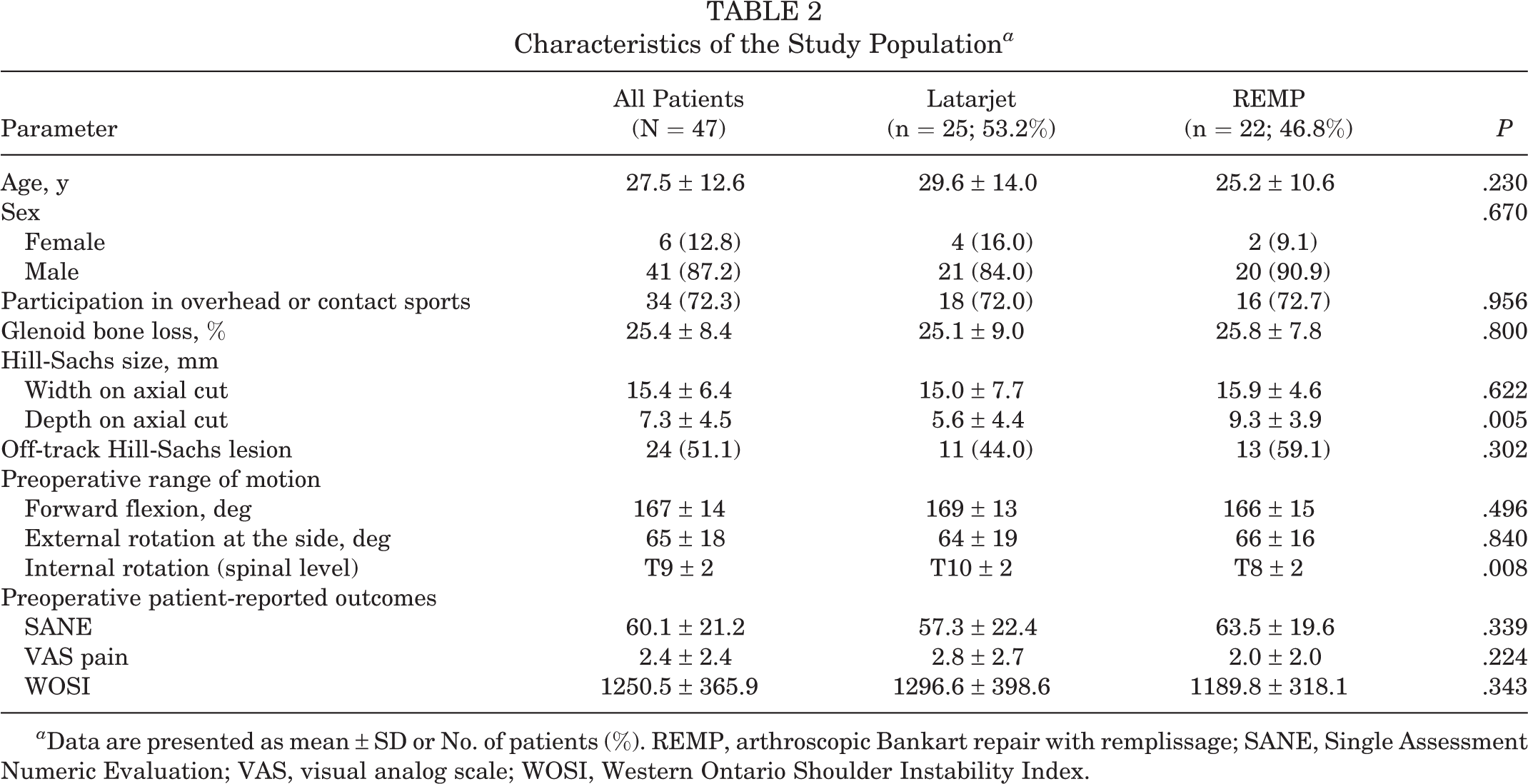
a Data are presented as mean ± SD or No. of patients (%). REMP, arthroscopic Bankart repair with remplissage; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
Minimum 2-Year Postoperative Patient-Reported Outcomes and Range of Motion a

a Outcomes are reported as mean ± SD. Boldface P values indicate statistically significant difference (P < .05). ER, external rotation; FF, forward flexion; IR, internal rotation; REMP, arthroscopic Bankart repair with remplissage; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
Return to Sport, Satisfaction, Recurrence, and Revision
Return to the same level of sport (87.5% vs 86.4%; P = .99) and satisfaction (95.8% vs 95.5%; P = .99) were similar between the groups (Table 4). One Latarjet patient’s data were incomplete for return to sport, and attempts to contact this patient were unsuccessful. No recurrent dislocations occurred during follow-up for either intervention. There was 1 complication (4.5%) in the Latarjet group consisting of a postoperative infected hematoma, which required debridement. This is notably lower than previously reported Latarjet complication rates, especially when considering hardware and bony healing. 24 There were no complications in the REMP group.
Postoperative Outcomes a

a Data were available for 46 patients. NA, not applicable; REMP, arthroscopic Bankart repair with remplissage.
Discussion
The primary finding of this study was that functional outcomes were equivalent for primary REMP and Latarjet at short-term follow-up in patients with >15% GBL. Recurrence and return to sport were also equivalent between groups. This adds to the growing body of evidence that REMP is safe and effective, and its use can be considered in patients with >15% GBL.
Advancements in instability surgery, including advocating for treatment based on GBL combined with categorization of the glenoid track, have greatly benefited patient care. 10,16,41 As the definition of critical bone loss has gradually lowered, it has become abundantly clear that isolated arthroscopic Bankart repair is insufficient. 7,30,33,38 However, great debate over appropriate treatment continues, because the glenoid track concept provides an imperfect algorithm for patient care and the definition of critical bone loss is unresolved. Two common options beyond isolated arthroscopic Bankart repair include the addition of remplissage or transition to Latarjet. Those who favor remplissage often cite the invasiveness and complications of the Latarjet procedure. 23 Latarjet advocates often tout the triple effect of increased bony surface, sling effect of the conjoined tendon, and reconstruction of the inferior capsuloligamentous structure with repair to the coracoacromial ligament. 6,14,29 The Latarjet procedure also results in earlier return to sport, 1 and Latarjet advocates note that REMP may work by creating stiffness in the joint that may have long-term consequences. 3,15,18,25,35
Our study affirms similar PROs and return to sport for REMP and Latarjet, whereas ROM results are mixed in the literature. 2,4,12,34 A concern regarding REMP is the possibility of decreased ER based on biomechanical studies. 3,15,18,35 We noted a 4° ER decrease in the REMP patients compared with a 10° increase in the Latarjet patients after the procedure (–4° ± 13° vs +10° ± 22°, respectively; P = .017), which coincides with findings by Bah et al 4 (45° vs 56°; P < .001). In contrast, Cho et al 13 and Yang et al 41 noted no difference in ER between procedures. Although results are mixed, the possible loss of ER should be heavily considered in overhead athletes, particularly overhead throwers. However, it should be noted that our increased ER for the Latarjet is unusual when compared with the biomechanical and clinical studies noted. This is likely due to differences in surgeons’ measurements but could also be due to our extracapsular repair of the coracoacromial ligament with the arm held at 90° of abduction and ER, which allows for stable repair without sacrificing ROM. 32
It is well-established that both REMP and Latarjet decrease dislocation rates. 22,24,36 In a systematic review of 194 REMP and 185 Latarjet procedures, the rates of recurrent instability were 9.8% and 7.0%, respectively (P = .0004), for patients with engaging lesions and subcritical bone loss. 24 Another systematic review evaluated REMP versus bone block augmentation procedures (ie, Latarjet) and noted similar dislocation risks for patients with <10% GBL (0%-13.3% vs 5.7%-11.6% for REMP vs Latarjet, respectively) with mean 41-month follow-up. 22 However, the investigators recommended against soft tissue–only intervention for patients with 10% to 15% GBL due to increased dislocation with REMP (6.1%-13.2% vs 0%-8.2%, respectively). In contrast, the current study provides evidence that remplissage may be effective for some patients with >15% GBL. We observed no recurrences in either group despite a similar amount of preoperative participation in overhead or contact sports and high amount of preoperative GBL (25.8% vs 25.1%, respectively; P = .800) and off-track lesions (59.1% vs 44.0%, respectively; P = .302). We do not intend to imply that REMP should or can replace Latarjet but rather to suggest the REMP may still be an option for some patients with >15% GBL. In the literature, the complication rate of Latarjet is higher than that of REMP, and the complications in our study were particularly low. For instance, Haroun et al 24 noted a substantially increased rate of complications after Latarjet (9%) compared with REMP (1%) (P = .003) in their systematic review. Given the diversity of surgeons and patients, in an effort to minimize complications, it may be reasonable to consider REMP in patients with >15% GBL. However, more long-term, prospective evaluations are needed to compare REMP and Latarjet more thoroughly in this setting.
Limitations
This multicenter study was not without limitations. Our study design was retrospective, and the cohort size was small, even with 4 high-volume surgeons. We had no data on patients lost to follow-up. Treatment choice was based on surgeon preference rather than a predetermined algorithm or randomization. Although patient characteristics appeared to be similar between groups at baseline, there was likely a selection bias for procedure type based on patient presentation and surgeon preferences. There were also likely subtle differences between the nonblinded surgeon clinical assessments, documentation, and instrumentation used for surgery. The sample was small, and surgeons could have had significantly different results and complications if a larger sample had been available. The follow-up was short term at 2 years postoperative without long-term assessments or radiographs. It has been demonstrated that recurrence after glenohumeral stabilization increases with longer term follow-up. 8 Finally, a cost comparison was not practical based on the use of 4 international sites, and therefore, we could not assess the value of each procedure.
Conclusion
At short-term follow-up, the hypothesis was upheld: REMP and Latarjet provided similar outcomes for patients with >15% GBL, although REMP patients experienced slightly decreased ER. Although larger series and longer term follow-ups are required, remplissage may be considered as a treatment option in patients with >15% GBL.
Footnotes
Final revision submitted August 29, 2022; accepted September 15, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.L. received funds for supplies from the FORE foundation. J.L.H. has received education payments from Pylant Medical and hospitality payments from Encore Medical. P.N. has received support from Arthrex, outside of the submitted work. A.L. has received consulting fees from Arthrex, Medacta, and Stryker and royalties from Stryker; he has stock/stock options in Medacta. He is the founder of FORE, Med4Cast, and BeeMed. J.B. has received consulting fees from Arthrex, Move Up, and SBM and royalties from SBM and Move Up. P.J.D. has received education payments from Steelhead Surgical, consulting fees from Arthrex and Pacira Pharmaceuticals, and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Salus IRB.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.