
Abstract

Arthroscopic debridement and/or lavage has been shown to have no beneficial effect on the natural history of osteoarthritis (OA), nor is it indicated as a primary treatment in the management of OA. However, this does not preclude the judicious use of arthroscopic surgery, when indicated, to manage symptomatic coexisting abnormalities in the presence of OA or degeneration. Partial medial meniscectomy is not indicated as an initial treatment for atraumatic tears of degenerative menisci, excluding bucket-handle tears and surgeon-assessed locked or locking knees.
Arthroscopic Surgery in the Presence of Osteoarthritis or Degeneration
There are certain clinical scenarios in which arthroscopic surgery, in the presence of OA, may be appropriate. These include, but are not necessarily limited to, the following: known or suspected septic arthritis; symptomatic nonrepairable meniscal tears after the failure of an appropriate trial of a structured rehabilitation program; symptomatic loose bodies; surgeon-assessed locked or locking knees; traumatic or atraumatic meniscal tears that require repair; inflammatory arthropathy requiring synovectomy; synovial abnormalities requiring biopsy or resection; large unstable chondral abnormalities causing surgeon-assessed locking or locked knees; as an adjunct to, and in combination with, other surgical procedures as appropriate for OA (eg, high tibial osteotomy and patellofemoral realignment); and diagnostic arthroscopic surgery when the diagnosis is unclear on magnetic resonance imaging (MRI) or MRI is not possible and the symptoms are not of OA.
The decision to proceed with arthroscopic surgery in the presence of OA or degeneration should be made by the treating orthopaedic surgeon: after a careful review of the clinical scenario, particularly the assessment of the relative contributions of OA and the arthroscopically treatable abnormality, to the patient’s symptoms; with knowledge of the relevant evidence base, as listed in this work; after an appropriate trial of structured rehabilitation; and after a thoughtful discussion with the patient about the relative merits of the procedure versus ongoing nonoperative treatment.
Definitions
OA, or degenerative joint disease, is a progressive clinical disorder of joints characterized by gradual diffuse loss of articular cartilage, effects on the underlying bone, and secondary compromise of joint function. This should be distinguished from focal articular cartilage abnormalities in an otherwise normal joint.
There is a spectrum of severity of OA from minor partial-thickness articular cartilage abnormalities to large areas of full-thickness loss. Clinical decision making requires a careful assessment of the degree of arthritis, its likely contribution to the symptoms, and the potential contribution of additional abnormalities to those symptoms.
The concept of degenerative versus traumatic, in regard to meniscal lesions and tearing, is arbitrary. 15 No universally accepted definition of degeneration or degenerative change exists, and commonly used clinical diagnostic descriptors lack validity.
Assessment and Interpretation of MRI
While plain radiography is the preferred initial imaging modality, MRI remains an excellent adjunct both to clinical decision making and to guiding the use of surgery. In particular, it can be used to more accurately assess the degree of arthritis and to look for and assess additional abnormalities that may correlate with a patient’s symptoms. MRI scans should be interpreted carefully by the treating surgeon, in combination with direct review of the imaging, when determining the clinical relevance of the findings. MRI descriptions of meniscal tearing, degeneration, and lesions in the absence of trauma lack validity. Further information on the appropriate radiological investigation of knee OA can be obtained from the statement, “Joint AKS-AMSIG Submission to the Australian Commission on Quality and Safety in Healthcare on the Radiological Investigation of Knee Osteoarthritis” (http://www.kneesociety.org.au/resources/Joint-AKS-AMSIG-submission-ACQSH-investigation-knee-osteoarthritis.pdf).
Systematic Review: Arthroscopic Surgery in the Presence of Osteoarthritis
Introduction
Our aim was to examine the evidence of effectiveness, inclusion and exclusion criteria, effects of age, and adverse events in existing knee arthroscopic surgery randomized controlled trials (RCTs), with a view to the formulation of clinical indication guidelines based on International Classification of Diseases–10th Revision (ICD-10) codes for knee arthroscopic surgery in the presence of degeneration or OA.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for systematic reviews was utilized for this work. 11
Literature Search and Study Selection
In December 2015, a systematic search for clinical indications in Medline, Embase, CINAHL, and the Cochrane Central Register of Controlled Trials was undertaken. The keywords “arthroscopy” and “knee,” or variations of them, were used. Limitations to clinical trials and human studies were applied. No search restrictions for follow-up time, study size, or date of publication were set.
Eligibility Criteria
The inclusion and exclusion criteria were as follows.
Inclusion criteria:
RCTs assessing the effectiveness of arthroscopic surgery involving meniscal surgery, debridement, chondroplasty, loose body removal, or any combinations, with or without clinical or radiographic OA, compared with nonoperative treatment, sham surgery, or lavage.
English-language reports.
Publication in a peer-reviewed journal.
Exclusion criteria:
All criteria for inclusion had to be satisfied, and other systematic reviews or meta-analyses were excluded.
Data Extraction
Titles and/or abstracts of studies that were retrieved using the search strategy were screened independently by 2 review authors to identify studies that potentially met the inclusion criteria. The full-text versions of these potentially eligible studies were retrieved and independently assessed for eligibility by the 2 review team members. Any disagreement over the eligibility of a particular study was resolved through consensus with the addition of a third reviewer.
A standardized form was used to extract data from the included studies for the assessment of study quality and evidence synthesis. Extracted information included study population, primary diagnosis, inclusion criteria, exclusion criteria, details of the intervention, details of the comparator, study methodology, outcomes and times of measurement, and power analysis. Two review authors extracted the data independently.
If 2 separate studies with the same authors and the same intervention had overlapping dates of patient enrollment, then only 1 study was included. In this situation, the reviewer selected the study with the longer follow-up. If a different data analysis or subanalysis was undertaken, then the supplemental study was included.
ICD-10 Diagnosis Matching
ICD-10–Clinical Modification (ICD-10-CM) codes or ICD-10–Procedure Coding System (ICD-10-PCS) codes were matched by 2 review authors to the inclusion and exclusion criteria of all matched studies. ICD-10-CM codes were developed by the United States Centers for Disease Control and Prevention in conjunction with the National Center for Health Statistics for outpatient medical coding and reporting, as published by the World Health Organization. ICD-10-PCS codes were developed by the United States Centers for Medicare and Medicaid Services as a system of procedural codes to classify all health interventions by medical professionals. 1
Results
Knee Arthroscopic Surgery Outcome Studies
Fourteen RCTs of arthroscopic knee surgery (Table 1) fulfilled the search criteria (Figure 1) in 3 different primary clinical ICD-10 diagnosis categories (Table 2). In 4 studies, the primary clinical diagnosis was OA 2,9,10,12 (ICD-10 code M17.9). In the study by Hubbard, 6 the primary clinical diagnosis was a single medial femoral condyle degenerative chondral lesion; however, not enough information was provided by the author to allow the classification of the degenerative chondral lesion as clinical OA.
Arthroscopic Surgery Outcomes in Randomized Controlled Trials a

a ACR, American College of Rheumatology; APM, arthroscopic partial meniscectomy; AS, arthroscopic surgery; KL, Kellgren-Lawrence; KOOS, Knee Injury and Osteoarthritis Outcome Score; MMT, medial meniscal tear; MRI, magnetic resonance imaging; NS, not stated; OA, osteoarthritis; OM, outcome measure; PROM, patient-reported outcome measure; PT, physical therapy; ROM, range of motion; SF-36, Short Form–36; TKA, total knee arthroplasty; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; WOMET, Western Ontario Meniscal Evaluation Tool.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Inclusion and Exclusion Criteria in Arthroscopic Knee Surgery RCTs Using ICD-10 Codes a

a Osteoarthritis as defined by the American College of Rheumatology. ICD-10, International Classification of Diseases–10th Revision; RCT, randomized controlled trial.
b Does not include nontraumatic osteoarthritis in studies with a primary clinical diagnosis other than osteoarthritis. Diagnoses of conditions external to the knee joint not included.
In 8 studies, the primary clinical diagnosis was a symptomatic degenerative atraumatic medial meniscal tear (MMT) 4,5,7,13 –15,17,18 (ICD-10 code M23.2) in the presence of chondral degeneration of various degrees. In the study by Kettunen et al, 8 the primary clinical diagnosis was patellofemoral pain (ICD-10 code M22.4).
Three RCTs were assessed as having inadequate power for the primary outcome measure. Østerås et al 13 examined arthroscopic partial medial meniscectomy in the presence of knee OA compared to physical therapy. They included a power analysis; however, the final number of patients in their study was less than stated to achieve adequate power. Chang et al 2 lacked a power analysis; however, a post hoc power analysis using G*Power 3 revealed that the study was inadequately powered (power <0.8) to confirm the self-described meaningful improvement of a reduction of >1 cm from the baseline visual analog scale score. Sihvonen et al 14 provided a post hoc subgroup analysis of patients from their original 2013 RCT 15 who suffered self-described mechanical symptoms, defined as catching and clicking excluding locked or recently locked knees. The authors stated that the subgroup analysis was underpowered.
Three studies favored an arthroscopic intervention at final follow-up: 2 OA studies 6,10 and 1 MMT study. 4 The remaining 11 studies reported no outcome difference compared to the control intervention.
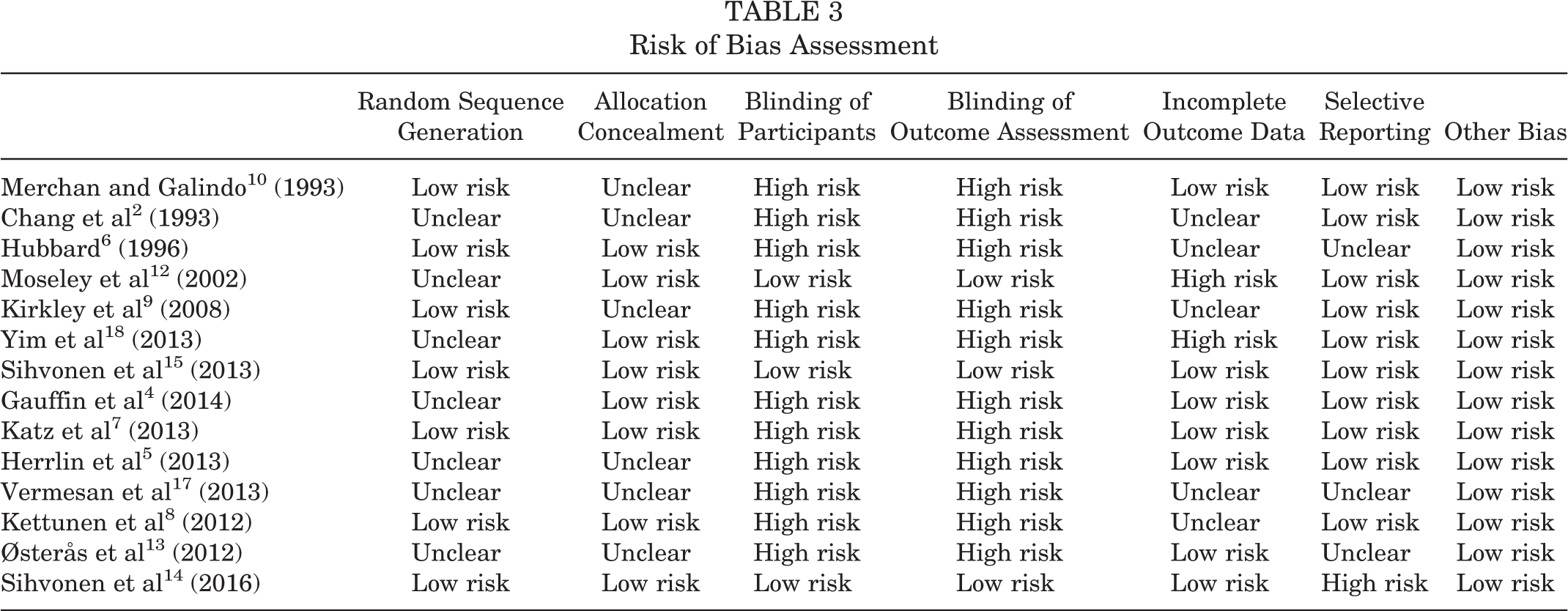
Risk of Bias Assessment
Studies were rated for their risk of bias in Table 3. There were no studies with a low risk of bias in all 7 risk domains assessed in the OA studies and patellofemoral pain studies. 10 In the MMT studies, there was only 1 study with a low risk of bias 15 in all domains.
Risk of Bias Assessment
Exclusion Criteria in MMT Studies
In the 8 studies with a primary clinical diagnosis of an MMT, 5 studies excluded surgeon-assessed locked or locking knees, 4,7,13 –15 and 1 study excluded loose bodies, 5 with Vermesan et al 17 not stating any exclusion criteria (Table 4). The Sihvonen et al 15 (2003) and Sihvonen et al 14 (2016) studies excluded surgeon-assessed locked or recently locked knees and major chondral flaps but included knees with patient-reported catching and locking symptoms. Yim et al 18 and Katz et al 7 also included patients with mechanical symptoms.
Exclusion Criteria in Medial Meniscal Tear Randomized Controlled Trials a

a NS, not stated.
A history of traumatic onset was an exclusion criterion in 6 MMT studies, 5,13 –15,17,18 with Vermesan et al 17 not stating any exclusion criteria. No study included meniscal repair as a management intervention, and meniscal repair was an exclusion criterion in 3 studies. 14,15,18
No study included diagnostic arthroscopic surgery. Inflammatory joint disorders were excluded in 4 studies 9,14,15,18 or were not an inclusion criterion in the remainder.
Exclusion Criteria in OA Studies
Merchan and Galindo 10 excluded patients with pain longer than 6 months, male patients with a weight over 85 kg, female patients weighing greater than 70 kg, instability, or an angular deformity greater than 15°. Hubbard 6 excluded any other intra-articular lesions except for symptomatic medial femoral condyle degenerative lesions in patients with no radiographic OA. Moseley et al 12 added the Kellgren-Lawrence grade for each compartment together, excluding the patients with a score of greater than 9. Kirkley et al 9 excluded patients with large meniscal tears, bucket-handle tears, prior major knee trauma, inflammatory or postinfectious arthritis, deformity >5°, or Kellgren-Lawrence grade 4 in 2 compartments.
Types of MMTs
Only the study by Yim et al 18 described the MMT pattern; the remainder grouped all MMT patterns together as atraumatic degenerative. Sihvonen et al 15 described an atraumatic sudden symptom–onset subgroup that did no better with a surgical intervention.
Crossover Into Surgical Group
None of the OA studies described crossover into the surgical group. Seven of the 9 MMT studies described crossover into the surgical group of 0%, 13 2%, 18 2.5%, 14 6.6%, 15 21.3%, 4 30.2%, 7 and 33.3%. 5 Reasons for crossover into the surgical group were either those of persistent symptoms 4,5,15 or were not given. 7,18 Herrlin et al 5 and Katz et al 7 stated that patients who crossed over into the surgical group had significantly worse symptoms than the remainder of the control group before crossing over but achieved similar outcomes to the control and surgical groups.
Effect of Age
Only 1 study specifically examined the effect of age on outcomes. Gauffin et al 4 reported better outcomes for both rehabilitation and arthroscopic interventions for 55- to 64-year-old patients compared to younger patients aged 45 to 55 years.
Adverse Events
No study described a greater rate of adverse events in the arthroscopic group.
Lateral Meniscal Tears
No study examined outcomes of partial meniscectomy as a treatment for lateral meniscal tears.
Outcomes of Patients With Atraumatic MMTs Who Failed Nonoperative Management
The inclusion criteria for 4 of the 8 MMT studies included the failure of clinician-assessed nonspecific nonoperative management between 1 and 3 months. No MMT study examined the outcomes of patients who had undergone a structured rehabilitation program and continued to have severe self- described symptoms after randomization to an operative versus nonoperative intervention.
Outcomes of Patients Who Self-Reported Mechanical Symptoms
Self-reported mechanical symptoms were common in all studies. One study, 14 a secondary analysis of a previously published RCT, found no difference in patients with atraumatic self-described mechanical symptoms who underwent medial meniscectomy compared to a sham procedure. Kirkley et al 9 found no improvement in a subgroup of patients with OA and self-described mechanical symptoms compared to rehabilitation.
Progression of OA After Partial Meniscectomy
The study by Herrlin et al 5 found no difference in OA progression 5 years after partial medial meniscectomy compared to physical therapy.
Conclusion
All of the OA studies had a high risk of bias in at least 1 domain. One OA study
12
had a low risk of bias from blinding. In this study, patients who were assessed clinically to have moderate to severe knee OA, in the absence of loose bodies or locking, showed no advantage of arthroscopic debridement over lavage or sham surgery. In a study with a high risk of bias,
6
patients with isolated medial femoral condyle degenerative lesions benefited from an arthroscopic intervention compared to rehabilitation. In a study with a high risk of bias,
8
arthroscopic patellofemoral chondroplasty did not benefit patients compared to nonoperative management. In atraumatic MMTs,
15
in the absence of surgeon-assessed locking or locked knees or a repairable meniscal tear, a study with a low risk of bias showed no advantage of arthroscopic partial meniscectomy over sham surgery. In a study with a high risk of bias in 1 domain,
14
in patients with an atraumatic onset of self-described mechanical symptoms, in the presence of an MMT, other than surgeon-assessed recent locking, a locked knee, or symptomatic loose bodies, there was no advantage to arthroscopic partial meniscectomy over sham surgery. The role of arthroscopic surgery in lateral meniscal tears remains uncertain, as it has not been subjected to an RCT. The role of subchondral drilling or microfracture undertaken in combination with osteotomy remains uncertain, as no RCTs exist comparing it to osteotomy alone. Preservation of the medial or lateral meniscus by repair of the body or root, with or without degeneration of the joint, has not been subjected to an RCT. No study investigated the role of diagnostic arthroscopic surgery in situations where MRI was inconclusive or unable to be performed. The value of MRI in the investigation of atraumatic nonlocking knee symptoms in the presence of OA remains uncertain. No MMT study examined the outcomes of patients who failed a structured rehabilitation program by randomization to an operative versus nonoperative intervention.