
Abstract
Background:
Spontaneous osteonecrosis of the knee (SONK) is a clinical entity identified by acute knee pain usually associated with joint effusion, with radiographic findings of a radiolucent defect on the weightbearing area of the femoral condyle. Conservative treatment is initially undertaken; however, surgical procedures are often necessary. Historically, surgical options have included core decompression, cartilage repair, high tibial osteotomy, or joint arthroplasty. Few studies in the literature have reported the use of fresh osteochondral allograft (OCA) for the treatment of SONK lesions.
Hypothesis:
OCA transplantation is an effective treatment for SONK lesions on the medial femoral condyle.
Study Design:
Case series; Level of evidence, 4.
Methods:
A case series was analyzed of 7 patients treated with OCA for large SONK lesions of the medial femoral condyle with a minimum 4-year follow-up. All patients experienced failure of at least 6 months of conservative treatment and declined arthroplasty as the form of definitive treatment for medial femoral condyle lesion. All patients underwent OCA of the medial femoral condyle. Mean lesion size was 4.6 cm2 (range, 3.24-6.25 cm2), with a mean condylar width of 41.7 mm (range, 35.4-48.6 mm), resulting in a median proportion (lesion size/condylar width) of 56.8% (range, 32.7%-62.6%). The median surface allograft area was 5.1 cm2 (range, 3.2-6.3 cm2).
Results:
The median follow-up was 7.1 years (range, 4.5-14.1 years). No patient had additional surgery following OCA transplant; the allograft failure rate was 0%. Subjective outcome scores from the International Knee Documentation Committee, Knee injury and Osteoarthritis Outcome Score, and modified Merle d’Aubigné-Postel scale improved from preoperative assessment to the latest follow-up. All patients were extremely satisfied with the results of the OCA transplant.
Conclusion:
Fresh OCA transplantation demonstrated excellent efficacy, durability, and satisfaction in this group of patients with isolated stage 2 and 3 SONK lesions who had experienced failure of conservative treatment. Fresh osteochondral allografts are an attractive method for surgical management of selected patients with spontaneous osteonecrosis of the knee.
Spontaneous osteonecrosis of the knee (SONK), originally described by Ahlbach et al 2 in 1968, was thought to represent a manifestation of focal osteonecrosis of the femoral condyle that may progress to severe osteoarthritis of the medial femorotibial joint. On plain radiographs, SONK initially appears as a flattening of the femoral condyle and progresses to a radiolucent osteochondral defect adjacent to the weightbearing area, typically involving the medial femoral condyle. 8,28 On magnetic resonance imaging (MRI), SONK lesions appear as a focal, low-signal finding with linear features in the subarticular bone of the epiphysis. 28 The exact cause of SONK remains unknown. Theories of a disrupted vascular supply, repetitive trauma, and postarthroscopic origin have been suggested, although some authors have assumed that this typical lesion could result from an insufficiency fracture of the subchondral bone. 1,6,26,37 Clinical findings of SONK are characterized by a sudden acute severe pain in the knee usually associated with articular effusion, with most patients presenting in their 50s or older. SONK can be differentiated from secondary osteonecrosis by the absence of risk factors such as alcoholism, chronic use of corticosteroids, and systemic disorders. 18,19,28
Conservative treatment with protected weightbearing, analgesics, and physical therapy is usually successful in early stages, with resolution of MRI alterations and clinical symptoms in up to 93% of patients. 20,38 In more advanced stages of the disease, patients with larger lesions and osteochondral defects comprising more than 40% of the condylar width have an unfavorable prognosis and tend to rapidly progress to osteoarthritis. 1 Surgical treatment is usually performed after failure of conservative treatment or in poor prognostic lesions and includes core decompression, cartilage repair, high tibial osteotomy, or joint arthroplasty. 1,10,35,39 A typical SONK lesion can be characterized as an isolated osteochondral defect in the femoral condyle and may be considered appropriate for biological joint preservation procedures that include replacement of the diseased osteochondral unit. The use of osteochondral autologous transplantation (OAT) for SONK has been reported. 10,13 This technique is best suited for small osteochondral defects of 1 to 2 cm2, where a single plug is necessary due to donor site morbidity and technical challenges involved in multiple graft insertion. 17
Fresh osteochondral allograft (OCA) transplantation has traditionally been used for primary repair of large osteochondral lesions of the knee or as a salvage procedure when other repair techniques have failed. 7 In our previous series we presented good results with OCA as a salvage procedure for secondary osteonecrosis of the knee 16 ; however, few studies have reported the use of OCA for the treatment of SONK lesions.
The purpose of this study was to determine whether joint preservation surgery in the form of fresh OCA transplant is an effective treatment for SONK lesions on the medial femoral condyle; we undertook this by assessing allograft survivorship and subjective outcomes of pain, function, quality of life, and satisfaction among a case series of patients.
Methods
Patient Selection
Using our institutional review board–approved OCA database, we identified 7 patients who had been treated with OCA transplant for large SONK lesions of the medial femoral condyle between 2002 and 2011. Diagnosis of SONK was established according to Mont et al, 28 with a flattening of the femoral condyle of the knee that progressed to a radiolucent osteochondral defect adjacent to the weightbearing area and/or MRI finding of a focal, low-signal finding with linear features in the subarticular bone of the epiphysis. All patients were treated with 1 single allograft. Patients with osteochondral lesions of the patella, trochlea, lateral femoral condyle, or tibial plateau and any history of corticosteroid use, immunosuppressive therapy, or systemic diseases were excluded. The 7 consecutive patients included in the study had a diagnosis of SONK (stage 2 or 3 according to Koshino et al 23 ) (Table 1) and an axial mechanical limb alignment of less than 3° of varus. All patients experienced failure with at least 6 months of conservative treatment and declined arthroplasty as the form of definitive treatment for their medial femoral condyle lesions. Patient characteristics and allograft details were recorded (Table 2). Five of the 7 patients were male, and all patients were younger than 60 years (mean, 51.2 years; range, 43-59 years). The mean body mass index was 26.1 (range, 21.2-28.9).
Koshino Radiographic Classification for Spontaneous Osteonecrosis of the Knee (SONK) a

a From Koshino et al. 23
Patient Characteristics a
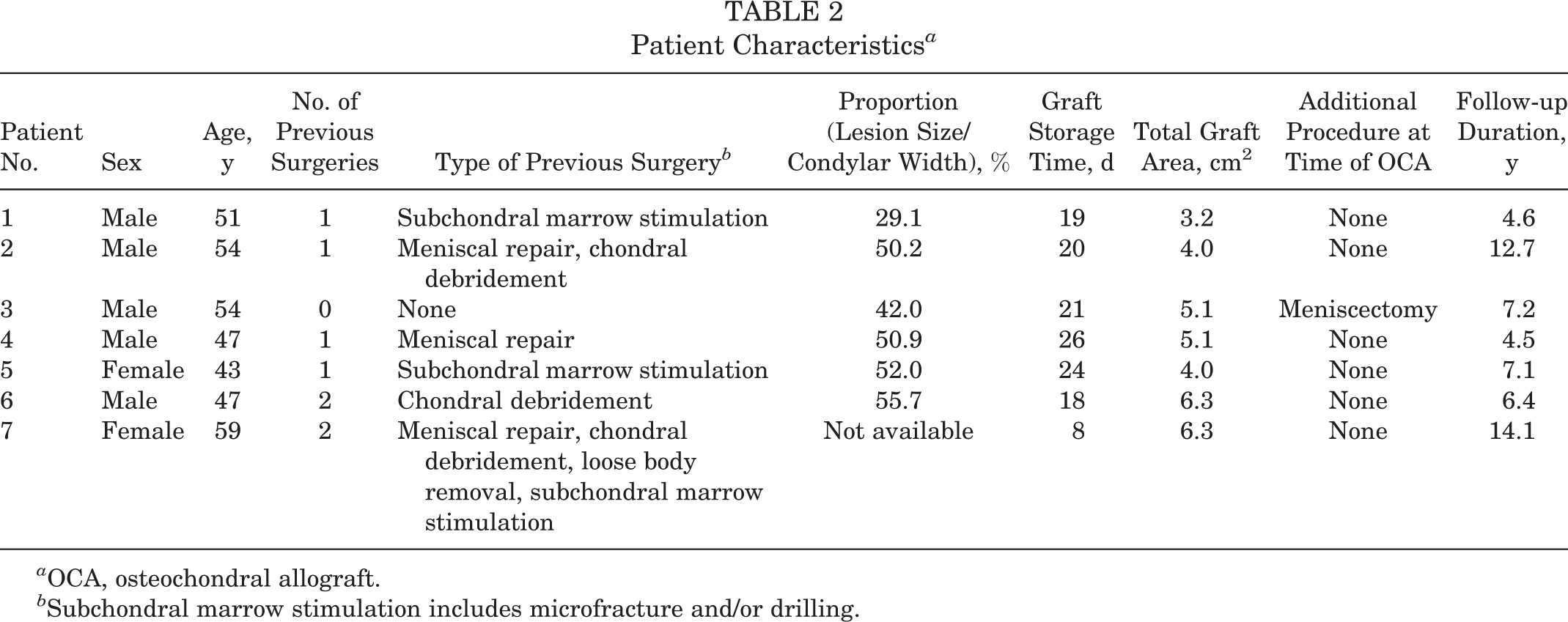
a OCA, osteochondral allograft.
b Subchondral marrow stimulation includes microfracture and/or drilling.
Radiographic Measurement
Weightbearing anteroposterior digital radiographs of both knees were taken preoperatively and were available for measurement in 6 of 7 patients. The anteroposterior size of the necrotic area was measured, and its value was expressed as a percentage of the maximum transverse width of the affected condyle (lesion size/condylar width) as described by Lotke et al. 24 The mean lesion size was 4.6 cm2 (range, 3.24-6.25 cm2), with a mean condylar width of 41.7 mm (range, 35.4-48.6 mm), resulting in a median proportion (lesion size/condylar width) of 56.8% (range, 32.7%-62.6%). The median surface allograft area was 5.1 cm2 (range, 3.2-6.3 cm2).
Surgical Treatment and Rehabilitation
Preoperatively, the allograft donor and recipient were matched by measurement of the mediolateral proximal tibial width. For the recipient, the tibial width was measured using standard anteroposterior digital radiographs after correcting for magnification; for the donor, the tibial width was directly measured with a caliper. No immunosuppressive therapy was used. Fresh OCAs were obtained from donors aged 15 to 40 years who met the criteria of the American Association of Tissue Banks. 4 All donor tissue was recovered within 24 hours of donor death and was processed and stored fresh at 4°C in tissue culture media until the time of transplant.
The surgical procedure was performed with the patient in a supine position with a tourniquet on the proximal ipsilateral thigh. An anteromedial 5-cm arthrotomy was executed. Dowel OCA technique was used in all patients as previously described. 15 A 2.5-mm Kirschner wire was drilled in the center of the lesion, and 15- to 30-mm cylindrical templates were used to measure the appropriate size of resection. Depth of the debridement was determined when healthy bleeding subchondral bone was encountered, and the depth was usually no more than 10 mm. Donor grafts were cored out at the exact same location as the lesion on the recipient, having the same depth. Press-fit fixation was achieved in all patients, and no additional fixation was used to secure the grafts in place.
Postoperatively, full range of motion was implemented as tolerated immediately after surgery. Patients were allowed 25% weightbearing for 6 weeks after surgery. After 6 weeks, progressive weightbearing was implemented as tolerated. Patients were allowed to return to recreational and sports activities by 6 months.
Outcome Assessment
Postoperatively, patients returned for clinical and radiographic evaluation at standard follow-up intervals (6 weeks, 3 months, 6 months, 1 year, and annually thereafter). Patients who did not live locally were sent a questionnaire via mail. Further surgery was documented. Failure of the allograft was defined as revision OCA transplant or conversion to partial or total knee arthroplasty. Subjective outcomes were assessed both pre- and postoperatively using the International Knee Documentation Committee (IKDC) score; the Knee injury and Osteoarthritis Outcome Score (KOOS) symptoms, pain, activities of daily living, sports/recreation, and quality of life subscale scores; and the modified Merle d’Aubigné-Postel score. Patient satisfaction was captured at each follow-up interval with a 5-item categorical scale, with responses ranging from extremely satisfied to dissatisfied. The most recent available postoperative outcome data were analyzed for the study. Postoperative radiographs were evaluated for evidence of allograft healing, subsidence, collapse, or fragmentation.
Statistical Analysis
Means, medians, ranges, and frequencies were calculated to summarize patient characteristics (age, sex, body mass index, number of previous surgeries on the operative knee, proportion of lesion/condylar width), allograft details (size), subjective patient outcomes (IKDC, KOOS, and modified Merle d’Aubigné-Postel scores), and follow-up data (follow-up duration, patient satisfaction, and radiographic evidence of allograft healing). SPSS (v 13.0; IBM Corp) was used for all descriptive statistics.
Results
All patients had a minimum follow-up of 4 years. The median follow-up duration was 7.1 years (range, 4.5-14.1 years). No patient had further surgery on the operative knee following the OCA transplant. The allograft failure rate (revision OCA transplant or conversion to partial or total arthroplasty) was 0%. Subjective outcome scores from the IKDC, KOOS, and modified Merle d’Aubigné-Postel scale improved from preoperative assessment to latest follow-up (Table 3).
Preoperative and Latest Follow-up Subjective Outcome Scores a

a Values expressed as median (range). IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score.
All 7 patients indicated they were “extremely satisfied” with the results of the OCA transplant. In all cases, integration of grafts was seen by 6 months postoperatively, with bone trabeculae crossing the interface of the graft (Figure 1). No graft subsidence, collapse, or fragmentation was seen on postoperative radiographs.

(A) Preoperative radiograph of the left knee showing a Koshino stage 3 spontaneous osteonecrosis of the knee (SONK) lesion on the medial femoral condyle. (B) Long-term postoperative radiograph after osteochondral allograft showing integration of the graft and maintenance of joint space without progression of degenerative disease.
Discussion
Joint preservation treatments for patients with focal chondral or osteochondral lesions of the knee are becoming increasingly popular in the orthopaedic community. Numerous techniques of cartilage repair have been described. 9,14 Osteochondral lesions present a unique challenge because of the combined bone and hyaline cartilage tissue injury or deficit, requiring techniques that address both bone and cartilage deficiency. Good to excellent outcomes (reduction in pain, improvement in function, high patient satisfaction) in the treatment of large osteochondral lesions such as osteochondritis dissecans, 11,31,34 fracture, 33 and secondary osteonecrosis 16 have been reported with the use of fresh OCA transplant. OCA transplant is uniquely suited for these clinical situations by virtue of its ability to restore both osseous and chondral tissue in a precise, anatomically identical fashion. SONK represents a similar clinical entity of a typically focal osteochondral lesion of the knee. Given few reports in the current orthopaedic literature of the use of joint preservation techniques in the treatment of SONK, we sought to investigate and report our experience with the use of OCA transplant in SONK. We hypothesized that OCA would effectively treat SONK lesions that failed nonoperative treatment. In this case series of Koshino stage 2 or 3 medial femoral condyle SONK lesions, we observed significant clinical improvement, high patient satisfaction, and 100% graft survivorship at a median follow-up duration of 7.1 years.
Many studies have shown that conservative treatment is usually successful for the majority of patients with SONK diagnosis if initiated in the early stages of the disease. 20,25,28,30 However, larger lesions are more likely to deteriorate over time and require surgical intervention. 21,24 For prognostic value, 2 measurements are usually used: the size of the lesion and the ratio between the size of the lesion and the width of the femoral condyle, expressed as a percentage. Lesions smaller than 3.5 cm2 or with a ratio width smaller than 20% usually have a favorable prognosis, with resolution of symptoms and radiographic images over time. 1,21,29 Yates et al 38 used MRI to evaluate 20 patients with diagnosis of SONK at an early stage in which nonoperative treatment was established. The investigators reported complete resolution of symptoms and MRI changes after a mean 4.8 months of conservative treatment. In contrast, other authors have reported that lesions larger than 5.0 cm2 or with a ratio of lesion to femoral condyle width larger than 40% to 50% tended to progress to osteoarthritis and/or condylar deformity during the first year, and surgical procedures were usually required for persistent clinical symptoms. 1,24,29 This experience suggests that large lesions are more likely to progress to degenerative disease. In our series, the mean lesion size was 4.6 cm2 (range, 3.24-6.25 cm2), and the median ratio of lesion to femoral condyle width was 56.8% (range, 32.7%-62.6%). All patients had experienced failure with previous conservative treatment, suggesting a poor prognosis and an appropriate indication for surgical intervention.
Surgical treatments for SONK lesions include core decompression, cartilage repair, high tibial osteotomy, or joint arthroplasty. Forst et al 12 evaluated 16 patients with early diagnosis of SONK on MRI following extra-articular core decompression by drilling; they reported disappearance of pain immediately after surgery in all patients and successful healing of the lesion. The authors emphasized that flattening of the affected femoral condyle was a strong predictor for progression of disease. 12 Malalignment of the limb in association with SONK has also been shown to lead to progression of cartilage damage and osteoarthritis. 32 Presence of a varus malalignment of 5° or more in patients with SONK lesions has been shown to be a poor prognostic factor. 3 In this scenario, osteotomy for correction of varus malalignment to decrease mechanical loads and potentially decrease progression of the degenerative disease has been described. 22,35 In an effort to exclude possible confounders, we included no patients who had more than 3° of malalignment or had a high tibial osteotomy associated with OCA.
Few studies have investigated results of cartilage repair techniques as a salvage procedure for SONK. OAT is a technique in which 1 or multiple osteochondral transplants are harvested from a nonweightbearing area of the knee and then transplanted to the lesion. In the case of SONK lesions, OAT has the disadvantage of donor site morbidity. Duany et al, 10 who evaluated joint-preserving surgical treatment for SONK lesions, reported on 9 patients with stage 3 lesions treated with OAT who had successful clinical outcome at a mean follow-up of 42 months. In a report of 2 cases, von Keudell et al 36 presented good long-term results following autologous chondrocyte implantation with bone graft associated with high tibial osteotomy for SONK lesions.
Two previous studies have included patients treated with OCA transplant for SONK lesions. These studies were published in the 1980s in case series with mixed patient diagnoses and inclusion criteria. OCA was performed using older “shell” techniques for the treatment of more advanced SONK. McDermott et al 27 evaluated their first 100 cases with OCA; 11 patients in their series had SONK lesions. They reported a successful outcome in only 27% (3/11) of cases, attributing poor outcome to a prolonged period of restricted weightbearing and the advanced age of the patients. Bayne et al 5 reported treatment of Koshino stage 3 and 4 SONK with bipolar OCA in 6 knees and noted that 5 of 6 unsatisfactory results were due to graft subsidence and fragmentation.
In our study, we treated 7 patients with focal stage 2 or 3 osteochondral defect of the medial femoral condyle secondary to SONK. These patients had experienced failure with conservative treatment and had been offered joint replacement as a salvage procedure. We performed OCA transplant with a single dowel transplant as an isolated procedure prior to the onset of advanced arthritis. In this study, we observed 100% survivorship and no graft subsidence or fragmentation. One explanation for the difference in outcome compared with previous reports is that our patients had stage 2 and 3 focal medial condyle lesions. Another difference is that patients were treated with a more contemporary surgical technique that entailed dowel grafts with press-fit technique, whereas Bayne et al 5 and McDermott et al 27 used shell grafts and screw fixation. Dowel transplant is usually performed with specific surgical instruments for donor and recipient, which may facilitate matching and implantation of the grafts more precisely and provide stronger host bone support and fixation.
Prosthetic arthroplasty has been used as a treatment for SONK. However, many patients are relatively young and often have subchondral bone abnormalities that could affect implant fixation, particularly in the setting of unicompartmental knee arthroplasty (UKA). In an effort to study whether results following UKA in SONK patients were similar to results in primary osteoarthritis patients, Zhang et al 39 performed a matched-pair analysis of patients treated with UKA for SONK compared with patients treated with UKA for the diagnosis of osteoarthritis. The investigators reported no difference in postoperative results in terms of pain and knee outcome scores in both groups. In the presence of advanced stages of osteoarthritis or advanced age, total knee arthroplasty may be indicated. Aglietti et al 1 reported results with total knee arthroplasty superior to those obtained with high tibial osteotomy for the treatment of SONK lesions.
Our study has several limitations. We reported on a case series with a small number of patients and no control group. Due to the specific indication of this procedure for this uncommon condition, obtaining a large sample of patients or a matched control group is very difficult. We included only patients with stage 2 and 3 medial femoral condyle SONK lesions without malalignment of the limb, so we cannot affirm that this procedure would benefit patients other than those who met our inclusion criteria. The lack of long-term radiographic follow-up is also a weakness of the study, and degenerative radiographic changes were not evaluated. Another limitation is that SONK typically occurs in women older than 55 years, 10 and in this study the majority of patients were male and younger. This preponderance of males might be due to a selection bias in that a biological repair was specifically chosen for the younger group where an alternative such as arthroplasty was considered less optimal. Conversely, the more typical older female would more likely be offered an arthroplasty over a biological repair. We were unable to determine in our database the number of patients with SONK who were treated nonsurgically or with other forms of treatment, such as osteotomy or arthroplasty, in this study period. Biological repair is likely indicated for only a small percentage of patients with SONK. This study confirms the utility of OCA for the treatment of this condition. No patients experienced failure with the procedure, and good clinical outcome and high satisfaction were reported by all patients at a median of 7.1 years postoperatively.
Treatment of large SONK lesions with biological repair remains challenging. Although involving a small series of patients, this is the largest reported series of dowel OCA transplant for treatment of isolated stage 2 and 3 SONK lesions on the medial femoral condyle. All patients had the allograft in situ at latest follow-up and had clinically meaningful improvements in pain, function, quality of life, and satisfaction, which were similar to or better than those of patients receiving osteochondral autografts or allografts for other indications. We conclude that OCA transplantation is a valuable procedure in the treatment of some patients with spontaneous osteonecrosis of the knee.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: L.E.P.T. is a consultant for Sanofi and Arthrex. J.C.M. is a consultant for JRF Ortho. W.D.B. is a consultant for DePuy, Zimmer Biologics, Smith & Nephew, and JRF Ortho.
Ethical approval for this study was obtained from the Scripps Institutional Review Board (protocol No. IRB-13-6297).