
Abstract
Background:
Labral tears confirmed by magnetic resonance imaging (MRI) are a relatively common injury among collegiate athletes and can influence a player’s ability to compete at the professional level.
Purpose:
To determine the prevalence of MRI-confirmed shoulder labral injuries in collegiate football players entering the National Football League (NFL) Combine and to further describe these injuries by tear location, player position, history of surgical intervention, and associated concomitant shoulder injuries.
Study Design:
Descriptive epidemiology study.
Methods:
Data from 2009 to 2015 were retrospectively collected through review of the injury data registry available to the medical and training staff of all NFL teams following the completion of the NFL Combine. After players with potential labral tears were identified through history and examination, their MRIs were reviewed by 2 fellowship-trained orthopaedic sports medicine surgeons. Players diagnosed with a labral tear confirmed by MRI were separated for further analysis.
Results:
A total of 2285 players were analyzed for the presence of labral tears at the NFL Combine. Overall, 377 shoulders (in 340/2285 players; 14.9%) demonstrated MRI evidence of labral tear; whereas linebackers had the highest rate of labral tear (19.2%), linemen had significantly higher risk for labral injury in at least 1 shoulder (odds ratio, 1.31; 95% CI, 1.02-1.67; P = .029) compared with nonlinemen. Of the 377 shoulders analyzed, 115 (30.5%) exhibited an anterior labral tear, 131 (34.7%) had a posterior labral tear, and 131 (34.7%) had combined anterior and posterior tears. One hundred twenty (31.8%) shoulders had superior labral anterior-posterior (SLAP) tears. A total of 203 (53.8%) shoulders demonstrated evidence of previous surgical intervention on imaging.
Conclusion:
Injury involving the labrum is relatively common among participants at the NFL Combine, especially linebackers and linemen. Further investigation is necessary to determine the impact these injuries have on player draft position and NFL performance.
Keywords
Labral tears confirmed by magnetic resonance imaging (MRI) are a relatively common injury among collegiate athletes and can influence a player’s ability to compete at the professional level. Shoulder instability events in athletes, which commonly cause a shoulder labral tear, reportedly occur at a rate of 0.12 per 1000 exposures. 11 Athletes in contact and collision sports have a higher risk of shoulder instability because of exposure to repeated traumatic loads on the shoulder. 1 In rugby, for example, the shoulder has been reported to be the third most common site of injury. 4 Yet the prevalence of injuries to the glenoid labrum in football has not been well documented in the literature, particularly in the context of football players entering the National Football League (NFL) Scouting Combine in an attempt to make a professional NFL roster. An understanding of the prevalence of labral tears has financial implications, as labral tears may negatively affect player draft order, which in turn lowers the value of the drafted player’s first contract. To date, limited epidemiological data are available in this specific patient population.
In addition to studying the prevalence of labral tears, studying the pathoanatomic characteristics of labral tears based on anatomic location and their association with football player position may be important. Such study may also assist with musculoskeletal evaluation and assessment, as anterior, posterior, and combined anterior and posterior labral tears may represent different mechanisms of injury, different spectrums of symptoms, and different effects on performance.
The NFL Scouting Combine is a weeklong showcase where collegiate football players are tested and evaluated. Because thorough injury evaluations are conducted by skilled medical teams, with supplemental imaging, the event provides a unique opportunity to collect and analyze injury data among an elite, high-demand athlete population. This study therefore aimed to characterize the epidemiological characteristics of labral tears, including anterior tears, posterior tears, combined anterior and posterior labral tears, and superior labral anterior-posterior (SLAP) tears, in elite football players by analyzing the records of NFL Combine participants. We hypothesized that certain tear patterns would be more prevalent in certain player positions due to the repetitive movements exerted during play, the loads to which the shoulder is subjected, and position-specific training. We also hypothesized that linemen, both offensive and defensive, would have a higher incidence of posterior labral tears because of the at-risk shoulder orientation that their position requires, whereas SLAP tears would be more prevalent in quarterbacks owing to the overhead throwing motion of their position. Anterior labral tears were hypothesized to be more prevalent in wide receivers, tight ends, and other skill positions in which the player uses the arm in a more outstretched position, which increases the risk of traumatic anterior dislocation during tackling, collisions, or forceful landing.
Methods
The medical records of 2285 players participating in the NFL Combine from 2009 to 2015 were evaluated retrospectively. All participants were entered into our study, and their records were deidentified in order to preserve protected health information privacy. A flow chart depicting our player selection process is provided in Figure 1.

Flow chart depicting player selection process for study population. MRI, magnetic resonance imaging.
At the combine, the medical staff of each of the 32 NFL teams performed their respective musculoskeletal evaluations of each player, and a comprehensive orthopaedic note was dictated after examination of the athletes. Each NFL team has an opportunity to review the National Collegiate Athletic Association (NCAA) Injury Surveillance Program and evaluate the player, and each player is subsequently evaluated by a group of doctors from several NFL teams. A physician from every NFL team has the opportunity to order imaging based on the player’s injury history and physical examination findings. All injury data were collected through review of the injury data registry available to the medical and training staff of all NFL teams after the completion of the NFL Combine.
For the purposes of this study, each record was searched specifically for shoulder injuries potentially involving the labrum, rotator cuff, biceps, clavicle, acromioclavicular joint, or sternoclavicular joint. Exclusion criteria included players without a history of shoulder injury, those with incomplete imaging, and those without evidence of a labral injury on imaging review performed by a fellowship-trained orthopaedic sports medicine surgeon.
Shoulder Labrum MRI Evaluation
After players with potential labral tears were identified based on the NFL Combine medical evaluation, Siemens 3.0-T MRIs performed with standardized shoulder protocol and dedicated shoulder coil were retrospectively reviewed by 2 fellowship-trained orthopaedic sports medicine surgeons (S.M., S.J.F.), and these interpretations were corroborated with the assessment of a musculoskeletal radiologist to develop a consensus on the characteristics of each tear. Any discrepancies between the two orthopaedic surgeons were ruled on by the musculoskeletal radiologist, and that decision was final. Multiple views and formats of the shoulder MRIs were viewed on a standard picture archiving and communication system (PACS) and analyzed for tear location and size, evidence of previous surgery, number of anchors used, anchor size and location, signs of chondromalacia (graded via Samilson-Prieto classification 15 ), and associated lesions, including anterior labroligamentous periosteal sleeve avulsion, posterior labral periosteal sleeve avulsion, glenoid bone loss, humeral avulsion of the glenohumeral ligament, Hill-Sachs lesion, rotator cuff tear, and biceps injury. Because sublabral foramen variants are normal variants, they were not considered labral tears. The convention of the 12-o’clock position being superior, the 3-o’clock position being anterior, the 6-o’clock position being inferior, and the 9-o’clock position being posterior was adapted regardless of whether the right or left shoulder was involved (Figure 2). All tears involving 12- to 6-o’clock were considered anterior tears, while all tears involving 6- to 12-o’clock were considered posterior tears. Any tears that crossed 6- or 12-o’clock were considered combined anterior and posterior tears. All SLAP tears were also considered combined anterior and posterior tears. The size of the labral tear was estimated by using the face of the clock to identify the start and end positions of the tear, then converting their difference into degrees.

Right and left glenoid depicting clockface location convention.
Players with a labral tear confirmed by MRI were separated for further analysis. Demographic data including age, injury date, side affected, and position were recorded. Players with bilateral labral tears were noted, and the data for the contralateral shoulders were initially removed from the analyses. The prevalence of labral injury was then analyzed by position, and the data were further stratified to compare the prevalence of labral tears in linemen versus nonlinemen. “Linemen” included both offensive and defensive linemen but did not include tight ends or long snappers; “nonlinemen” included all other positions. For the remainder of our analysis, we considered all shoulders with MRI-confirmed labral tears, meaning that both shoulders in individuals with bilateral tears were included. We compared the rates of anterior versus posterior tears among all shoulders with labral injuries and then stratified these data between position groups. Next, we analyzed the rates of previous surgery, as determined by MRI, among all shoulders with labral tears and classified the results by playing position and by the anatomic location of the labral tear. Previous shoulder surgery was defined by evidence of previous operative intervention on MRI (anchors, hardware, grafts, etc) and included successful, healed surgeries. For shoulders that had undergone previous surgery, we studied the number of anchors used in the repair across all players and then compared these data specifically for linemen versus nonlinemen.
Statistical Analysis
The statistical software R was used for all analyses (R Foundation for Statistical Computing). Basic descriptive statistics were analyzed by use of mean, range, SD, CI, and percentage. Fisher exact tests in combination with odds ratio and CI assessment were used to determine statistical significance between positions in subanalysis. Statistical significance was determined by P < .05.
Results
A total of 340 players (14.9%) of the 2285 players at the NFL Combine demonstrated MRI evidence of labral tears in the study years 2009 to 2015. Of the 340 players, 37 (10.9%) had bilateral labral tears, for a total of 377 shoulders included for analysis. Participants with bilateral labral tears represented 1.6% of all combine participants and 10.9% of the participants with MRI-confirmed labral tears. On average, the size of the labral tear was 131.1°. The most common associated injury was a Hill-Sachs lesion, followed by SLAP tears. Imaging findings are detailed in Table 1.
Imaging Findings in Players With Labral Injury at the NFL Combine a

a Percentages are based on number of shoulders unless noted. MRI, magnetic resonance imaging; NFL, National Football League.
b Some shoulders had more than one additional injury, so the values for specific types of injury total more than 315.
Although linebackers had the highest overall rate of labral tears among positions with at least 10 players analyzed, linemen had significantly higher risk for labral tear in at least 1 shoulder (odds ratio, 1.31; 95% CI, 1.02-1.67; P = .029) compared with nonlinemen (Fisher exact test). The rate of labral tears was higher in linemen (17.2%; 95% CI, 14.6%-20.1%) compared with nonlinemen (13.7%; 95% CI, 12.0%-15.5%). An assessment of labral tears by player position is displayed in Table 2.
Overall Prevalence of Labral Tears by Player Position Group a

a MRI, magnetic resonance imaging.
Tear location (anterior, posterior, combined) was further analyzed and characterized based on player position. The rates of anterior tears seen in various positions are shown in Table 3. Of the 377 shoulders with a labral tear, 246 (65.3%) were found to have an anterior shoulder labral tear, of which 131 (53.3%) were combined anterior and posterior tears. Of those combine participants with labral tears who underwent MRI, defensive backs had the highest prevalence of anterior shoulder labral tears at 83.6% (61/73 shoulders), aside from kickers/punters, who had a 100% prevalence (4/4 shoulders). Offensive linemen had the lowest prevalence of anterior labral tears at 53.3% (40/75 shoulders), aside from long snappers, who had 0% prevalence (0/2 shoulders).
Prevalence of Anterior Labral Tears by Player Position Group a
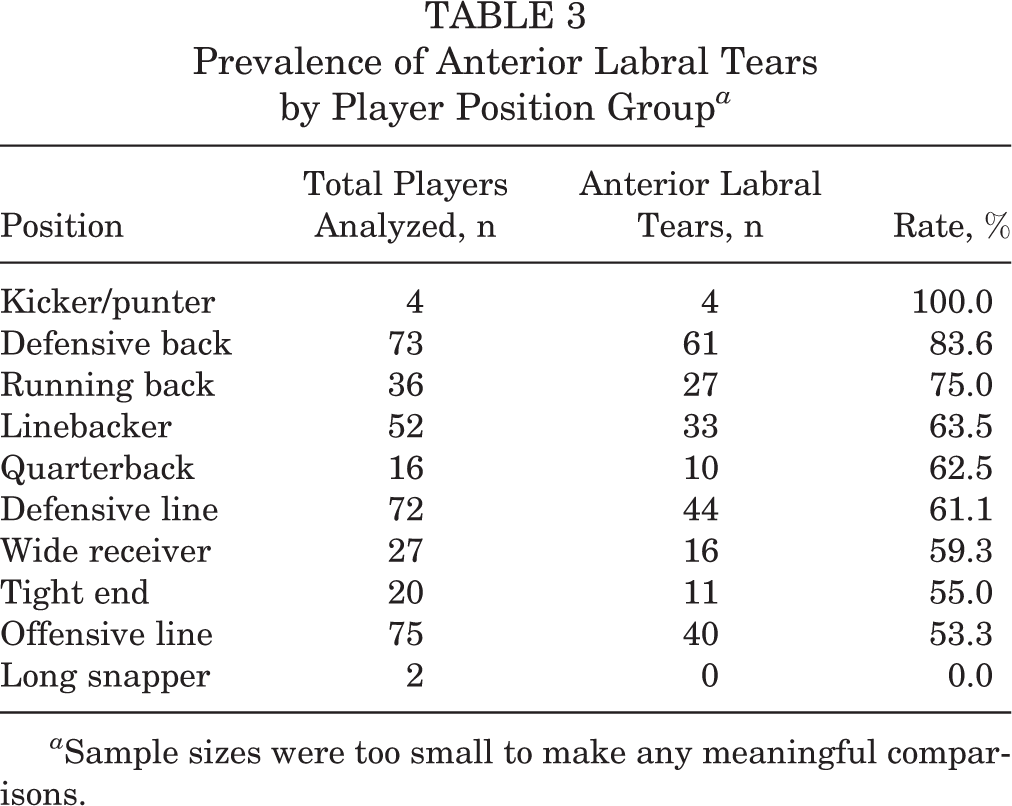
a Sample sizes were too small to make any meaningful comparisons.
Among those combine participants with labral tears who underwent MRI, the prevalence of posterior tears by player position is shown in Table 4. Of the 377 shoulders analyzed, 262 (69.5%) demonstrated a posterior shoulder labral tear, of which 131 (50.0%) were combined anterior and posterior tears. The prevalence of posterior labral tears by position in our cohort ranged from 50% to 100%. We noted a high rate of posterior labral tears among tight ends (80.0%; 16/20 shoulders), offensive linemen (80.0%; 60/75 shoulders), and wide receivers (77.8%; 21/27 shoulders). All long snappers in our series demonstrated posterior labral tears (2/2 shoulders; 100%), although there were relatively few players at that position. Kickers/punters had the lowest rate of posterior tears at 50% (2/4 shoulders), although this position also had relatively few players.
Prevalence of Posterior Labral Tears by Player Position Group a
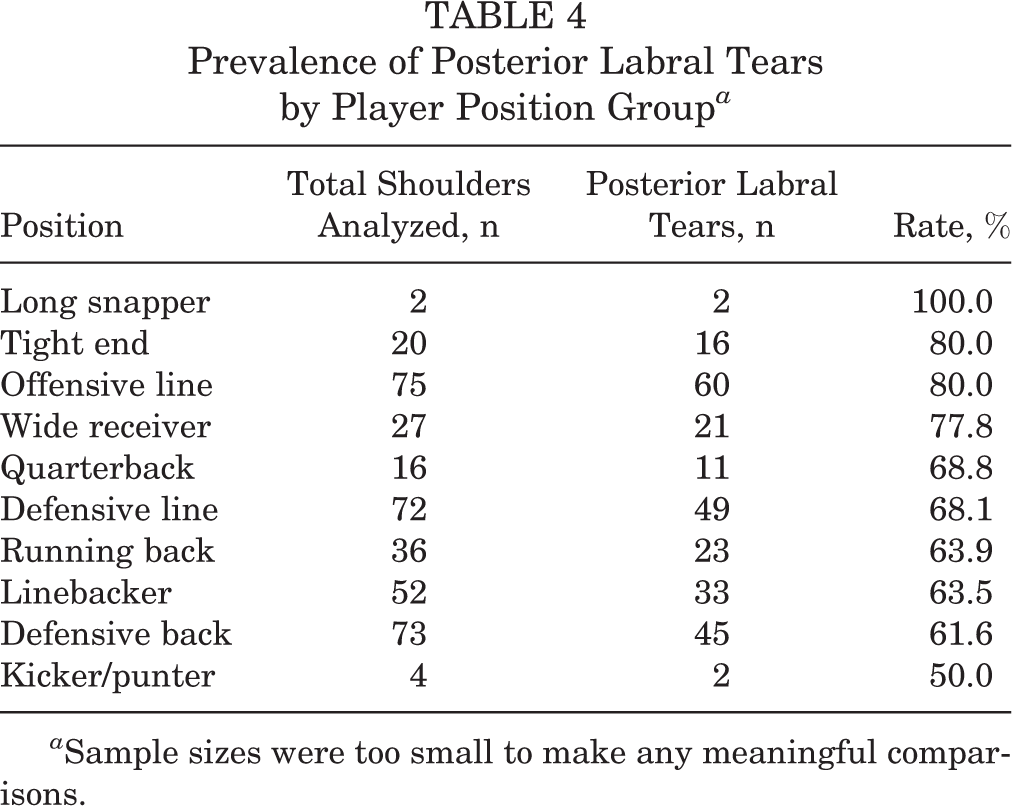
a Sample sizes were too small to make any meaningful comparisons.
Table 5 shows the prevalence of SLAP tears by player position among players with MRI-confirmed labral tears. Of the 377 shoulders analyzed, 120 (31.8%) showed evidence of a SLAP tear. Compared with anterior and posterior labral tears (Tables 3 and 4), SLAP tears were less frequent, but they were still not uncommon. The prevalence of SLAP tears by position in our cohort was 0% to 50%. SLAP tears were seen in 31.2% (5/16 shoulders) of quarterbacks.
Prevalence of SLAP Tears by Player Position Group a

a Sample sizes were too small to make any meaningful comparisons. SLAP, superior labral anterior-posterior.
Numerous players entering the NFL Combine had imaging evidence of previous surgical intervention to address labral injury. The number of previous surgeries performed in our cohort of MRI-assessed labral tears in the NFL Combine is shown by position in Table 6. Of the 377 shoulders analyzed, 203 (53.8%) had a previous surgical intervention. Of these 203 shoulders with evidence of surgical intervention, an average of 3.89 anchors were used in their surgery. The prevalence of previous shoulder stabilization surgery in our cohort ranged between 43.1% and 100%, based on position.
Rates of Imaging Evidence of Previous Surgical Intervention to Address Labral Injury by Player Position Group a

a Sample sizes were too small to make any meaningful comparisons.
Discussion
This study presents the prevalence of labral injuries in elite collegiate football players among those who underwent MRI, the variation of shoulder labral injury rate among different position groups, and the frequencies of labral lesion location. By position, linebackers had the highest rate of labral injury overall, and linemen had a higher risk and rate of labral injuries than did nonlinemen.
Our cohort included 340 players (14.9%) with MRI-confirmed labral injuries, which is similar to the 14.9% prevalence of instability and confirmed SLAP tears reported at the 2004 NFL Combine. 8 These figures represent a much lower rate of labral injury when compared with other overhead sports. In 2009, Lajtai et al 9 found MRI-confirmed labral tears in 24% of professional volleyball players. In a study published in 1985, Andrews et al 2 studied an athletic cohort and found that 73 of 120 patients who underwent shoulder arthroscopy were overhead athletes; 51 of these 73 players were baseball players, while only 6 were football players.
In terms of the pathoanatomic features of the labral tears that were encountered, 65.3% of tears involved the anterior labrum, while 69.5% of tears involved the posterior labrum. Many of the labral tears were combined and had components of both anterior and posterior involvement; of the 377 shoulders with MRI-confirmed labral tears, 131 (34.7%) demonstrated combined anterior and posterior tears.
Additionally, 120 (31.8%) of the 377 labral injuries were considered a SLAP lesion, which made up 10.3% of the 1160 players at the NFL Combine who were identified as having shoulder injuries. This is much higher than the reported rate of 2.2% at the 2004 combine, 8 although the authors of that report did not detail their diagnostic methods and may have defined these injuries more strictly than we did. Weber et al 17 found that SLAP repairs made up 9.4% of all shoulder cases in the American Board of Orthopaedic Surgery database, a figure comparable with our findings. Those authors 17 speculated that increased recognition and technical ability to repair SLAP tears may have led to the increase when compared with the original description of the injury by Snyder et al. 16 Compared with other collision sports, football appears to have a much lower frequency of SLAP lesions. For example, in rugby, 35% of all shoulder injuries were SLAP tears, more than 3-fold that seen in our study. 7 This discrepancy may be related to the fact that noncontrast MRI, as used in our study, is not considered the gold standard for diagnosing SLAP tears. 3,6
Although anterior shoulder instability is not always necessarily associated with a labral tear, it is worth mentioning that anterior instability was responsible for 20.9% of shoulder abnormalities at the 2004 NFL Combine, 8 while posterior instability made up only 4% of all shoulder injuries. Posterior instability was much less common in their study 8 and posterior labral tears were substantially more common in our study, despite a nearly identical cohort in both studies. This finding likely represents the increased understanding and awareness of posterior instability that have developed over the past decade and is consistent with other studies that demonstrate increased rates of posterior labral injuries compared with earlier studies. 12 –14
In our analysis of labral injury by each football player position group, we found that the frequency and location of labral injuries had certain patterns. These patterns may be useful when evaluating football players with shoulder injuries. For example, linemen and linebackers had the highest rates of labral injury in our cohort. Dick et al 5 reported similar anecdotal findings in their 16-year study on collegiate football players; the authors stated that they had seen more shoulder injuries in linemen, likely due to the blocking techniques that involve punching and blocking with the arms forward flexed, adducted, and internally rotated. In contrast, Kaplan et al, 8 in their study on 2004 NFL Combine participants, reported that quarterbacks had the highest rate of shoulder injuries, followed by defensive backs and linebackers. Those authors further broke down their findings by specific injury, describing anterior instability as a defensive injury, as defensive linemen, linebackers, and defensive backs sustained this injury more frequently than players in other positions. 8
We also found a higher prevalence of anterior tears in defensive players, although offensive linemen and running backs had rates similar to those of defensive linemen. Kaplan et al 8 suggested that defensive players sustained anterior labral tears more frequently because of the high-velocity impact during tackling, which occurs with the arms outstretched away from the body. Funk and Snow 7 corroborated this explanation, stating that the typical mechanism of labral injury in rugby players was related to shoulder trauma secondary to tackling. In terms of posterior tears, Kaplan et al 8 found that offensive and defensive linemen were at higher risk, and the authors attributed this finding to the loads placed on forward-flexed, adducted, and internally rotated arms during blocking and shedding blocks, sustaining posteriorly directed forces of the humeral head on the glenoid. Our study’s findings are in accordance with this conclusion, as offensive linemen, tight ends, and long snappers—three positions commonly involved in blocking—had the highest rates of posterior tears.
The decision to treat labral injuries surgically often depends on surgeon and patient preference, patient expectations, and sport-specific demands. Some physicians recommend surgery for all throwing athletes with labral tears, while other physicians consider the extent of the injury, the demands placed on the athlete, or the severity of symptoms. 2,10 Nearly 55% of shoulders with MRI-confirmed labral injury in our study showed signs of previous surgical intervention on imaging. In contrast, Kaplan and colleagues, 8 in their NFL Combine study, found that 73.3% of shoulders had required surgery; however, those authors studied anterior and posterior instability rather than labral injuries, which may have excluded some players with tears but without significant symptoms.
The present study provides results that can be applied clinically to high-level football players. Sports medicine physicians should give special consideration to labral injuries in linemen and linebackers, especially when the injury was caused through a blocking or tackling technique. Similarly, coaches and trainers may be mindful of these mechanisms and more cautious when implementing them in practices or training programs. Our study found that posterior labral tears were more common than anterior tears, which should continue to increase diagnostic awareness of this injury, especially in this specific cohort. Further, our epidemiological study provides valuable data regarding the prevalence of these shoulder injuries in an elite athletic cohort, which is valuable to high school, college, and professional football coaches, associated staff, and medical professionals.
Because of the retrospective nature of this study, there were several limitations. We were not able to obtain MRI results on all scouting combine participants, and since MRI confirmation was required for diagnosis of these injuries, it is possible that some players with labral injury were not included in our study. Further, this study entailed radiographic assessment of the labrum, and the symptoms were not correlated with physical examination findings. Likewise, some players may have been asymptomatic but may have undergone MRI as a precautionary measure, especially in the setting of previous surgery. We were unable to obtain magnetic resonance angiography (MRA) consistently in this study; MRA provides greater sensitivity in detecting certain labral tears and associated injuries. Studying injuries at the NFL Combine entails an inherent selection bias because players with labral injury that significantly affected performance likely would not be invited to the combine. The patient cohort was highly specialized—elite athletes attempting to make NFL rosters—and thus the findings based on this patient cohort may not be generalizable to other football cohorts.
Conclusion
Injury involving the labrum is relatively common among NFL Combine participants, especially linebackers and linemen. Both anterior and posterior lesions were seen in at least half of these injuries, while SLAP tears were slightly less common. Further investigation is necessary to determine the impact these injuries have on player draft position, NFL performance, longevity of playing career, and need for future surgical intervention.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.M. receives research support from DJO and Smith & Nephew. S.J.F. receives research support from DJO. J.P.B. receives royalties from Arthrex. R.F.L. receives royalties from Arthrex, Ossur, and Smith & Nephew; is a paid consultant for Arthrex, Ossur, and Smith & Nephew; and receives research support from Arthrex, Linvatec, Ossur, and Smith & Nephew. M.T.P. receives royalties from Arthrex and Slack Inc and is a paid consultant for Arthrex and Joint Restoration Foundation (AlloSource).
Ethical approval for this study was obtained from the Partners Human Research Committee.