
Abstract
Background:
Involvement of the intramuscular (central) tendon in acute hamstring injuries, as detected on magnetic resonance imaging (MRI), may prolong recovery times. To date, it is unclear whether hamstring injuries exhibiting intramuscular tendon involvement can be identified though routine clinical examinations that assess flexibility and strength.
Purpose:
To test whether MRI-detected intramuscular tendon involvement could be identified by a clinical assessment of muscle strength and flexibility.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Participants were drawn from a multicenter randomized controlled trial on the effect of platelet-rich plasma in acute hamstring injuries. Clinical parameters assessed within 5 days of injury were active knee extension and passive straight-leg raise for hamstring flexibility and isometric knee flexion force with 15° and 90° of knee flexion. Also, 1.5-T MRI of the thigh was performed within 5 days of injury and was evaluated for the presence of different types of intramuscular tendon involvement. One-way analysis of variance was used to determine whether clinical parameters could discriminate injuries with intramuscular tendon involvement from those without such involvement.
Results:
A total of 74 acute hamstring injuries were included, with 52 (70.3%) injuries affecting the myotendinous junction. Injuries exhibiting intramuscular tendon discontinuity on MRI had an increased mean absolute flexibility deficit for active knee extension (20.4° ± 14.9° vs 10.7° ± 9.0°, respectively; P = .006) and decreased mean strength at 15° (62.2 ± 26.7 N vs 76.6 ± 22.5 N, respectively; P = .05) compared with injuries without intramuscular tendon discontinuity. Flexibility and strength showed major overlap and variance among injuries with and without intramuscular tendon involvement.
Conclusion:
Hamstring flexibility and strength cannot be used to discriminate the presence of intramuscular tendon involvement.
Muscle injuries can lead to a substantial absence from training and competition and can limit optimal performance. Of all noncontact muscle injuries, the hamstring muscles are the most commonly affected. 1,5,6,9,12,13,15,16,34 Many previous studies of acute hamstring injuries have attempted to demonstrate imaging features that might be clinically relevant, especially those depicted on magnetic resonance imaging (MRI). †† Several discrepancies have been found when evaluating the relevance of different MRI features, especially when testing these features against the amount of time needed before return to play 8,24,28,35 and the incidence of reinjuries. 17,20,27,36
Two recent studies demonstrated that the presence of MRI-detected intramuscular tendon discontinuity (at the myotendinous junction [MTJ]) in acute hamstring injuries is related to much longer recovery times than injuries without such involvement. 7,26 Furthermore, 1 of these studies demonstrated an increased risk for hamstring reinjuries when extensive initial involvement of the intramuscular tendon was present. 26 These results suggest a potential for intramuscular tendon involvement as a prognostic feature in acute hamstring injuries. To date, it is unclear if hamstring injuries exhibiting intramuscular tendon involvement can be identified through routine clinical examinations that assess flexibility and strength. If intramuscular tendon involvement appears to affect recovery times in athletes, it may be that it impairs muscle function at the time of injury compared to injuries without tendon involvement.
To test the hypothesis that a clinical assessment of flexibility and strength can identify hamstring injuries exhibiting intramuscular tendon involvement, we examined the relationships of hamstring flexibility and strength with different types of MRI-detected intramuscular tendon involvement.
Methods
Participants
Participants included in our study were enrolled in a randomized controlled trial of platelet-rich plasma injections in acute hamstring muscle injuries: the Dutch Hamstring Injection Therapy (HIT) study. Detailed information on the main study design, recruitment, inclusion and exclusion criteria, randomization, sample size calculation, blinding, and intervention has been previously published (supplemented online at http://www.nejm.org/doi/suppl/10.1056/NEJMc1402340/suppl_file/nejmc1402340_appendix.pdf). 30 Briefly, participants were included if they were between 18 and 50 years of age and had sustained an acute hamstring injury, with positive findings on MRI at baseline. Participants with a clinical diagnosis of an acute hamstring injury without abnormal MRI findings or with complete muscle ruptures/tendon avulsions (grade 3 injuries) were not included. 31 For the present cross-sectional substudy, only the baseline assessments (ie, before treatment) were considered for the analysis.
Clinical Examinations
Hamstring Flexibility
Flexibility was evaluated at baseline using 2 tests: the active knee extension 22,32 and the passive straight-leg raise. 2 Participants were evaluated supine with an inclinometer placed at the anterior tibial aspect. For the active knee extension test, participants placed the hip of the tested leg in 90° of flexion and were instructed to extend the knee until maximal tolerable stretch, with the contralateral leg remaining flat on the table. At the endpoint of maximal tolerable stretch, the absolute knee angle was measured. For the passive straight-leg raise test, participants were instructed to fully relax the tested leg, while the examiner lifted the leg with the knee in full extension until maximal tolerable stretch was reached. The contralateral leg remained completely flat on the table. At maximal tolerable stretch, the angle between the raised leg and the table was calculated. For both flexibility tests, both (injured and uninjured) legs were assessed, and the absolute flexibility deficit was calculated by subtracting the angle of the injured leg from that of the uninjured leg. The higher the resultant angles, the higher the absolute flexibility deficit. The reported minimal detectable difference in the study cohort of the active knee extension test was 15° and for the passive straight-leg raise test was 21°. 32
Isometric Knee Flexion Force
Participants were evaluated in a prone position with the knee in 15° and 90° of flexion, with flexion force assessed using handheld dynamometry. 21 The dynamometer was placed on the participant’s heel, applying force to the heel, which was gradually increased over 3 to 5 seconds. Participants were instructed to resist the force applied by the examiner, and at the exact point that participants could no longer resist, the assessment was terminated and the reading taken. Force was measured in newtons (N). Both legs (injured and uninjured) were evaluated 3 times with the knee flexed at 15° and 90°, and only the highest force values were recorded. The relative strength deficit (%) was calculated by dividing the recorded maximal force value of the injured leg by the maximal force value of the uninjured leg. The reported minimal detectable difference for strength at 15° and 90° was 81 N and 71 N, respectively. 29
The clinical testers were blinded to the results of the MRI assessments.
MRI Protocol
MRI of the injured leg was performed at baseline within 5 days of injury. A modified version of the protocol described by Askling et al 3 was applied. To locate the area of the injury, the entire hamstring muscle complex of the injured limb was assessed by obtaining coronal and sagittal short tau inversion recovery (STIR) scans from the ischial origin of the hamstring muscles to their distal insertion on the fibula and the tibia (repetition time/echo time [TR/TE] of 3500/31 ms, inversion time [TI] of 170 ms, field of view [FOV] of 300 mm, and a 256 × 320 matrix). Subsequently, axial STIR (TR/TE of 3500/31 ms, TI of 170 ms, FOV of 300 mm, and a 205 × 256 matrix), T1-weighted (TR/TE of 500/12 ms, FOV of 300 mm, and a 355 × 448 matrix), and T2-weighted (TR/TE of 4080/128 ms, FOV of 300 mm, and a 355 × 448 matrix) scans were obtained from the injured area. The slice thickness for all sequences was 5 mm. MRI was performed with a 1.5-T magnet system (Magnetom Essenza; Siemens) with the use of a surface coil.
MRI Interpretation
Each MRI scan was initially assessed by a single experienced musculoskeletal radiologist (M.M.), blinded to clinical data, using standardized scoring forms with known excellent reliability. 3,8,14,18,19,35 Injuries were graded from 1 to 3 according to the classification of Hancock et al 19 : grade 1: increased muscle signal intensity on fluid-sensitive sequences without evidence of a macroscopic tear; grade 2: increased muscle signal intensity on fluid-sensitive sequences with a visible partial tear; and grade 3: total muscle or free proximal or distal tendon rupture.
A second experienced musculoskeletal radiologist (M.D.C.), blinded to clinical data and to the initial MRI assessment for grading injuries, independently examined hamstring injuries depicted on MRI using another grading system for intramuscular tendon involvement (at the MTJ). For each muscle evaluated in this cohort, injuries were considered to affect the MTJ when the abnormalities (increased signal intensity or rupture) were centered at the MTJ. Injuries affecting the MTJ were then scored as different types using the fluid-sensitive sequences (STIR and T2) on MRI (Figure 1): no injury: no morphological or signal changes around the MTJ; type 1: increased signal intensity with a feathery pattern around the MTJ, with the intramuscular tendon exhibiting normal morphology and signal; type 2: increased signal intensity with a feathery pattern around the MTJ, with the intramuscular tendon exhibiting thickening and/or abnormal increased signal without discontinuity of the tendon; type 3: increased signal intensity with a feathery pattern around the MTJ, with the intramuscular tendon exhibiting partial-thickness discontinuity/disruption; and type 4: increased signal intensity with a feathery pattern around the MTJ, with the intramuscular tendon exhibiting complete disruption. When more than 1 muscle was involved, only the muscle exhibiting the most extensive MRI findings was included in the analysis. Because it may affect the assessment of hamstring strength and flexibility, the presence of chronic changes at the MTJ depicted on MRI (abnormal low signal intensity depicted in all sequences with architectural distortion near the MTJ) or proximal or distal free tendon injuries was also recorded.

Coronal short tau inversion recovery (STIR) scans showing magnetic resonance imaging (MRI) grades of myotendinous junction (MTJ) and intramuscular tendon involvement in acute injuries of the long head of the biceps femoris muscle. (A) Type 1: increased signal intensity with a feathery pattern around the MTJ, with the adjacent tendon exhibiting normal morphology and signal (arrows). (B) Type 2: increased signal intensity with a feathery pattern around the MTJ, with the adjacent tendon exhibiting mild thickening and abnormal increased signal without discontinuity of the tendon (arrows). (C) Type 3: increased signal intensity with a feathery pattern around the MTJ, with the adjacent tendon exhibiting abnormal signal intensity and partial discontinuity/disruption and a waviness pattern of the tendon (arrows). (D) Type 4: increased signal intensity with a feathery pattern around the MTJ, with the adjacent tendon exhibiting complete disruption (arrow). Consecutive axial STIR and T2 scans were systematically evaluated to confirm the absence or presence of intramuscular tendon discontinuity.
Statistical Analysis
Initially, descriptive analysis was performed to show the frequencies of muscles affected and the frequency and distribution of MTJ injury grades in hamstring muscles. To test for differences in hamstring strength and flexibility deficits between the different types of MTJ/intramuscular tendon involvement assessed on MRI, we applied 1-way analysis of variance (ANOVA). We also applied ANOVA to test for differences in hamstring strength and flexibility deficits between injuries exhibiting intramuscular tendon discontinuity (types 3 and 4) versus those without intramuscular tendon discontinuity (types 1 and 2). As the injury severity assessed according to the classification of Hancock et al 19 demonstrated no significant relationship with hamstring flexibility and strength, these grades were not taken into account for the analysis. Statistical significance was set at .05. All analyses were performed using SPSS Statistics version 23.0 (IBM).
Results
The baseline characteristics of the 80 participants included in the Dutch HIT study have been previously published (http://www.nejm.org/doi/suppl/10.1056/NEJMc1402340/suppl_file/nejmc1402340_appendix.pdf). 30 For our cross-sectional substudy, 5 participants were excluded because of the presence of chronic changes at the MTJ depicted on MRI, and 1 participant was excluded because of the presence of proximal free tendon partial avulsions. Ultimately, 74 participants with acute hamstring injuries detected on MRI at baseline were included in the analysis, with 64 (84.2%) injuries affecting the long head of the biceps femoris muscle, 2 (2.7%) affecting the short head of the biceps femoris muscle, 2 (2.7%) affecting the semitendinosus muscle, and 6 (8.1%) affecting the semimembranosus muscle. Furthermore, a total of 52 (70.3%) injuries exhibited involvement of the MTJ on the baseline MRI assessment (12 type 1 injuries, 15 type 2, 22 type 3, and 3 type 4). The baseline characteristics of the 74 participants included in the present study are displayed in Table 1.
Baseline Characteristics of the Included 74 Participants a

a Values are expressed as mean ± SD unless otherwise specified. ACL, anterior cruciate ligament; IQR, interquartile range; MRI, magnetic resonance imaging.
Table 2 shows the differences in hamstring flexibility (active knee extension test and passive straight-leg raise test) and strength (isometric knee flexion force at 15° and 90°) with regard to the MRI grades of MTJ involvement. When considering each MRI injury type for MTJ/tendon involvement separately, we noted that an increase in MRI type was related to a decrease in mean hamstring flexibility as assessed by the active knee extension test (a higher difference in angles between the injured vs uninjured legs referring to lower flexibility): type 1, 8.1° ± 8.9°; type 2, 12.8° ± 8.8°; type 3, 19.6° ± 13.7°; and type 4, 26.0° ± 25.6° (P = .030). The wide SD values obtained for each MRI injury grade indicate overlap (Figure 2). No differences in flexibility determined by the passive straight-leg raise test were found when considering each MRI type separately. Furthermore, there were no differences in strength when considering each MRI type separately.
Myotendinous Junction Grade on MRI a
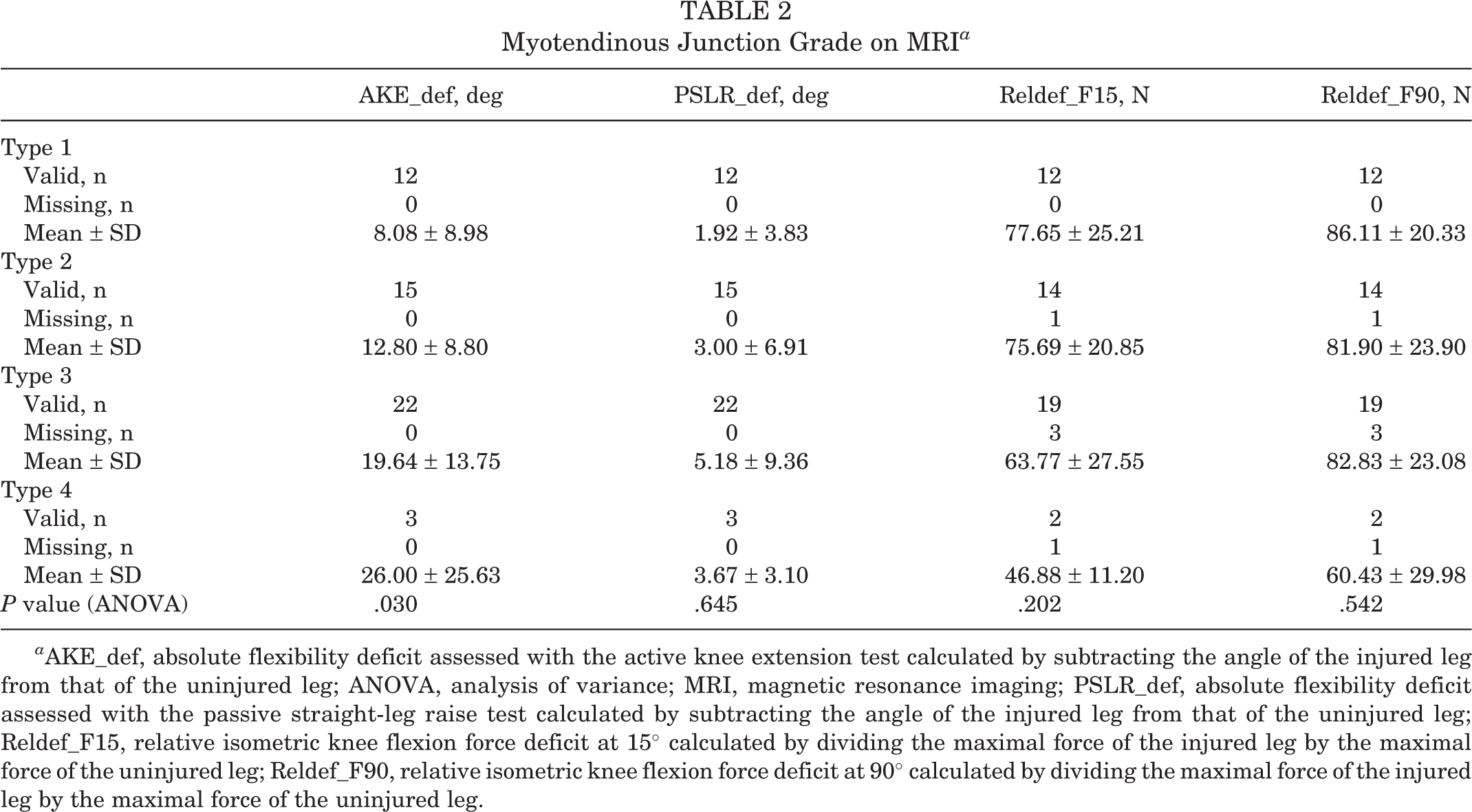
a AKE_def, absolute flexibility deficit assessed with the active knee extension test calculated by subtracting the angle of the injured leg from that of the uninjured leg; ANOVA, analysis of variance; MRI, magnetic resonance imaging; PSLR_def, absolute flexibility deficit assessed with the passive straight-leg raise test calculated by subtracting the angle of the injured leg from that of the uninjured leg; Reldef_F15, relative isometric knee flexion force deficit at 15° calculated by dividing the maximal force of the injured leg by the maximal force of the uninjured leg; Reldef_F90, relative isometric knee flexion force deficit at 90° calculated by dividing the maximal force of the injured leg by the maximal force of the uninjured leg.
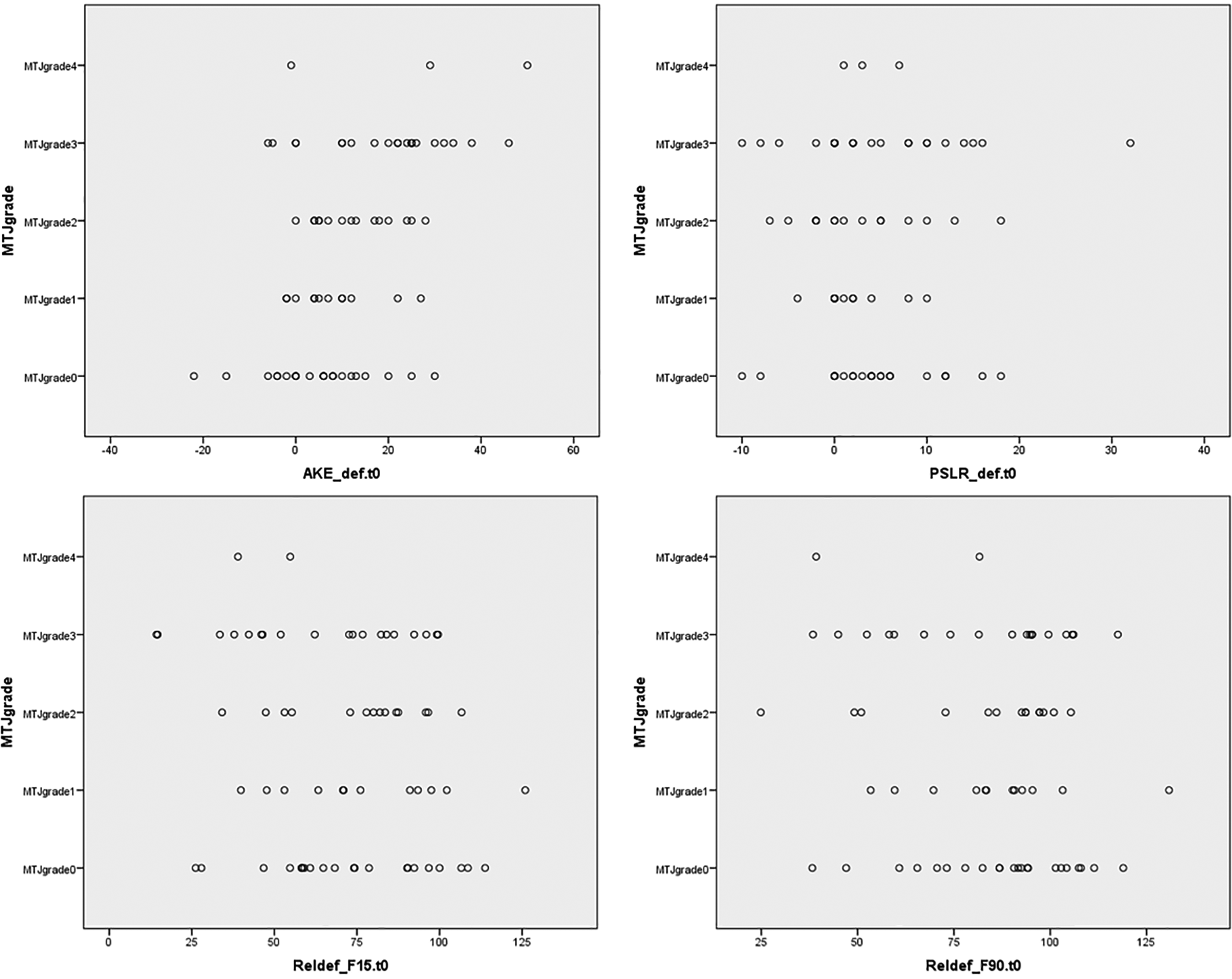
Scatter plots from Table 2. AKE, active knee extension test; MTJ, myotendinous junction; PSLR, passive straight-leg test; Reldef_F15, strength at 15°; Reldef_F90, strength at 90°.
Table 3 depicts the differences in hamstring flexibility (active knee extension test and passive straight-leg raise test) and strength (isometric knee flexion force at 15° and 90°) with regard to the presence of tendon discontinuity (vs no discontinuity) as depicted on MRI. Injuries exhibiting partial or complete intramuscular tendon discontinuity on MRI (types 3 and 4) when compared to injuries without intramuscular tendon discontinuity (types 1 and 2) showed an increased mean absolute flexibility deficit for the active knee extension test (20.4° ± 14.9° vs 10.7° ± 9.0°, respectively; P = .006) and decreased mean strength at 15° (62.2 ± 26.7 N vs 76.6 ± 22.5 N, respectively; P = .051). Here again, the wide SD values obtained for each group (discontinuity vs no discontinuity) indicate overlap (Figure 3). When comparing injuries with discontinuity of the intramuscular tendon against those without discontinuity, no differences were found in flexibility as determined by the passive knee extension test or in strength (isometric knee flexion force at 90°).
Tendon Discontinuity at the Myotendinous Junction a

a Injuries exhibiting discontinuity of the tendon (types 3 and 4) were compared to injuries without tendon discontinuity (types 1 and 2). AKE_def, absolute flexibility deficit assessed with the active knee extension test calculated by subtracting the angle of the injured leg from that of the uninjured leg; ANOVA, analysis of variance; PSLR_def, absolute flexibility deficit assessed with the passive straight-leg raise test calculated by subtracting the angle of the injured leg from that of the uninjured leg; Reldef_F15, relative isometric knee flexion force deficit at 15° calculated by dividing the maximal force of the injured leg by the maximal force of the uninjured leg; Reldef_F90, relative isometric knee flexion force deficit at 90° calculated by dividing the maximal force of the injured leg by the maximal force of the uninjured leg.

Scatter plots from Table 3. AKE, active knee extension test; PSLR, passive straight-leg test; Reldef_F15, strength at 15°; Reldef_F90, strength at 90°.
Discussion
Our study demonstrated a relationship between types of intramuscular tendon involvement detected on MRI and flexibility as assessed by the active knee extension test, with the more severe MRI types related to increased mean deficits in hamstring flexibility. Furthermore, we demonstrated that acute hamstring injuries exhibiting discontinuity of the intramuscular tendon had higher mean deficits in flexibility and strength when compared to injuries without intramuscular tendon discontinuity, with the differences in strength at 15° of knee flexion almost significant (P = .051). However, because of major overlap and variance observed in flexibility and strength when comparing the different MRI grades, it was not possible clinically to identify injuries exhibiting intramuscular tendon involvement.
To date, the clinical relevance of muscle injuries involving the intramuscular tendon has been little explored. The majority of previous work assessing MRI features of hamstring injuries did not take into account the presence of this characteristic. 2,3,4,8,11,14,24,33 A recent systematic review included studies that assessed multiple MRI features of muscle injuries as prognostic factors and concluded that, so far, there is no strong evidence for such a relationship. 28 Limited evidence exists for a few MRI features such as an abnormal signal intensity involving the proximal tendon or intramuscular tendon, injuries not affecting the MTJ, and complete muscle or tendon ruptures. 28 Involvement of the intramuscular tendon at the MTJ in acute hamstring injuries, as depicted on MRI, has been demonstrated to represent a potential prognostic factor. 7,26 These reports, in which the return-to-play decision maker was not blinded to the initial MRI results, demonstrated that intramuscular tendon involvement was related to longer recovery times of athletes when compared to injuries without such involvement. 7,26 One of these was recently published (after the systematic review 28 ), thus adding evidence that intramuscular tendon involvement might be clinically relevant. 26 Furthermore, it has been demonstrated that extensive intramuscular tendon involvement initially detected on MRI is related to a higher incidence of hamstring reinjuries. 26
Therefore, it may be clinically relevant to depict hamstring injuries exhibiting intramuscular tendon involvement when performing routine clinical assessments. If flexibility and strength tests performed at the time of injury could identify such involvement, it would provide prognostic information to clinicians and could help in selecting athletes for MRI assessments. Although we were able to detect statistically significant differences in mean hamstring flexibility and strength when comparing injuries with and without intramuscular tendon discontinuity, the wide overlap observed in flexibility and strength measures indicates that it is not possible, according to our results, to depict intramuscular tendon involvement in acute hamstring injuries based on these clinical parameters alone.
Flexibility and strength still represent important clinical parameters widely used in sports medicine when monitoring rehabilitation after acute muscle injuries, with deficits in these parameters demonstrated to persist up to 50 days after an acute hamstring injury. 23 Furthermore, it has been demonstrated that persistent deficits in isometric force and flexibility after return to play are independent predictors of a reinjury. 10 A previous study demonstrated that flexibility, determined by the passive straight-leg raise test but not the active knee extension test, was independently associated with recovery times after hamstring injuries. 24
Our negative results support that, to date, imaging is still necessary to depict intramuscular tendon involvement in hamstring injuries, which has been demonstrated to predict longer recovery times. 7,26 Our results may further serve to increase the attention of radiologists and clinicians when assessing acute hamstring injuries on MRI, until clinical tests demonstrate usefulness in depicting intramuscular tendon involvement. To date, most radiologists apply the widely known 3-grade system, 14,19 which does not routinely include an assessment of the intramuscular tendon. Only recently have efforts been made to incorporate intramuscular tendon involvement in grading systems for muscle injuries, such as the British athletics muscle injury classification. 25
Some limitations to our study need mentioning. Although we included clinical data at the time of injury on acute hamstring injuries in our analyses, we cannot rule out the influence of potential previous injuries on the strength and flexibility assessments. To minimize such an influence, we carefully searched for MRI features of chronic muscle injuries associated with acute findings, and 5 participants were ultimately excluded because of the presence of chronic features. Furthermore, because of the cross-sectional design of our study, we cannot affirm that injuries exhibiting intramuscular tendon involvement actually lead to a deficit in muscle strength and flexibility, although it is worth mentioning that preexisting decreased hamstring strength or flexibility, possibly from a prior injury, could lead to injuries with involvement of the tendon at the MTJ. Finally, we acknowledge the lack of a control group of patients with clinical features of a hamstring injury but negative (normal) MRI findings as a limitation of this study.
Conclusion
We demonstrated that acute hamstring injuries affecting the intramuscular tendon, as depicted on MRI, are related to decreased hamstring flexibility and strength in comparison to injuries without tendon involvement, especially when tendon discontinuity is present. However, because of the wide overlap and variance of clinical parameters when testing the different MRI grades of injuries, it was not possible clinically to affirm the presence of intramuscular tendon involvement in hamstring injuries based on flexibility or strength assessments alone.
Footnotes
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Royal Dutch Football Association and Arthrex Medizinische Instrumente.
Ethical approval for this study was obtained from Haaglanden Medisch Centrum.