
Abstract
Background:
The delayed management of patients with shoulder instability may increase the prevalence and severity of concomitant intra-articular shoulder injuries resulting from persistent subluxations and dislocations.
Hypothesis:
Patients with a longer delay from the initial dislocation event to undergoing magnetic resonance imaging (MRI) or magnetic resonance arthrography will demonstrate more subluxations or dislocations and a greater amount of intra-articular shoulder damage.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We performed a retrospective review of 89 patients from a single institution with clinically and radiographically confirmed primary traumatic anterior shoulder dislocations. Patients were divided into 2 groups: those undergoing MRI less than 6 months (n = 44; LT6) or greater than 6 months (n = 45; GT6) from the initial dislocation event. The MRI assessment included evaluation of soft tissue injuries, including the labrum, capsule, rotator cuff, and cartilage damage severity along with bone loss.
Results:
The delayed MRI group (GT6) demonstrated a greater degree of intra-articular abnormalities compared to the early MRI group (LT6). A greater percentage of superior labral anterior-posterior (SLAP) tears (58% vs 34%, respectively) and cartilage damage (73% vs 27%, respectively) was present in the GT6 group compared to the LT6 group. Cartilage damage was 18% mild, 7% moderate, and 2% severe for the LT6 group as compared to 38% mild, 31% moderate, and 4% severe for the GT6 group. Additionally, more recurrent shoulder dislocations were seen in the GT6 group (n = 6) compared to the LT6 group (n = 2). In the LT6 group, there were more rotator cuff tears (50% vs 24%, respectively) and capsular tears (25% vs 9%, respectively) than the GT6 group. There was no difference in anterior glenoid bone loss, glenoid version, or humeral head subluxation between the 2 groups.
Conclusion:
Patients who undergo MRI greater than 6 months from the time of primary or initial shoulder dislocation had significantly more recurrent shoulder instability events and demonstrated a greater incidence and severity of intra-articular abnormalities, including SLAP tears, posterior labral tears, and anterior glenoid cartilage damage.
Keywords
Traumatic anterior shoulder instability is commonly seen in patients secondary to sports or trauma, with a reported incidence of 24 per 100,000 person-years. 24,28,29 Controversy exists regarding the optimal timing for surgical intervention. Younger patients have higher rates of recurrent dislocations and may benefit from acute intervention depending on presenting symptoms, clinical evidence of instability, activity levels, and goals to return to high-demand sports. Conversely, older patients experience lower rates of recurrent shoulder instability with nonoperative treatment after an initial dislocation. Prospective studies comparing operative stabilization to nonoperative treatment favor operative intervention in young, athletic patients to reduce the risk of subluxations or instability recurrence. 2,3,12,13,20,23,30 However, delayed or conservative treatment has also been described as a way to continue in-season play and avoid potentially unnecessary surgery. 8,13
Traditional decision-making treatment algorithms employed in favor of early surgical stabilization consider the risk of recurrent instability in relation to the patient’s age and activity level. Besides the risk of recurrent instability, recurrent shoulder subluxation or dislocation events cause additional damage to the intra-articular structures and increase the risk of the patient developing glenohumeral arthritis. 6,7,16,17,22,36 Therefore, the risk of additional intra-articular glenohumeral structural damage after repeated dislocation events may be a relevant factor and should also be taken into consideration when determining optimal treatment. 9,25 While the development of additional or worsening severity of intra-articular abnormalities is important, it is not known how quickly or to what degree these changes occur after the primary dislocation event.
The purpose of this study was to evaluate whether patients who undergo shoulder magnetic resonance imaging (MRI) later after their initial primary dislocation event will have more intra-articular abnormalities and more subluxation/dislocation events than those who undergo MRI sooner after their initial episode. We hypothesized that a delay in undergoing MRI will result in greater intra-articular damage to both the soft tissue and cartilage.
Methods
Our institutional review board approved this study. The orthopaedic departmental billing database was queried for International Classification of Diseases, 9th Revision (ICD-9) codes 831.00 (closed dislocation of the shoulder) and 831.01 (closed anterior dislocation of the humerus) from 1999 through 2013 to identify all patients ≥18 years of age who were treated for a primary traumatic anterior shoulder dislocation and had available MRI or magnetic resonance arthrography (MRA) scans of the involved shoulder. A retrospective chart review was performed for the initial dislocation event date, patient age, mechanism of injury, and number of subsequent dislocations or subluxations. Patients were excluded if they presented with multidirectional instability or posterior shoulder instability or lacked one of the following criteria: clinical documentation of the exact initial dislocation date, clinical and radiographic documentation of a shoulder dislocation, number of recurrent shoulder subluxations or dislocations, and adequate clinical follow-up.
Patients were stratified into 2 groups: MRI less than 6 months (LT6) or greater than 6 months (GT6) from the initial documented anterior shoulder dislocation event. The reasons that we used 6 months as the cutoff time point for the 2 groups were as follows: (1) After applying the inclusion and exclusion criteria to our data, we narrowed the total group down to 89 patients from the original 255 patients who were screened. Using the 6-month time point from the initial dislocation event to MRI provided us with 2 groups that were evenly distributed. (2) Most patients seen by our primary care provider with a first-time dislocation event may receive 3 to 6 months of physical therapy before MRI. Thus, using the 6-month time point was reasonable to separate the groups.
A musculoskeletal radiologist and a fellowship-trained orthopaedic surgeon (A.M.M. and X.L.) independently reviewed all shoulder MRI scans for intra-articular abnormalities; both reviewers were blinded to the patient and the initial time of dislocation. A consensus was achieved with another musculoskeletal radiologist when a difference in radiographic scoring existed between the 2 reviewers. The following abnormalities were documented: bone marrow edema, Hill-Sachs lesion (size and location) (Figure 1), soft tissue Bankart lesion (Figures 2 and 3), bony Bankart lesion (Figures 4 and 5), superior labral anterior-posterior (SLAP) tear (Figure 6), posterior labral tear (Figure 7), biceps injury, rotator cuff tear, and capsular rupture.

Hill-Sachs lesion (arrow) on an axial proton density sequence.

Soft tissue Bankart lesion with a tear of the anterior inferior labrum and an adjacent, small, full-thickness mild (<25%) chondral defect over the anterior inferior glenoid (arrow) on an axial proton density sequence.

(A) Soft tissue Bankart lesion with a mildly displaced tear of the anterior inferior labrum as well as focal stripping of the periosteum (arrowhead) and a posterior labral tear (arrow) on an axial proton density sequence. (B) Normal bony morphology of the glenoid on a sagittal T1 sequence using the surface area method.
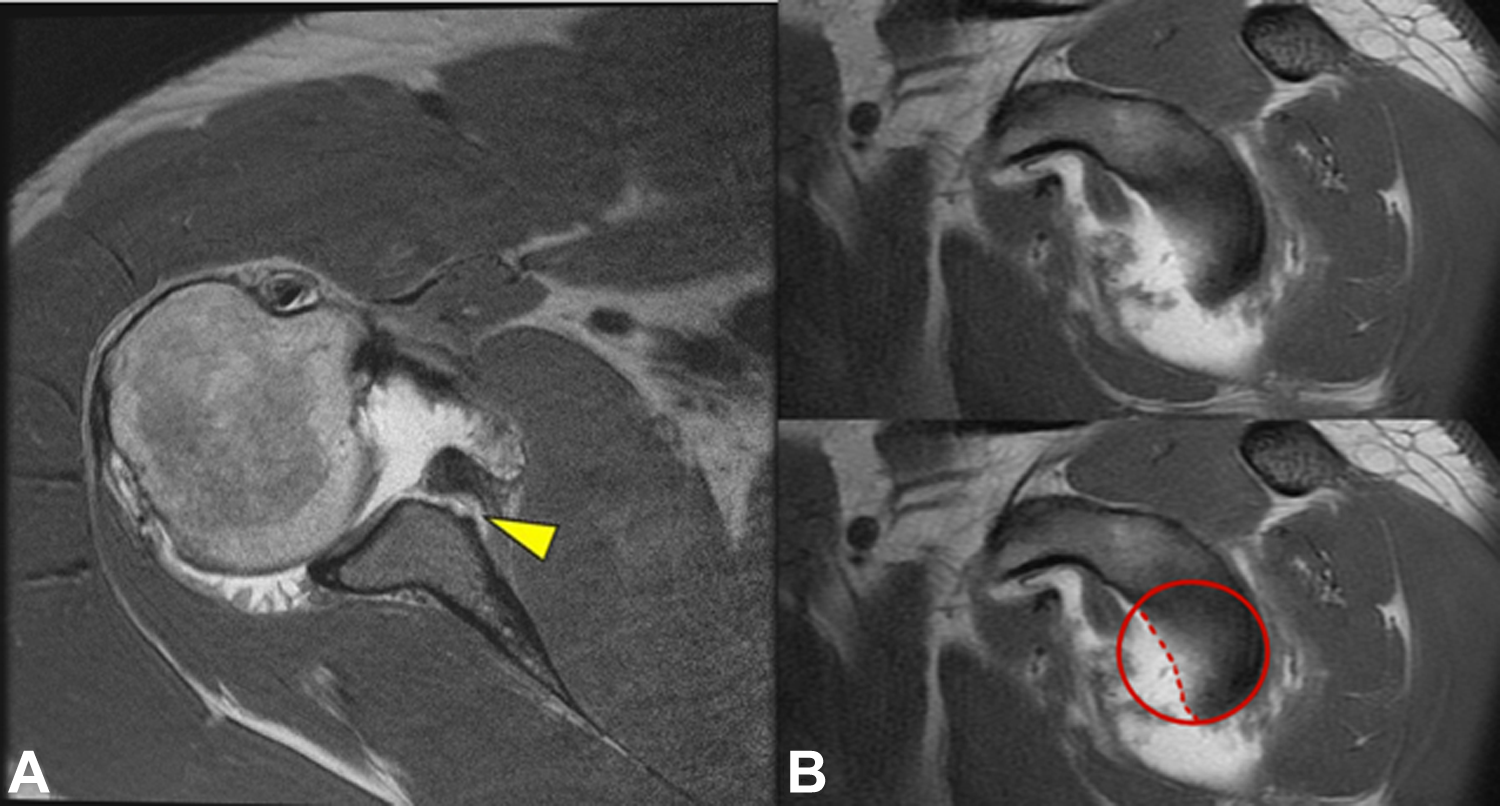
(A) Bony Bankart lesion with a large displaced fragment of the anterior inferior glenoid (arrowhead) on an axial proton density sequence. (B) Quantification of the size of the bony defect on a sagittal T1 sequence using the surface area method; the defect encompasses nearly 30% of the articular surface of the glenoid.

Bony Bankart lesion with a large displaced fragment of the anterior inferior glenoid (arrow) on an axial proton density sequence. Localized chondral delamination along the margins of the defect (arrowhead).

Tear of the superior labrum (arrowhead) on a coronal T1 fat-saturated sequence (magnetic resonance arthrography).

Macerated anterior inferior labrum with an adjacent full-thickness chondral defect over the anterior inferior glenoid (arrow) and a posterior labral tear (arrowhead) on an axial proton density sequence.
Glenoid bone loss was recorded and measured on sagittal T1-weighted MRI with the surface area method. 32,33 Cartilage damage on both the glenoid and humeral head was documented and graded as mild, moderate, or severe. The evaluation of cartilage damage on the glenoid was performed using the axial cut at the middle of the glenoid and counting the total number of MRI slices from the top of the glenoid to the bottom, then dividing this number by 2. This method is reproducible and will always obtain the axial image to the middle of the glenoid for the evaluation of cartilage damage. The full diameter of the glenoid was then measured on this axial image in the middle of the glenoid.
The amount of cartilage loss was determined relative to the glenoid diameter. A categorical distinction of cartilage damage based on axial proton density, T1 fat-saturated, or T2 fat-saturated MRI sequences was used, with mild damage corresponding to partial- or full-thickness cartilage defect involving <25% of the diameter of the glenoid. Moderate cartilage damage corresponded to full-thickness cartilage defect involving between 25% and 50% of the glenoid diameter, and severe cartilage damage corresponded to full-thickness cartilage defect involving >50% of the diameter of the glenoid. Additionally, glenoid version, as described by Friedman et al, 11 as well as the percentage of humeral head subluxation was measured. 21,34 Humeral head subluxation was determined using the adapted subluxation index by Walch et al, 35 with posterior subluxation defined as >55% and anterior subluxation defined as <45%.
Statistical analysis was performed with SPSS (IBM Corp). The Student t test was used for parametric data, and the chi-square test was used for categorical data.
Results
A total of 89 patients met our inclusion criteria (255 patients screened), with 44 in the LT6 group and 45 in the GT6 group (Table 1). In the LT6 group, of the 44 scans, 32 were MRI and 12 were MRA. In the GT6 group, of the 45 scans, 28 were MRI and 17 were MRA.
Patient Demographics a

a Values are reported as mean ± SD unless otherwise specified. GT6, MRI greater than 6 months; LT6, MRI less than 6 months; MRA, magnetic resonance arthrography; MRI, magnetic resonance imaging.
Demographic differences between the LT6 and GT6 groups included age (39.4 vs 29.9 years, respectively; P < .05) and number of total dislocation events (1.9 vs 5.9, respectively; P < .0001). Sex distribution was similar between the 2 groups (84% vs 80% male, respectively; P = .615). Sports injuries were responsible for 25% (11/44) of the injuries in the LT6 group and 51% (23/45) of the injuries in the GT6 group. The remaining dislocations occurred as a result of a mechanical fall, physical altercation, or motor vehicle accident.
Patients in the LT6 group underwent MRI a mean 2.0 ± 1.8 months after the initial dislocation, while those in the GT6 group underwent MRI a mean 54.8 ± 46.6 months after the initial dislocation (P < .0001). On MRI, there was less cartilage damage in the LT6 group compared to the GT6 group (27% vs 73%, respectively; P = .0002) (Table 2). Cartilage damage was 18% mild, 7% moderate, and 2% severe for the LT6 group as compared to 38% mild, 31% moderate, and 4% severe for the GT6 group (P < .0001) (Figure 8).
Associated Abnormalities on MRI a

a Values are reported as n (%). GT6, MRI greater than 6 months; LT6, MRI less than 6 months; MRI, magnetic resonance imaging; SLAP, superior labral anterior-posterior.

Degree of cartilage damage seen in the LT6 (magnetic resonance imaging [MRI] less than 6 months) versus GT6 (MRI greater than 6 months) group.
There were significantly fewer associated SLAP tears (34% vs 58%, respectively; P = .025) in the LT6 group compared to the GT6 group. Bone marrow edema was present in 68% of the LT6 group and 11% of the GT6 group (P < .0001). Additionally, rotator cuff tears were present in 50% of the LT6 group and 24% of the GT6 group (P = .021).
There was no significant difference between the LT6 and GT6 groups for the presence of posterior labral tears (7% vs 22%, respectively; P = .069), Hill-Sachs lesions (77% vs 87%, respectively; P = .249), Bankart lesions (55% vs 56%, respectively; P = .924), bony Bankart lesions (36% vs 33%, respectively; P = .764), long head of the biceps tendon lesions (18% vs 7%, respectively; P = .118), capsular lesions (25% vs 9%, respectively; P = .051), posterior humeral head subluxations (36% vs 40%, respectively; P = .724), glenoid bone loss (39% vs 40%, respectively; P = .895), or glenoid version (–5.3% ± 4.4% vs –4.5% ± 3.6%, respectively; P = .395). Among patients with glenoid bone loss, there was no quantitative difference between the 2 groups (8% vs 7%, respectively). Subscapularis tendon tears were seen in 16% versus 4% of patients in the LT6 and GT6 groups, respectively (P = .098).
Discussion
The results from this study show that the progression of intra-articular shoulder abnormalities (cartilage loss and labral tears) after a primary shoulder dislocation event is correlated with time and number of recurrent subluxations or dislocations. In this study, patients who underwent MRI greater than 6 months after the primary dislocation event had a 3-fold increase in the incidence of cartilage damage and twice as many SLAP tears as compared to patients evaluated with MRI within 6 months of the primary dislocation event. However, with regard to Hill-Sachs, Bankart, bony Bankart, and long head of the biceps lesions as well as glenoid bone loss, we did not find a significant difference between the 2 groups, which suggests that the majority of these abnormalities can be attributed to the initial damage experienced as a result of the inciting traumatic dislocation event, without remarkable progression based on time or number of recurrences. The initial dislocation event appears to alter the biomechanical load sharing and translational forces of the glenohumeral joint to allow significant continuous progression of intra-articular cartilage and labral damage without notable progression in the abnormalities of other associated static and dynamic stabilizers, as detected via MRI in our study. These findings suggest the need for prompt MRI or MRA evaluations in patients who are at a higher risk for recurrent instability (younger age, male, contact sports, and shoulder hyperlaxity). These patients may benefit from early stabilization surgery to prevent recurrent instability, which leads to further intra-articular damage to the shoulder.
Patients who underwent MRI greater than 6 months after injury were nearly twice as likely to exhibit a SLAP lesion as compared to those who underwent MRI less than 6 months from the primary dislocation event (58% vs 34%). P value stated in the Results section and in Table 2. Among the 44 patients in the LT6 group, we found 27% had associated cartilage damage, which was significantly less compared to the GT6 group (73% with cartilage damage). Additionally, in the subset of patients who waited longer than 6 months to undergo MRI, there were significantly higher grades of cartilage damage as compared to the LT6 group. Recurrent shoulder instability may cause eccentric loading, leading to secondary damage to the superior or posterior labral structures and cartilage over time. 1,31 Gutierrez et al 16 compared the frequency of lesions associated with traumatic shoulder dislocations in patients with primary and recurrent instability. They also reported a higher rate of SLAP lesions along with more posterior labral tears and rotator cuff abnormalities in the recurrent group.
Hovelius and Saeboe 18 reviewed the radiographs of 223 nonoperatively treated patients for 25 years to evaluate the progression of arthropathy in posttraumatic anterior shoulder dislocations. They found a higher presence of moderate to severe shoulder arthropathy in patients with recurrence (39%) or those who were surgically treated (26%) compared to patients with no recurrence of instability (18%). Buscayret et al 5 reported that the preoperative incidence of arthritis was 9.2% compared to the postoperative incidence of 19.7% after anterior shoulder stabilization surgery. Franceschi et al 10 also reported a 21.8% incidence rate of postoperative arthritis in patients after surgery for anterior instability. Both studies found that older age at the time of injury, increased time from the initial dislocation to surgery, and increased number of preoperative dislocations were risk factors for developing glenohumeral arthritis. 5,10 Yiannakopoulos et al 36 reported similar findings in their review of arthroscopic images, in that associated secondary intra-articular lesions were more frequently encountered in patients with chronic shoulder dislocations compared to acute dislocations, which is likely related to the repeated dislocation or subluxation episodes. Our data suggest that early imaging (MRI or MRA within 6 months of the primary dislocation event) of high-risk patients after anterior shoulder instability and appropriate surgical stabilization to prevent further glenohumeral damage might mitigate the risk of progressive labral tears and cartilage degeneration over time.
Landmark studies by Burkhart and De Beer, 4 Itoi et al, 19 and Sugaya et al 33 that linked progressive glenoid bone loss to the failure of soft tissue stabilization surgery did not comment on the timing of the primary dislocation event in relation to the date of initial imaging or the effect of the number of subluxations or dislocations on glenoid bone loss. Our study did not demonstrate a significant difference with respect to the occurrence of osseous Bankart lesions, Hill-Sachs lesions, or glenoid bone loss on MRI between the early and delayed imaging groups. Griffith et al 15 reported variable flattening of the anterior glenoid curvature in 91% (42/46) of anterior dislocated shoulders compared to only 4% (2/54) observed in normal shoulders. They found an exponential relationship between the degree of anterior glenoid flattening and the number of dislocations sustained; however, they did not find a linear relationship between the 2 factors. The authors attributed this finding to the possibility that the first few dislocation events had a relative greater impact in the degree of flattening or bone loss as compared to the subsequent dislocations. This is similar to the results of our study in that the cumulative increase in intra-articular cartilage loss and labral tears in the absence of notable differences in the amount of anterior glenoid bone loss between the 2 groups suggests that the initial dislocation event was the major contributor to glenoid bone loss, whereas the subsequent recurrent subluxations and dislocations contributed more to glenoid cartilage damage and labral tears. Additionally, we found no difference in glenoid version or humeral head subluxations between these 2 groups, which suggests that static glenoid morphology did not play a role in the differences in the tear rate and the severity of cartilage damage.
Interestingly, we found a significant difference with respect to patient age and timing of MRI. The mean age of the LT6 group was 40 years as compared to 30 years for those in the GT6 group (P < .05). Further, the LT6 group had more rotator cuff tears (50%) than the GT6 group (24%). This difference in the incidence of rotator cuff tears may be explained by the differences in the ages between the 2 groups, as older patients tend to tear their rotator cuff more than younger patients. Neviaser et al 26,27 published the results of 11 patients over the age of 40 years who had recurrent instability secondary to rotator cuff abnormalities. Similarly, a systematic review by Gombera and Sekiya 14 evaluated all studies from 1950 to 2012 and found that patients older than 40 years were more likely to sustain a concomitant rotator cuff tear during a traumatic shoulder dislocation event compared to younger patients. Given the high incidence of rotator cuff tears in older patients after the initial dislocation event, prompt MRI or MRA should be considered in all older patients who present with clinical evidence of rotator cuff weakness after a dislocation. Another explanation of the age difference is related to selection bias, as this study was retrospective in nature. However, the injury findings are not all accounted for by age-related changes that one would expect in an older cohort rather than a younger cohort. In other words, if the older cohort demonstrated more severe associated abnormalities than the younger cohort, then one could argue that the difference was primarily age related and not injury related, but the opposite findings were found in this study between the 2 groups.
Several limitations are inherent to this retrospective study. First, this was not a randomized study, and this likely led to selection bias in the 2 patient groups. The LT6 group had older patients compared to the GT6 group, and this would explain the higher percentage of rotator cuff tears seen after anterior dislocation in the LT6 group. Furthermore, the causes for anterior shoulder dislocations ranged from sports to motor vehicle accidents to high-energy trauma, which may have also produced bias between the 2 groups. There are also many factors contributing to whether a patient undergoes MRI after a shoulder dislocation event, including socioeconomic factors, health insurance status, physician treatment bias, and patient bias. Another limitation to this study is that some patients underwent noncontrast MRI while others underwent MRA. Using MRI to detect labral tears may result in decreased sensitivity compared to MRI with an intra-articular arthrogram. Furthermore, we did not assess for both intraobserver and interobserver reliability. A significant strength of this study is that the patient population consisted of a cohort treated at a single institution, thus limiting variability in management and imaging and mitigating some of the inherent bias.
Thus, a prospective randomized study is needed to better separate and control preoperative demographic factors while prospectively performing serial MRI or MRA in these patients with anterior shoulder dislocations. Such a study could document both the progression of intra-articular shoulder lesions and track functional outcomes as they correlate with the number of preoperative recurrent instability events and time to MRI.
Conclusion
Patients who waited more than 6 months from the time of primary shoulder dislocation to undergo MRI had an increased risk of SLAP tears, posterior labral tears, and anterior glenoid cartilage damage. These findings suggest that even in the absence of a subsequent dislocation event, recurrent shoulder subluxations may be responsible for the progression of intra-articular damage over time. This information provides additional evidence of disease progression and is valuable for counseling patients about nonsurgical versus surgical treatment options after a primary shoulder dislocation. Thus, in the higher risk patient population (younger age, male, contact sports, or shoulder hyperlaxity), prompt MRI or MRA should be performed to help better counsel patients regarding the benefit of early shoulder stabilization surgery as an option to decrease the risk of recurrence and associated intra-articular glenohumeral lesions.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: X.L. is a paid consultant for Mitek and Tornier and has equity in the Journal of Medical Insight.
Ethical approval for this study was obtained from Boston University Medical Campus/Boston Medical Center institutional review board (protocol No. H-33007).