
Abstract
Background:
The Activity Rating Scale (ARS) for disorders of the knee evaluates the level of activity by the frequency of participation in 4 separate activities with high demands on knee function, with a score ranging from 0 (none) to 16 (pivoting activities 4 times/wk).
Purpose:
To translate and cross-culturally adapt the ARS into Swedish and to assess measurement properties of the Swedish version of the ARS.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
The COSMIN guidelines were followed. Participants (N = 100 [55 women]; mean age, 27 years) who were undergoing rehabilitation for a knee injury completed the ARS twice for test-retest reliability. The Knee injury and Osteoarthritis Outcome Score (KOOS), Tegner Activity Scale (TAS), and modernized Saltin-Grimby Physical Activity Level Scale (SGPALS) were administered at baseline to validate the ARS. Construct validity and responsiveness of the ARS were evaluated by testing predefined hypotheses regarding correlations between the ARS, KOOS, TAS, and SGPALS. The Cronbach alpha, intraclass correlation coefficients, absolute reliability, standard error of measurement, smallest detectable change, and Spearman rank-order correlation coefficients were calculated.
Results:
The ARS showed good internal consistency (α ≈ 0.96), good test-retest reliability (intraclass correlation coefficient >0.9), and no systematic bias between measurements. The standard error of measurement was less than 2 points, and the smallest detectable change was less than 1 point at the group level and less than 5 points at the individual level. More than 75% of the hypotheses were confirmed, indicating good construct validity and good responsiveness of the ARS.
Conclusion:
The Swedish version of the ARS is valid, reliable, and responsive for evaluating the level of activity based on the frequency of participation in high-demand knee sports activities in young adults with a knee injury.
Injuries to the knee, such as trauma to ligaments, menisci, and/or cartilage, are common in young adults and middle-aged patients 16 and constitute a major risk factor for the development of knee osteoarthritis (OA). 21 The evaluation of outcomes after treatment of a knee injury includes objective clinical measures, such as range of motion, performance tests, and muscle strength, and generic and/or disease-specific patient-reported outcome measures (PROMs). 15 PROMs that are important and relevant to the patient include those for pain, function, quality of life, and level of physical activity. 5 Return to physical activity at the previous level or at a modified activity level are common goals often used to measure success of treatment of a knee injury. 5,11,15,22,24
Preinjury, current, and desired physical activity levels are assessed for both clinical and research purposes. The Tegner Activity Scale (TAS) 8 was developed for and is recommended for patients with a knee injury. 14 The TAS measures the activity level based on the type of participation in specific work and sports activities and, to a certain extent, the intensity of participation. 8,29 The Activity Rating Scale (ARS) for disorders of the knee 17 (Appendix 1) could constitute a complement to the TAS, as this scale evaluates the frequency of participation in different sport-specific tasks. The ARS consists of 4 items (ARS1-4), and the frequency of participation is rated in 4 separate activities with high demands on knee function: running (ARS1), cutting (ARS2), decelerating (ARS3), and pivoting (ARS4). The ARS is scored on a 5-point scale from 0 (no participation) to 4 (participation ≥4 times/wk), with a total score ranging from 0 to 16. The ARS has good face, content, and construct validity and is a reliable instrument for the evaluation of activity participation among patients with knee disorders, including ligament injuries. 5 A Swedish version of the ARS has not yet been validated.
The aims of this study were to (1) translate and cross-culturally adapt the ARS into Swedish and (2) assess measurement properties of the Swedish version of the ARS.
Methods
The measurement properties of the ARS were assessed according to the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) checklist. 18,19,30
Translation and Cross-Cultural Adaptation
The translation and cross-cultural adaptation of the Swedish version of the ARS followed recommended guidelines (Figure 1). 9,19
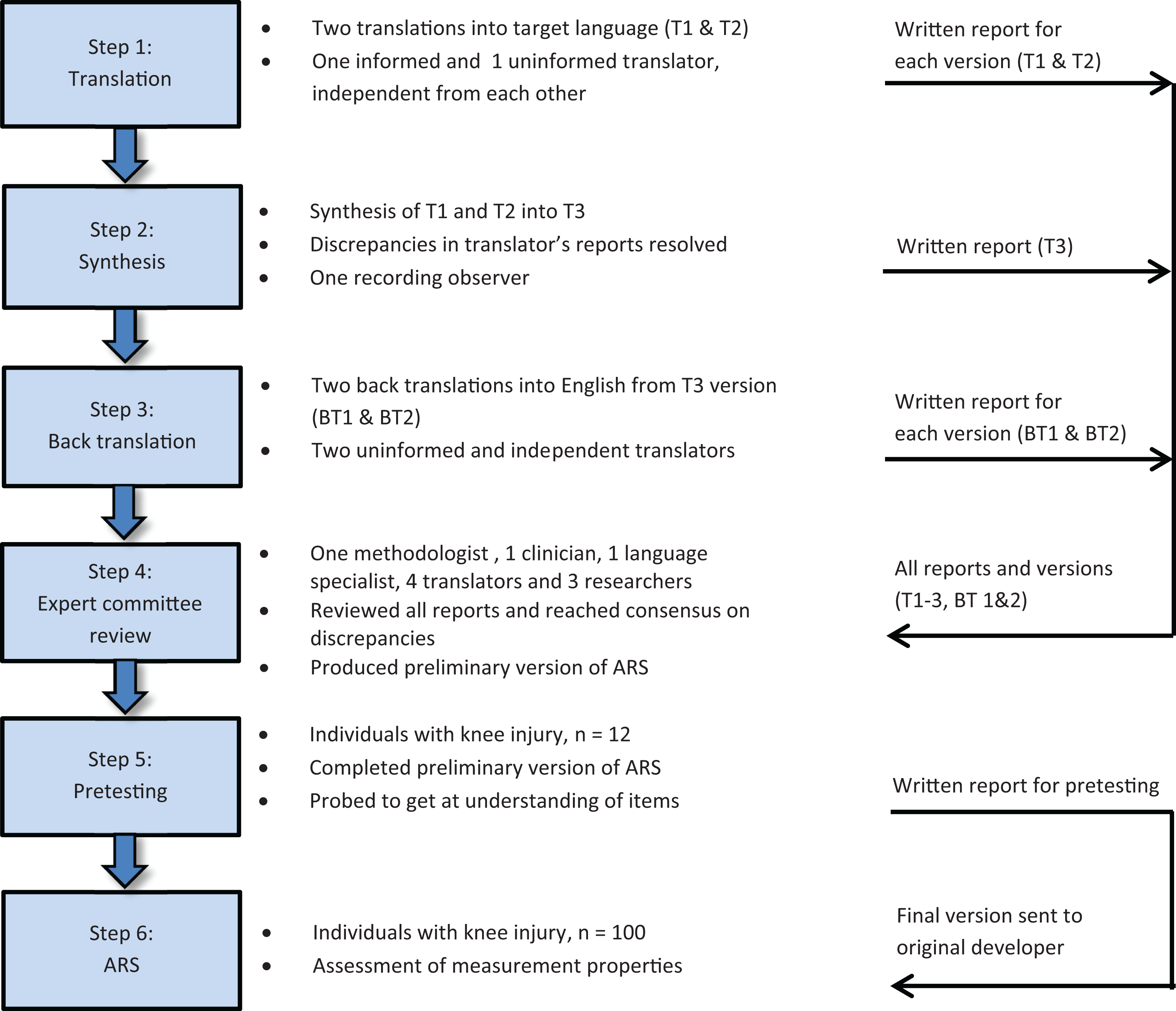
Graphic representation of the translation and cross-cultural adaptation process of the Activity Rating Scale (ARS).
Step 1: Initial Translation
The original version of the ARS was translated from English into Swedish by 2 independent translators native to the Swedish language. One of the translators (T1) was aware of the concepts being measured and had previous experience in the use of the ARS as a physical therapist. The other translator (T2) was a professional translator with no medical background and was unfamiliar with the concepts of the ARS.
Step 2: Synthesis of the Translations
The discrepancies between the 2 translated versions (T1 and T2) were resolved by the translators together with a recording process leader, resulting in a single preliminary Swedish version (T3). The process used, problems experienced, and their resolution were carefully documented in a written report.
Step 3: Back Translation
The translation process of the preliminary version (T3) back into English was performed independently by 2 native English translators (BT1 and BT2) uninformed about the constructs being measured and blinded to the original version of the ARS.
Step 4: Expert Committee Review
To consolidate all the translated versions into a preliminary one, a multidisciplinary committee consisting of the translators, the coauthors, a health professional, a language professional, and a methodologist was formed. The committee reviewed and discussed the original version of the ARS and all translations (T1, T2, T3, BT1, and BT2) together with corresponding written reports. After a consensus was reached on wording, a preliminary Swedish version of the ARS and a written report of the synthesis process were completed by the committee.
Step 5: Pretesting
The preliminary version was completed by a sample of the target population (n = 12) for pretesting and the evaluation of comprehensibility. Inclusion criteria for the participants included undergoing rehabilitation for a knee injury (ligament, meniscal, or chondral injury) or posttraumatic knee OA; age 15 to 49 years; and ability to read, write, and understand the Swedish language. Participants were excluded if (1) they were not undergoing rehabilitation for their knee injury at the time of inclusion; (2) their knee injury did not limit activities; (3) they had other diseases or disorders overriding the knee injury; (4) they had an overuse knee injury (such as runner’s or jumper’s knee); or (5) they were physically inactive (TAS score <3). After completing the ARS, the participants were interviewed by a physical therapist to identify their opinions on the usability, applicability, and completeness of the questionnaire. The participants answered questions about the wording of the instructions and items and their overall impression of the questionnaire. The Three-Step Test Interview was used for this procedure. 10
Step 6: Assessment of the Measurement Properties of the ARS
Between December 2014 and May 2016, 167 participants fulfilling the same criteria as in pretesting were included in this study. The participants were from 7 physical therapy clinics in Sweden and were in different phases of knee injury rehabilitation when completing the baseline questionnaires. Sixty-seven participants were excluded for various reasons (Figure 2), leaving 100 participants for data analyses (Table 1). When more than 50 participants 20 had completed the 4-month follow-up, this subgroup (n = 70) was included in the responsiveness assessment (Table 2 and Figure 2). As part of the validation and responsiveness assessments, the TAS, the Saltin-Grimby Physical Activity Level Scale (SGPALS), the Knee injury and Osteoarthritis Outcome Score (KOOS), and anchor questions were administered to the participants simultaneously with the ARS. The measurement properties of the Swedish version of the ARS were investigated using 2 recall periods: frequency of participation in high-demand knee activities during the past year (ARSYear) and during the past month (ARSMonth).
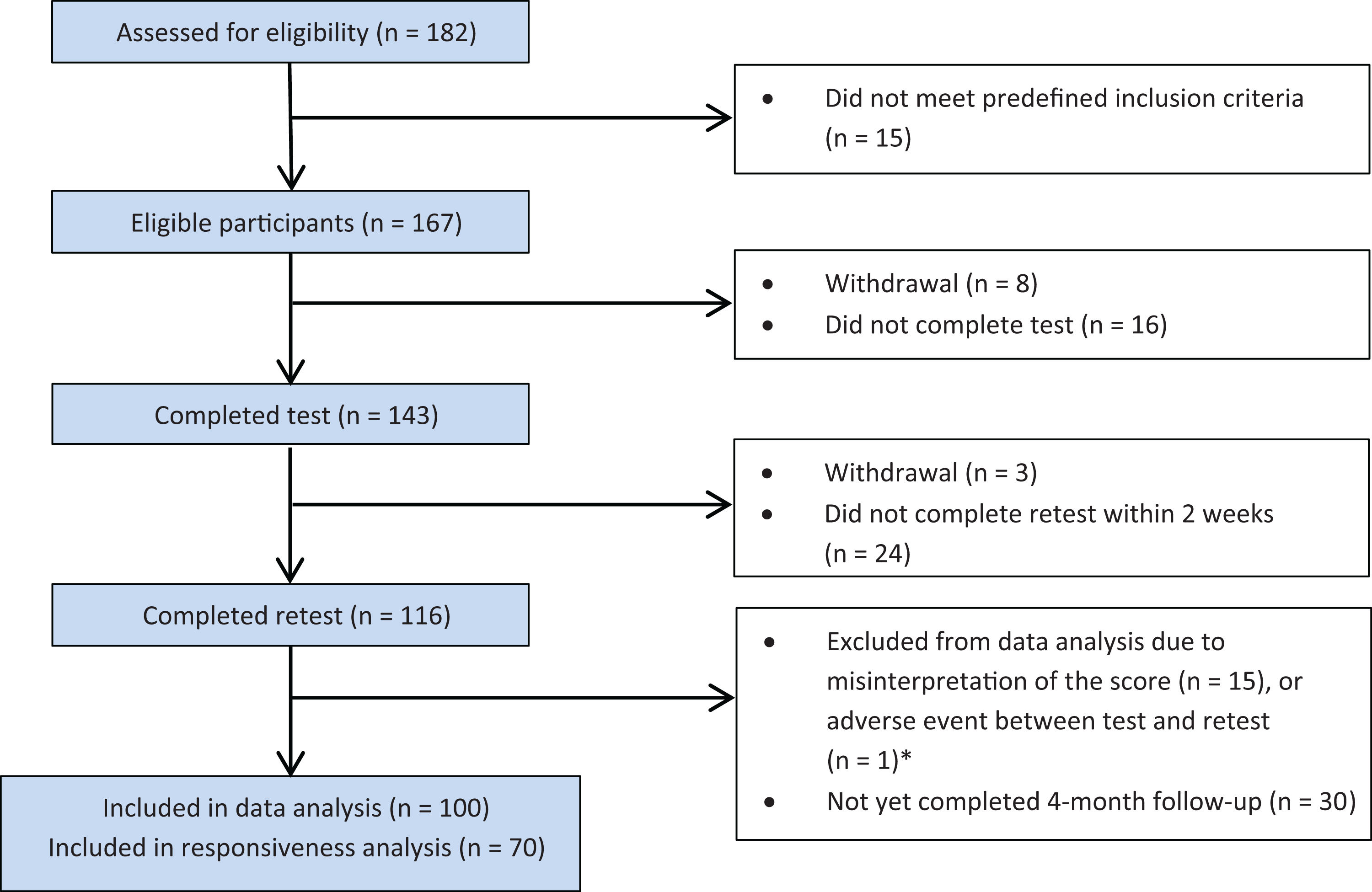
Flow chart of the recruitment, test-retest, and data analysis process. *Sixteen participants were contacted because of reporting major differences in Activity Rating Scale scores (≥12 points) between the 2 test occasions. Only one of these participants reported an adverse event between the test occasions. Fifteen participants confirmed misinterpretation of the recall time to account for the differences in scores.
Baseline Characteristics of Study Participants (N = 100) a

a ACL, anterior cruciate ligament; IQR, interquartile range; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament.
b Concomitant injuries: meniscal, cartilage, MCL, LCL, and/or posttraumatic osteoarthritis (n = 40).
c Concomitant injuries: posttraumatic osteoarthritis (n = 1).
d Concomitant injuries: meniscal, cartilage, or patellar dislocation (n = 2).
e Concomitant injuries: MCL/LCL.
f n = 75.
Scores at Baseline and 4-Month Follow-up and Differences in Scores (n = 70) a
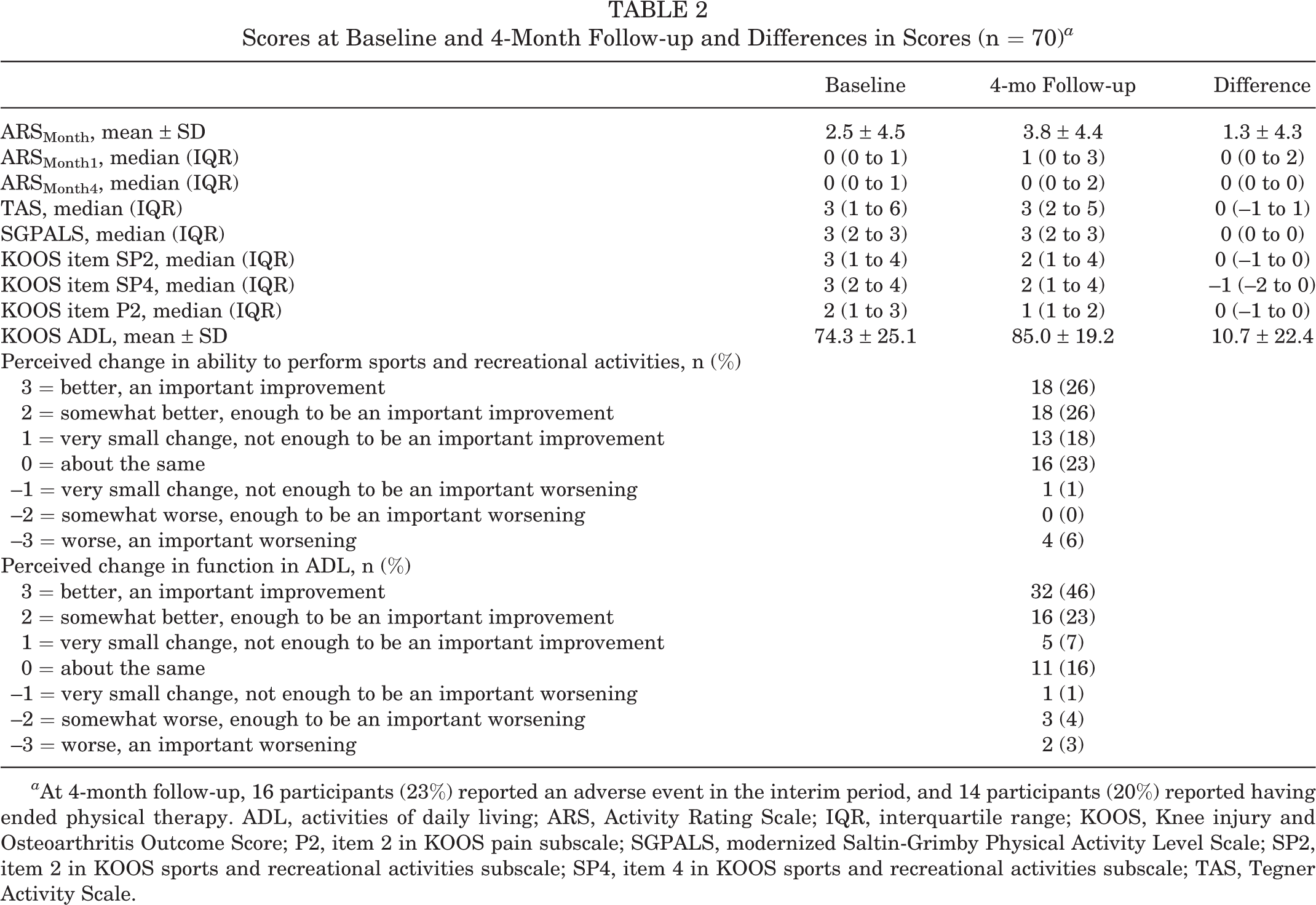
a At 4-month follow-up, 16 participants (23%) reported an adverse event in the interim period, and 14 participants (20%) reported having ended physical therapy. ADL, activities of daily living; ARS, Activity Rating Scale; IQR, interquartile range; KOOS, Knee injury and Osteoarthritis Outcome Score; P2, item 2 in KOOS pain subscale; SGPALS, modernized Saltin-Grimby Physical Activity Level Scale; SP2, item 2 in KOOS sports and recreational activities subscale; SP4, item 4 in KOOS sports and recreational activities subscale; TAS, Tegner Activity Scale.
The study was approved by the Research Ethics Committee at Lund University (Dnr. 2014/672), and all participants gave their written informed consent. The ethical principles for medical research proposed in the Declaration of Helsinki were followed.
Tegner Activity Scale
The TAS is an instrument designed to evaluate patients with a knee injury and their level of activity based on specific sports participation and/or line of work. The TAS score ranges from 0 (sick leave or disability due to knee problems) to 10 (participation in competitive sports at a national or international level). The TAS is responsive and has shown adequate validity and reliability for assessing activity levels in patients with a knee injury (anterior cruciate ligament [ACL] and meniscal injury, patellar dislocation, and knee OA). 3,5,29
Saltin-Grimby Physical Activity Level Scale
The SGPALS is a 4-level rating scale used to assess the level of leisure-time physical activity, where 1 represents physical inactivity and 4 represents regular hard physical training for competitive sports. 25,27 The scale has shown good reliability and validity in a population-based sample. 1,25
Knee injury and Osteoarthritis Outcome Score
The KOOS is a 42-item knee-specific tool used to assess self-reported measures of the knee. 26 The KOOS consists of 5 subscales, covering pain, symptoms, activities of daily living (ADL), function in sports and recreational activities (Sport/Rec), and quality of life, with separate normalized subscores ranging from 0 (worst) to 100 (best). The KOOS Sport/Rec subscale contains a total of 5 items. In item SP2 (KOOS Sport/Rec, item 2), trouble with running is reported, and in item SP4 (KOOS Sport/Rec, item 4), trouble with twisting/pivoting is reported, with scores ranging from 0 (no trouble) to 4 (extremely troubled). The KOOS pain subscale consists of 9 items in total. In item P2 (KOOS pain, item 2), the experience of pain during twisting/pivoting of the knee is reported, with scores ranging from 0 (no pain) to 4 (extreme pain). The KOOS Sport/Rec and ADL subscales, as well as single items from the KOOS Sport/Rec and pain subscales, were used in the present study. The KOOS has adequate validity and reliability for use in patients with a knee injury that can result in posttraumatic knee OA (eg, ACL injury/reconstruction, meniscal or chondral injury). 6
Anchor Questions: Participant’s Perception of Change
To assess perceived change, the participants responded to 2 anchor questions at the 4-month follow-up: “How would you describe your ability to perform sports and recreational activities (running, jumping, squatting, kneeling, twisting/pivoting on your injured knee) now compared with 4 months ago?” and “How would you describe your function in daily living activities (sitting, standing, walking on stairs, dressing, housework) now compared with 4 months ago?” The response options were 3 = better, an important improvement; 2 = somewhat better, enough to be an important improvement; 1 = very small change, not enough to be an improvement; 0 = no change; –1 = very small change, not enough to be an important worsening; –2 = somewhat worse, enough to be an important worsening; and –3 = worse, an important worsening.
Data Analysis
Statistical analyses were performed using SPSS for Windows, version 22.0 (IBM Corp). Graphical interpretation of the data and tests for normality showed that assumptions for a normal distribution of the ARS were not met, and therefore, nonparametric tests were used in the analyses. There were no missing items for any of the participants (N = 100). P values ≤.05 were considered statistically significant.
Floor and Ceiling Effects
Floor and ceiling effects were considered to be present if more than 15% of the participants achieved the lowest (0) or highest score (16). 31 The Mann-Whitney U test was used for comparing participants who had sustained their injury during sports and those who had sustained their injury during other activities.
Face Validity
Face validity of the ARS was evaluated during the cross-cultural adaptation process by members of the expert committee and was further evaluated through qualitative analysis of the pretest interviews.
Reliability
Internal Consistency
Scale and item internal consistency were measured using the Cronbach alpha to investigate the level of reliability. A low Cronbach alpha indicates that summarization of the items is groundless, and a very high Cronbach alpha indicates a surplus of ≥1 items. A Cronbach alpha of .70 to .95 was accepted as a measure of good internal consistency. 30
Test-Retest Reliability
To determine relative test-retest reliability, the intraclass correlation coefficient (ICC) was derived from a 2-way random-effects model (absolute agreement definition). An ICC of ≥0.70 was considered as the minimum standard for reliability testing. 31 Absolute reliability was assessed using Bland-Altman plots with 95% limits of agreement (LOA), that is, the mean difference ±1.96 * SDdiff. 2 The participants completed the questionnaire on 2 different occasions 1 to 2 weeks apart (median, 7 days; interquartile range, 7-9 days). This time period was chosen to prevent recall bias and a change in activity levels among the participants. 31
Measurement Error
The standard error of measurement (SEM = SD1 × √ [1 – r], with SD1 representing the SD at baseline and r representing the ICC), was calculated including systematic differences to investigate to what extent the scores were the same for the repeated measurements. 20 The smallest detectable change (SDC) was determined both at an individual level (SDCInd = 1.96 × √2 × SEM) and at a group level (SDCGroup = SDCInd/√n). 30
Construct Validity
To investigate if the ARS validly measures the construct of interest, convergent construct validity was assessed by comparing the scores of the ARS with other knee-specific PROM scores. Spearman rank-order correlation analyses were used to assess the associations. A Spearman rho correlation coefficient (rs ) ≥ 0.50 was considered large, 0.30 to <0.50 was considered moderate, and 0.10 to <0.30 was considered small. 4 Construct validity was evaluated by testing the following predefined hypotheses.
Outcome Measure–Related Hypotheses
1. ARSMonth scores should correlate at least moderately (r
s ≥ 0.30) with TAS scores. Reasoning: These scales measure the same construct, knee-specific activity participation, through the assessment of frequency (ARS) versus type and intensity (TAS). 2. ARSMonth scores should correlate higher with TAS scores than with SGPALS scores. Reasoning: The TAS is a knee-specific measure, whereas the SGPALS is a generic measure. 3. ARSYear scores should correlate higher with SGPALS scores than with TAS scores. Reasoning: The time periods asked for in these scales are more similar for ARSYear (participation during the past year) and the SGPALS (participation during the past year) than for the TAS (current participation). 4. ARSMonth1 scores should correlate at least moderately (r
s ≤ –0.30) with KOOS item SP2 subscores. Reasoning: The frequency of running should be reflected by the trouble experienced during running. 5. ARSMonth4 scores should correlate at least moderately (r
s ≤ –0.30) with KOOS item SP4 subscores. Reasoning: The frequency of performing pivoting activities should be reflected by the trouble experienced during the performance of these activities.
Injury-Related Hypotheses
6. ARSMonth scores should correlate at least moderately (r
s ≥ 0.30) with time since injury. Reasoning: A longer time since injury should implicate better function and thereby a higher frequency of activity participation.
7. ARSMonth scores should correlate at least moderately (r
s ≥ 0.30) with time since surgery. Reasoning: A longer time since surgery should implicate better function and thereby a higher frequency of activity participation.
8. ARSYear scores should correlate at least moderately (r
s ≥ 0.30) with injuries sustained during sports activity. Reasoning: Injuries sustained during sports activity should reflect a higher frequency of sport-specific activity participation.
Results consistent with the predefined hypotheses, confirming at least 75% of the hypotheses, were accepted as a measure of good construct validity. 30
Responsiveness
Responsiveness was defined as the ability of an instrument to detect change over time (Δ) in the construct being measured. 20 Seven predefined hypotheses were used to investigate the responsiveness of ARSMonth:
1. ΔARSMonth scores should have low to moderate correlation (r
s ≥ 0.20) with ΔTAS scores. Reasoning: An increased knee-specific activity participation should reflect an increase in knee-specific activity levels.
2. ΔARSMonth scores should correlate higher with ΔTAS scores than with ΔSGPALS scores. Reasoning: An increased knee-specific activity participation should better reflect increased knee-specific than generic activity levels.
3. ΔARSMonth1 scores should have low to moderate correlation (r
s ≤ –0.20) with ΔKOOS item SP2 subscores. Reasoning: An increased frequency of running should be reflected by less trouble experienced during running.
4. ΔARSMonth4 scores should have low to moderate correlation (r
s ≤ –0.20) with ΔKOOS item SP4 subscores. Reasoning: An increased frequency of pivoting activities should be reflected by less trouble experienced during such activities.
5. ΔARSMonth4 scores should have low to moderate correlation (r
s ≤ –0.20) with ΔKOOS item P2 subscores. Reasoning: An increased frequency of running should be reflected by less pain experienced during running.
6. ΔARSMonth scores should have low or no correlation (r
s ≤ 0.10) with ΔKOOS ADL subscores. Reasoning: An increased frequency of participation in sport-specific activities differs from increased knee function in ADL.
7. ΔARSMonth scores should correlate higher with a perceived change in the ability to perform sports and recreational activities than with a perceived change in function in ADL. Reasoning: An increased frequency of participation in sport-specific activities should be better reflected by a higher perceived change in the ability to perform such activities than a higher perceived change in function in ADL.
The analyses of associations were performed using Spearman rank-order correlations, with rs ≥ 0.50 considered large, 0.30 to <0.50 were considered moderate, and 0.10 to <0.30 were considered small. 4 Results consistent with and confirming at least 75% of the predefined hypotheses were accepted as a measure of good responsiveness. 30
Results
Steps 1-3: Translation and Cross-Cultural Adaptation
The majority of the items in the English version of the ARS were translated into Swedish without any difficulty. The expert committee identified some issues regarding the wording of the second and fourth items. The word “cutting” in the English version was considered to describe a very fast and complex movement, and there was no consensus of a comparable word in Swedish. Hence, the final formulation in the Swedish version was changed to “fast change of direction.” In the cultural adaptation, 3 changes were made to the fourth item: “pivoting.” (1) The recited sports were not considered to cover Swedish sports with high rates of knee injuries. Accordingly, it was determined to change “kicking, throwing, hitting a ball” to “ball sports/games” with the addition of the sample sports “soccer, team handball, floorball, basketball, and racquet sports.” (2) Tennis and squash were excluded as sample sports and were instead compiled to racquet sports. (3) Golf was excluded as a sample sport, as it was considered to fall under the term of “ball sports/games.” Furthermore, the expert committee suggested an adjustable recall period, that is, 1 month or 1 week, as an option to 1 year in the English version to facilitate treatment follow-up. This comprehensive review resulted in a preliminary Swedish version of the ARS.
Steps 4-5: Face Validity and Pretesting
The expert committee and the pretesting participants considered the Swedish version of the ARS to be a comprehensive and appropriate outcome measure for knee-specific activity levels. The interviews generated 2 proposals for additions: (1) “physical contact displacing a player during play” to be added as an item and (2) treadmill and cross-trainer to be included as samples in the item “running.” “Physical contact with another player” was considered an external event and not a physical component of function, the item “running” was considered to cover the activity of running regardless of the surface, and cross-trainer exercise was not considered to equal the physical impact of running. Therefore, these proposals were dismissed. No modifications of the Swedish version of the ARS were made after pretesting.
Step 6: Assessment of Measurement Properties
Floor and Ceiling Effects
At baseline, 56% reported the lowest score (0) in ARSMonth. For ARSYear, a floor effect of 22% and a ceiling effect of 20% were observed. Participants who had sustained their injury during sports activity had a higher frequency of performing high-demand knee activities, as indicated by a significantly higher ARSYear score (mean, 8.6 ± 5.7), than those who had sustained an injury during other activity (mean, 2.8 ± 3.9) (P < .001). When analyzing these groups separately, there was no floor effect for ARSYear (14.5%) in the group of participants with an injury sustained during sports activity, while the floor effect (59%) remained for the group of participants with an injury sustained during other activity.
Reliability
Internal Consistency
The Cronbach alpha values for all 4 items of ARSMonth and ARSYear were above 0.95 (Table 3).
ARS Scores, Test-Retest Reliability, Internal Consistency, SEM, and SDC (N = 100) a

a Range of ARS scores = 0 (no participation) to 16 (very frequent participation). ARS, Activity Rating Scale; ICC, intraclass correlation coefficient; LOA, limits of agreement; SDCGroup, smallest detectable change at group level; SDCInd, smallest detectable change at individual level; SEM, standard error of measurement.
Test-Retest Reliability
There was no systematic change between test sessions (Figure 3), the ICC values were above 0.9, and the LOA values were approximately ±6 (see Table 2). There was no difference in scores between test and retest for 60% and 44% of the participants in ARSMonth and ARSYear, respectively. Differences between 1 and 5 points in the test-retest scores were noted for 32% (ARSMonth) and 45% (ARSYear) of the participants, respectively (Figure 4).

Test-retest reliability of the Swedish version of the Activity Rating Scale (ARS) presented as Bland-Altman plots with limits of agreement. Two assessments were performed 2 weeks apart. (A) ARSMonth. (B) ARSYear. The 95% CIs contained 0, indicating no systematic bias between the 2 measurements. LOA, limits of agreement.

Change in Activity Rating Scale (ARS) scores between test and retest. (A) ARSMonth. (B) ARSYear.
Measurement Error
The SEM was below 2 points. The SDC was below 1 point at a group level and below 5 points at an individual level (Table 3).
Construct Validity
Seven of the 8 (88%) predefined hypotheses were confirmed (Table 4). The single hypothesis being rejected was the one regarding the correlation between higher ARSMonth scores and a longer time since injury (r s = 0.134). The correlations between the ARS score and TAS, SGPALS, and single KOOS item scores were r s ≥ 0.310. A higher ARS score correlated at least moderately with a longer time since surgery and injury sustained during sports activity (r s ≥ 0.342).
Spearman Rho Correlation (r s) Between ARS Score and Other Outcome Measures for Construct Validity (N = 100) a
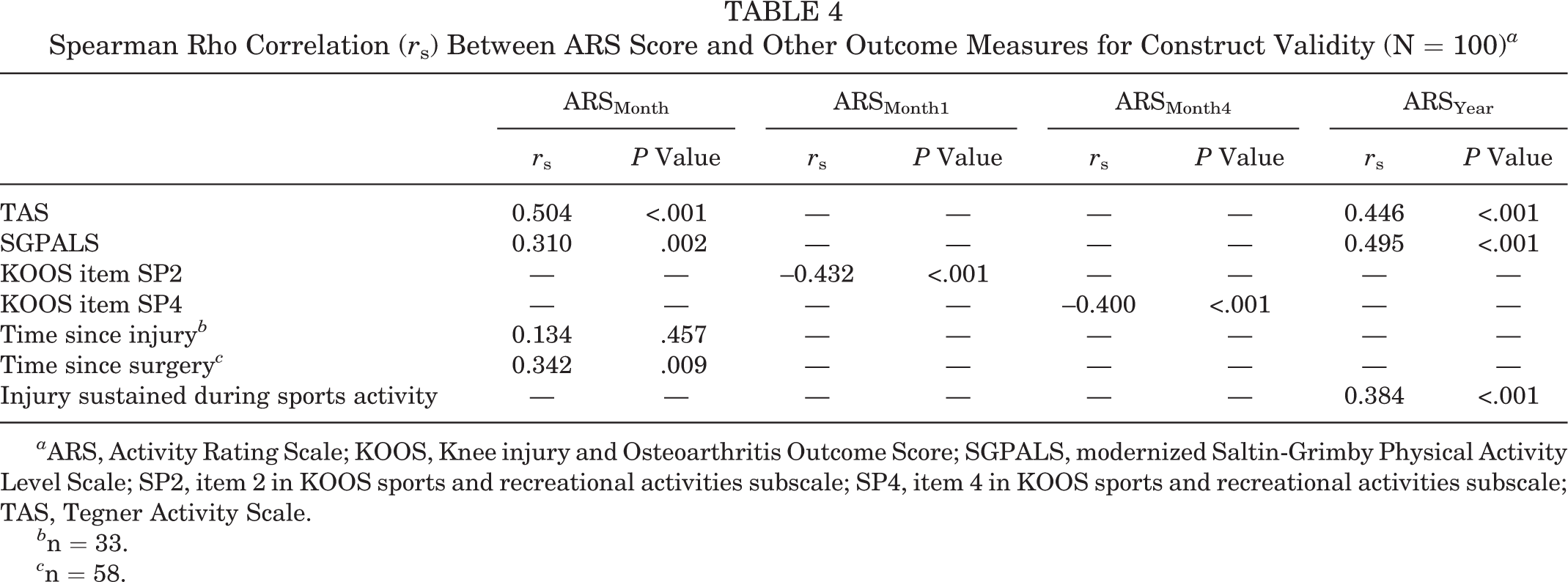
a ARS, Activity Rating Scale; KOOS, Knee injury and Osteoarthritis Outcome Score; SGPALS, modernized Saltin-Grimby Physical Activity Level Scale; SP2, item 2 in KOOS sports and recreational activities subscale; SP4, item 4 in KOOS sports and recreational activities subscale; TAS, Tegner Activity Scale.
b n = 33.
c n = 58.
Responsiveness
Six of the 7 (86%) predefined hypotheses were confirmed (Table 5). The hypothesis regarding changes in ARSMonth and KOOS item P2 scores was rejected (r s = –0.027). A change in the ARS score correlated higher with a change in the TAS score (r s = 0.229) than with the SGPALS score (r s = 0.197). The correlations between a change in the ARS score and a change in single-item subscores of the KOOS Sport/Rec subscale and a perceived change in the ability to perform sports and recreational activities were r s ≥ –0.270. A change in the ARS score correlated with a change in the KOOS ADL subscore and a perceived change in function in ADL (r s ≥ 0.011).
Spearman Rho Correlation (r s) Between Change (Δ) in ARSMonth Score and Change in Other Outcome Measures for Responsiveness (n = 70) a

a ADL, activities of daily living; ARS, Activity Rating Scale; KOOS, Knee injury and Osteoarthritis Outcome Score; P2, item 2 in KOOS pain subscale; SGPALS, modernized Saltin-Grimby Physical Activity Level Scale; SP2, item 2 in KOOS sports and recreational activities subscale; SP4, item 4 in KOOS sports and recreational activities subscale; TAS, Tegner Activity Scale.
Discussion
The results show that the ARS was successfully translated and cross-culturally adapted into Swedish. The Swedish version of the ARS has good reliability and validity to evaluate the frequency of high-demand knee activities during the past year, or the past month, in young to middle-aged adults with a knee injury (Appendix 2). In addition, ARSMonth had good responsiveness, fulfilling 12 of 14 requirements of an excellent score in the COSMIN checklist. 20
Because more than 75% of the predefined hypotheses were confirmed, 30 it can be concluded that the Swedish version of the ARS has good construct validity. As expected, a higher frequency of performing high-demand knee activities correlated with a higher activity level, less trouble with running and pivoting, and a longer time since surgery and injury sustained during sports activity. Conversely, a longer time since injury did not correlate with a higher frequency of performing high-demand knee activities. One explanation for this may be that some patients modify their activity and reduce their participation in pivoting and high-demand knee activities based on clinical advice after the injury. 12,22
A majority of the participants were included at a stage in their treatment when high-demand knee exercises, that is, running, had not yet been introduced. This may explain the floor effects observed in ARSMonth, suggesting that this measure may not be suited for use in the early treatment phases. The absence of floor effects for ARSYear, when only participants with an injury sustained during sports activity were included in the analysis, supports that ARSYear can be used for a population active in sports. However, the ceiling effect for ARSYear could implicate a need to increase the range of the scale to detect even higher frequencies of participation in high-demand knee activities.
The high internal consistency noted for both ARSMonth and ARSYear could indicate a surplus of ≥1 items. 30 However, because the coefficients only marginally exceeded the limit of 0.95, and the ARS only includes 4 items, the internal consistency can be considered to be good. The high test-retest reliability of the Swedish version of the ARS is in line with previous reports, 17,23 and the low SDCGroup values suggest that the ARS is useful for a group comparison. The relatively high SEM, SDCInd, and LOA values suggest that the change must exceed 6 points to exclude measurement errors and thus detect a real difference for a patient, for example, before and after treatment. Our findings of lower values to detect a change at a group level and higher values at an individual level are comparable to other studies on measurement properties of knee-specific PROMs. 6,13,28
There is no gold standard for the construct “frequency of performing high-demand knee activities.” Therefore, to evaluate the responsiveness of the ARS, we used predefined hypotheses regarding correlations in the change in the ARS score and the change in comparable instrument or construct scores. Our results suggest that ARSMonth can detect changes in the frequency of performing high-demand knee activities. An explanation for the rejected hypothesis (change [eg, increase] in frequency of pivoting and change [eg, decrease] in pain during twisting and pivoting) could be that patients with a knee injury report low changes in KOOS pain subscores 26 ; thus, using pain as a construct may not be appropriate for this population. However, because this was the only rejected hypothesis, the responsiveness of the ARS remains good.
The majority of the participants (74%) in the present study had an ACL injury. Therefore, a subgroup analysis, excluding participants with an ACL injury, was performed. The results for reliability were unchanged; however, because of the small sample size (n = 22-26), no definite conclusions can be drawn about measurement properties for the subgroup.
A main strength of this report is that the COSMIN guidelines were followed. In addition, the quality of the study was high because the sample size was adequate, 30 the response rate was high, 7 and the results can be generalized at least to young adults with an ACL injury. On the other hand, the heterogeneity of the cohort in terms of age, sex, and time spent in rehabilitation may constitute limitations, possibly reflected by the high floor effects, measurement errors, and SDCs. Another limitation is the recall period of ARSYear, which may have induced recall bias, potentially influencing the results.
Conclusion
The Swedish version of the ARS is valid, reliable, and responsive for evaluating the level of activity based on the frequency of participation in high-demand knee sports activities in young adults with a knee injury.
Footnotes
Acknowledgment
The authors thank the following physical therapy clinics for facilitating the recruitment of participants for this study: Kulan Idrottsskadecentrum in Malmö, Arena Fysio and Fysiokliniken City in Helsingborg, Motions-och idrottskademottagningen in Höör, Gerdahallen in Lund, and iKlinik in Malmö and Lund.
One of more of the authors has declared the following potential conflict of interest or source of funding: This research was funded by the Swedish Research Council (2009-1447), the Crafoord Foundation, the Swedish Rheumatism Association, the Swedish Research Council for Sport Science, and the Faculty of Medicine at Lund University.
Ethics approval for this study was obtained from the Research Ethics Committee at Lund University (Dnr. 2014/672).
Appendix 1 Activity Rating Scale – Original version (Marx et al 17 2001)

|
|
|
|
|
|
|
|---|---|---|---|---|---|
|
|
|||||
|
|
|||||
|
|
|||||
|
|
Appendix 2 Activity Rating Scale (ARS) – Svensk version (Flosadottir et al 2017)

|
|
|
|
|
|
|
|---|---|---|---|---|---|
|
|
|||||
|
|
|||||
|
|
|||||
|
|