
Abstract
Background:
Multiligament knee injuries cause significant functional impairment. Adults undergoing anatomic reconstruction of multiligament knee injuries have excellent outcomes postoperatively. However, less is known about the outcomes in adolescent patients following multiligament reconstruction.
Purpose/Hypothesis:
We aimed to assess patient outcomes and failure rates following unstaged multiligament reconstruction in an adolescent population at a minimum 2-year follow-up. We hypothesized that outcomes of multiligament reconstruction in these patients would be comparable to previously reported outcomes in the adult population.
Study Design:
Case series; Level of evidence, 4.
Methods:
The study included patients who had undergone multiligament knee reconstruction at 19 years of age or younger and had at least 2 years of follow-up. All procedures were performed by the same surgeon. Exclusion criteria included patient age 14 years or younger at the time of surgery, open physes, prior ipsilateral meniscal or knee ligament surgery, or a tibial plateau fracture at the time of injury. Multiligament reconstruction was defined as a reconstruction of at least 1 cruciate ligament and at least 1 component of the posterolateral corner or the medial knee. Patients were evaluated according to Lysholm score, Tegner score, Short Form–12 physical component summary (SF-12 PCS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score, and postoperative patient satisfaction.
Results:
Twenty patients (mean age, 17.7 years; mean follow-up, 37.1 months) were included in this study. No patient required additional ligament surgery after the index surgery because of graft failure. The median preoperative Lysholm score was 49.5 (range, 18-90), and the median postoperative Lysholm score was 86 (range, 44-100) (P < .001). The median preoperative Tegner activity score was 2 (range, 0-9), and the median postoperative Tegner activity score was 6 (range, 2-10) (P = .012). The median SF-12 PCS improved from 40.5 preoperatively to a median of 56.1 postoperatively (P < .001). WOMAC total score improved from a median of 26.5 preoperatively to a median of 2 postoperatively (P < .001). Median postoperative patient satisfaction was 10 (range, 5-10).
Conclusion:
Single-stage multiligament knee reconstruction is a reliable procedure that improves knee function at 2-year follow-up in adolescent patients. Patient satisfaction was excellent, but longer follow-up in a larger series of patients is required to determine the long-term benefits of multiligament reconstruction in this patient population.
Multiligament knee injuries constitute a challenging subset of orthopaedic injuries that can cause significant functional impairment and long-term sequelae, especially in the adolescent population. 24,48 Adolescents comprise a unique, challenging subset of patients for a number of reasons. Growth disturbance can occur after ligamentous knee surgery in children and can include genu recurvatum due to tibial tubercle apophyseal arrest, as well as limb length discrepancy and angular deformity due to physeal arrest or overgrowth. Anatomically, adolescents have decreased intercondylar notch width, increased posterior tibial slope, increased anterior pelvic tilt, increased femoral anteversion, and increased quadriceps angle. 7,44,50,54,55 Biomechanically, adolescents, especially females, demonstrate increased knee abduction angles, limited dynamic knee flexion, and asymmetrical landing. 53 Hormonally, sex hormone receptors within the anterior cruciate ligament (ACL), including those for estrogen, testosterone, and relaxin, may alter the biomechanical properties of the ACL, thereby increasing the risk of injury. 8 Psychologically, the ability to adhere to requirements and restrictions inherent to long-lasting rehabilitation programs is more challenging for adolescents. 9
The incidence of multiligament knee injuries and the outcomes following multiligament reconstruction in the adolescent population are lacking. Multiligament injuries were initially reported to occur at a rate of fewer than 0.0125 events per 100 patient-years, with most studies reporting on the adult population. 15,21,46 However, more recently, Arom et al 2 reported a higher incidence of knee dislocations, which were used as a surrogate for multiligament knee injuries (0.072 events per 100 patient-years) using a national database. This reported increase may be due to a better understanding of multiligament knee injury and improved objective diagnostic methods.
Higher failure rates and consequently poorer subjective and objective outcomes have been reported after repairs of the cruciate and collateral ligaments; therefore, anatomic reconstruction of all ligamentous structures is recommended. 22,37,38 An unstaged procedure is advocated when possible to minimize the risk of graft failure and to allow for early range of motion. § Numerous anatomic and nonanatomic techniques have been described for each individual reconstruction; in general, anatomic reconstructions are preferred because they restore near-native knee biomechanics and have been validated to improve patient outcomes and objective radiographic measurements. 30,32,58
With participation in youth sports near record numbers, the identification, diagnosis, and treatment of pediatric ACL injuries have increased nearly 10-fold. 56 Despite the increasing incidence of ACL injuries, multiligament knee injuries in the adolescent population are scarce, 13,26,59 and thus the literature on indications, surgical timing, outcomes, and complications is limited. 40
The purpose of this study was to assess patient outcomes and failure rates following unstaged multiligament reconstruction in the adolescent population at a minimum 2 years of follow-up. We hypothesized that outcomes of multiligament reconstruction in this subset of patients would be comparable to previously reported outcomes in the adult population.
Methods
Study Design
This study was approved by the institutional review board of Vail Valley Medical Center. A prospectively collected, institution-based patient outcomes database was searched retrospectively. Inclusion criteria were as follows: patients who sustained a multiligament knee injury; subsequently underwent multiligament reconstruction performed by a single surgeon at the age of 19 years or younger; and had at least 2 years of follow-up. The upper limit of 19 years of age was selected to reflect the World Health Organization’s definition of adolescence. 1 Patients were excluded from this study if they had open physes, were younger than 14 years at the time of surgery, underwent prior ipsilateral meniscal or knee ligament surgery, or sustained a tibial plateau fracture at the time of injury. For the purpose of this study, multiligament reconstruction was defined as a reconstruction of at least 1 cruciate ligament (ACL, posterior cruciate ligament [PCL]) and at least 1 component of the posterolateral corner (PLC) or the posteromedial knee. Failure was defined as any patient requiring additional ligament surgery after the index multiligament reconstruction.
Patient Demographics
Our data query yielded 20 patients. Demographic characteristics, including patient age, sex, and body mass index, were recorded (Table 1). Stress radiographs (Figures 1 and 2) and magnetic resonance imaging were obtained for every patient to assess the extent of the injury and identify associated pathologic features. 17,20,27,29
Patient Demographics (N = 20)


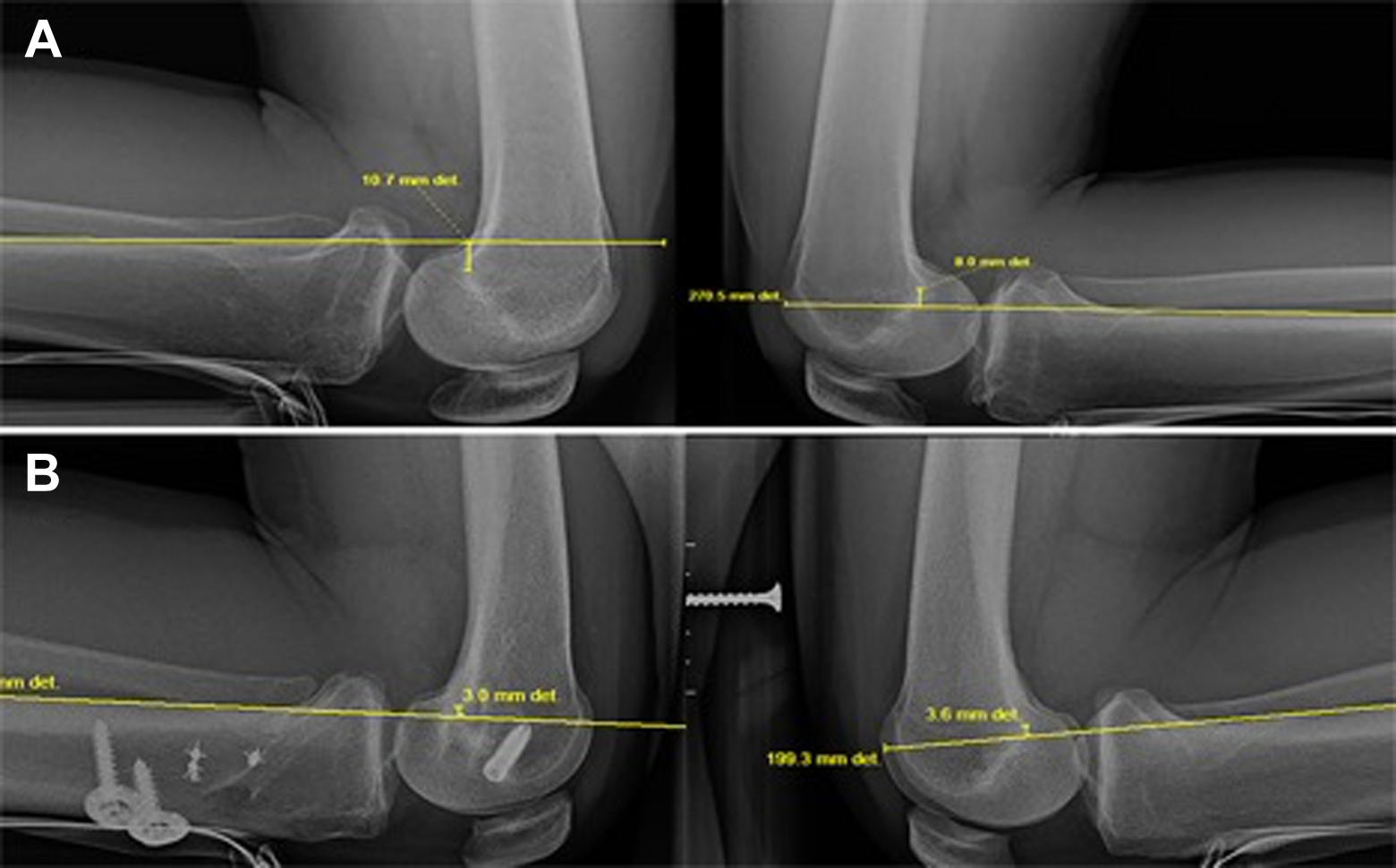
(A, B) Preoperative valgus stress views demonstrating increased medial joint space widening due to a medial collateral ligament tear. (C, D) Postoperative valgus stress views show symmetric medial opening.
(A) Preoperative posterior cruciate ligament (PCL) kneeling stress radiographs demonstrating a side-to-side difference of 18 mm of increased posterior tibial translation, which is correlated with a complete PCL injury. (B) Postoperative PCL kneeling stress radiographs demonstrating –0.6 mm side-to-side difference of posterior tibial translation. The negative sign shows that the operated side has 0.6 mm less posterior tibial translation compared with the normal, uninjured side.
For medial collateral ligament (MCL) injuries, as assessed with a valgus stress test, a side-to-side difference of <3.2 mm was considered normal or a partial tear, a difference of 3.2 to <9.8 mm was considered a complete superficial MCL (sMCL) tear, and a difference of ≥9.8 mm was considered a complete tear of all medial structures. 27 For fibular collateral ligament (FCL) injuries, as assessed with a varus stress test, a side-to-side difference of <2.7 mm was considered normal or a partial tear, a difference of 2.7 to <4 mm was considered an isolated FCL tear, and a difference of ≥4 mm considered a complete PLC injury. Patients with a ≥3.2 mm side-to-side difference of medial gapping on valgus stress testing or a ≥2.7 mm side-to-side difference of lateral opening on varus stress testing compared with the normal contralateral knee were deemed operative candidates for MCL and FCL reconstruction, respectively. Three patients had collateral ligament bony avulsions (2 MCL, 1 FCL) that were repaired. Intraoperative meniscal tear side (medial or lateral) and zone (red, red-white, and white-white) were noted. Chondral defect grade and location were also documented at the time of surgery; defects were graded from 1 to 4 based on the Outerbridge classification system. 45 Grade 1 entailed softening and swelling of cartilage; grade 2, a partial-thickness defect <13 mm in diameter; grade 3, a defect >13 mm in diameter; and grade 4, erosion of cartilage down to the subchondral bone.
Subjective Patient Outcomes
Preoperatively and at a minimum of 2 years following the index surgery, patients were administered a subjective questionnaire that included the following clinical outcome measures: Lysholm score, Short Form–12 (SF-12) physical component summary (PCS) and mental health component summary (MCS), Tegner activity scale, and patient satisfaction rating (measured on a 1-10 scale with 10 being very satisfied and 1 being very unsatisfied). The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain, stiffness, and total scores were also collected.
Surgical Technique
Patients were placed in the supine position on the operating table, and the operative leg was placed in a leg holder. Anatomic-based reconstructions of the cruciate ligaments, FCL, PLC, and posteromedial knee were performed according to previously reported techniques. ‖ As previously described, all extra-articular work for medial or posterolateral structure injury (structure identification, reconstruction tunnel reaming, and graft passing suture placement) was performed first to identify the injured structures prior to fluid extravasation from arthroscopy. 3,4,14,49 Next, cruciate ligament femoral tunnel reaming and passing suture placement were performed. This was followed by any indicated meniscal repair or meniscectomy, cartilage procedure(s), and then cruciate ligament tibial tunnel reaming and graft passage. The ligament reconstructions were fixed in the following order: PCL, FCL/PLC, ACL, and sMCL.
Rehabilitation
Postoperative recovery after a multiligament reconstruction procedure typically requires 9 to 12 months of rehabilitation prior to returning to full activities. Physical therapy was initiated on postoperative day 1 and focused on early quadriceps muscle activation and assisted knee flexion from 0° to 90°. In the acute phase, patients were treated with a brace, and limited range of motion exercises were initiated. Starting 2 weeks postoperatively, knee flexion was increased to full motion as tolerated. Patients who had injuries involving the PCL were placed in a dynamic PCL brace (Rebound PCL brace; Ossur) between postoperative days 3 and 5, and the PCL brace was used for 9 to 12 months. If the PCL was not involved, a knee immobilizer was used for 6 weeks, and then an ACL brace (Ossur CTi) was used for the first 6 months postoperatively. At 6 weeks postoperatively, weightbearing was initiated along with the use of a low-resistance stationary bike and 25% body weight leg presses to a maximum of 70° of knee flexion. Once the patient developed good dynamic neuromuscular control without any pain, he or she was allowed to progress to functional sport-specific exercises. Cast immobilization was not used in any of the patients. Return to athletic activities was allowed after a minimum of 9 to 12 months depending on the progression of the rehabilitation. Once the patient developed good dynamic neuromuscular control without any pain, he or she was allowed to progress to functional sport-specific exercises. When functional sport-specific exercises could be performed without pain and with good neuromuscular control as evaluated by a physical therapist, the patients were allowed to return to athletic activities.
Statistical Analysis
All scores were nonnormally distributed. Therefore, preoperative and postoperative scores were compared by use of Wilcoxon tests. Parametric and nonparametric statistical analysis was performed with the SPSS software package (version 11.0; SPSS Inc). All reported P values are 2-tailed, with a level of P < .05 indicating statistical significance.
Results
The average patient age at the time of surgery was 17.7 years (range, 14-19 years). The mean follow-up time was 37.1 months (range, 24-67 months). The mean time interval between injury and surgery was 34.6 weeks (range, 1 day to 3 years). Nine patients were treated in the acute phase (<6 weeks from injury), while 11 were treated in the chronic phase (>6 weeks from injury). Eighteen patients sustained low-energy sports-related injuries, while 2 patients sustained high-energy motor vehicle injuries. Five patients had combined ACL/MCL tears, 6 patients had combined ACL/FCL tears, 1 patient had a combined PCL/MCL tear, 3 patients had combined ACL/MCL/PCL tears, 1 patient had a combined ACL/PCL/FCL/popliteus tendon tear, 1 patient had a combined ACL/MCL/FCL tear, 1 patient had a combined PCL/FCL tear, 1 patient had a combined PCL/popliteus tendon tear, and 1 patient had a combined ACL/PCL/FCL tear. One patient had a popliteal artery bypass surgery prior to the index multiligament reconstruction. At final follow-up, all but 1 patient had returned to the same level of sport as before injury with or without use of a brace. One patient continued to be limited by pain and swelling during activity. Specific tear patterns and location data are shown in Table 2.
Summary of Injury and Intraoperative Findings a
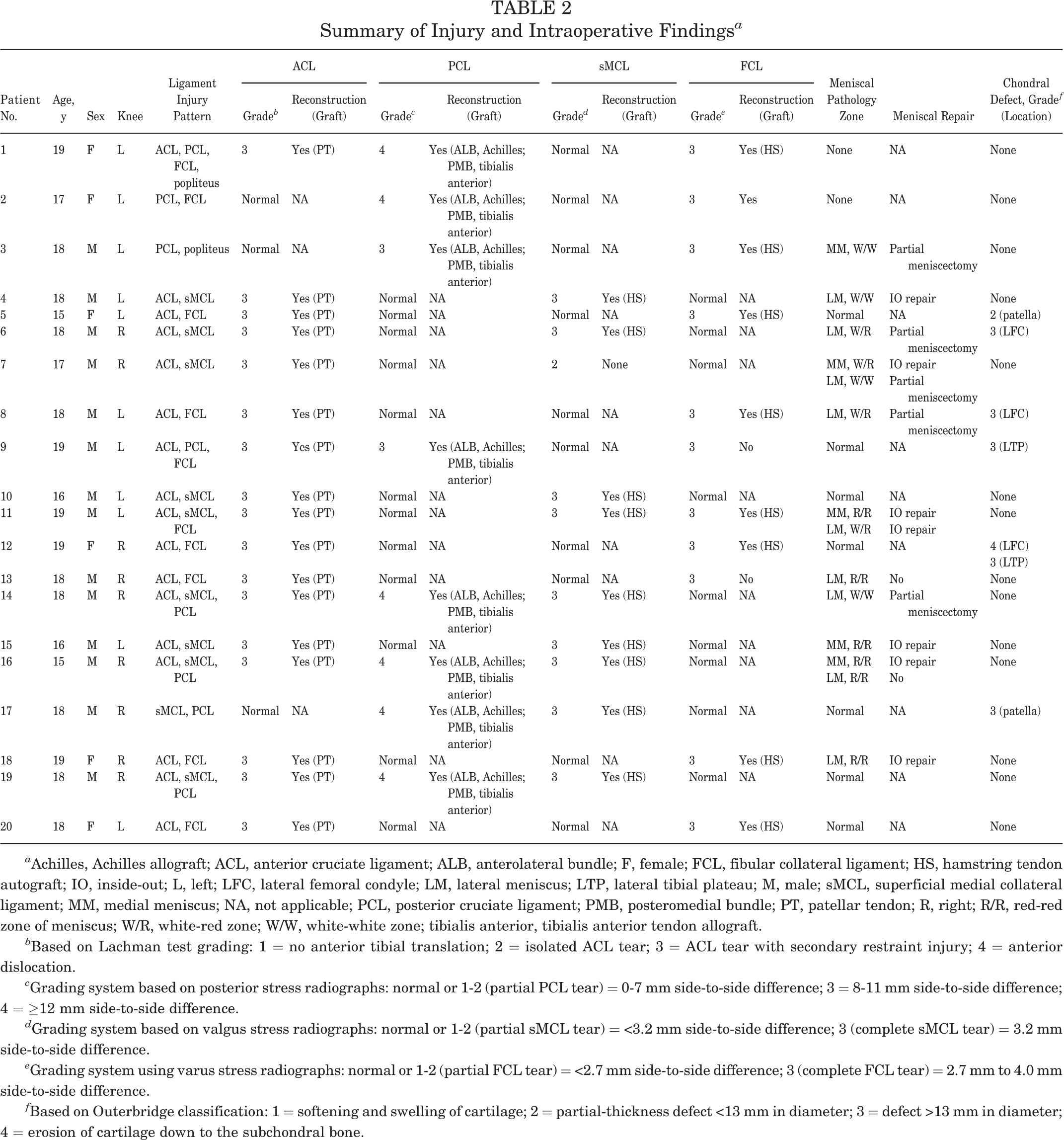
a Achilles, Achilles allograft; ACL, anterior cruciate ligament; ALB, anterolateral bundle; F, female; FCL, fibular collateral ligament; HS, hamstring tendon autograft; IO, inside-out; L, left; LFC, lateral femoral condyle; LM, lateral meniscus; LTP, lateral tibial plateau; M, male; sMCL, superficial medial collateral ligament; MM, medial meniscus; NA, not applicable; PCL, posterior cruciate ligament; PMB, posteromedial bundle; PT, patellar tendon; R, right; R/R, red-red zone of meniscus; W/R, white-red zone; W/W, white-white zone; tibialis anterior, tibialis anterior tendon allograft.
b Based on Lachman test grading: 1 = no anterior tibial translation; 2 = isolated ACL tear; 3 = ACL tear with secondary restraint injury; 4 = anterior dislocation.
c Grading system based on posterior stress radiographs: normal or 1-2 (partial PCL tear) = 0-7 mm side-to-side difference; 3 = 8-11 mm side-to-side difference; 4 = ≥12 mm side-to-side difference.
d Grading system based on valgus stress radiographs: normal or 1-2 (partial sMCL tear) = <3.2 mm side-to-side difference; 3 (complete sMCL tear) = 3.2 mm side-to-side difference.
e Grading system using varus stress radiographs: normal or 1-2 (partial FCL tear) = <2.7 mm side-to-side difference; 3 (complete FCL tear) = 2.7 mm to 4.0 mm side-to-side difference.
f Based on Outerbridge classification: 1 = softening and swelling of cartilage; 2 = partial-thickness defect <13 mm in diameter; 3 = defect >13 mm in diameter; 4 = erosion of cartilage down to the subchondral bone.
Concomitant Injuries
Seven patients had chondral defects at the time of surgery. The location and grade of chondral defects are reported in Table 2. All patients with chondral defects were treated with chondroplasty. Eleven patients had meniscal tears (2 medial meniscus, 6 lateral meniscus, and 3 bicompartmental menisci) confirmed at the time of surgery. Six patients underwent meniscal repair, and 5 patients underwent partial meniscectomy. Two patients underwent proximal tibial osteotomies in a staged fashion prior to ligamentous reconstruction. Specifically, 1 patient presented 8 months after initial injury and 5 months following ACL reconstruction with severe genu recurvatum (10 cm increased side-to-side heel height) and significant varus stress gapping at both full extension and 30° of flexion. Physical examination and imaging demonstrated ACL graft rupture, MCL tear, PCL tear, genu varus alignment (with the weightbearing axis crossing the tibial plateau at the 24.6% mechanical axis line from medial to lateral), and a grade 3 PLC injury based on varus stress radiographs. The patient underwent a proximal medial tibial opening wedge osteotomy followed by reconstructions of the ACL, PCL, PLC, and sMCL 7 months later. The other patient presented 4 years after initial injury and 2 years after reinjury. He had previously undergone an ACL reconstruction. Examination and imaging revealed an 8.5-cm heel height indicative of severe genu recurvatum, severe valgus malalignment, a flat tibial sagittal plane tibial slope of 3°, a grade 3 PLC injury based on varus stress radiographs, and ACL graft rupture. The patient underwent a proximal tibial anterolateral opening wedge osteotomy followed by reconstructions of the ACL and PLC 9 months later.
Patient-Reported Outcomes
The median Lysholm score was 49.5 preoperatively and 86 postoperatively (P < .001). The median Tegner activity score was 2 preoperatively and 6 postoperatively (P = .012). The SF-12 PCS improved from a median of 40.5 preoperatively to 56.1 postoperatively (P = .0008). WOMAC total score improved from a median of 26.5 preoperatively to 2 postoperatively (P < .001). Median patient satisfaction with outcome was 10 (range, 7-10). The improvements in Lysholm, Tegner, SF-12 PCS, and all WOMAC scores from preoperative to postoperative status were statistically significant (P < .05). Outcome scores are summarized in Table 3.
Patient-Reported Outcome Scores at Preoperative and Postoperative Assessment a

a MCS, mental health component summary; NA, not applicable; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Reported as median values and ranges.
We performed an additional analysis to examine whether there were any differences in acute or chronic treatment, which demonstrated no significant difference for any outcome score between those treated acutely and those treated chronically. We have included this information in Table 4.
Acute Versus Chronic Treatment Effect on Postoperative Outcome Scores a
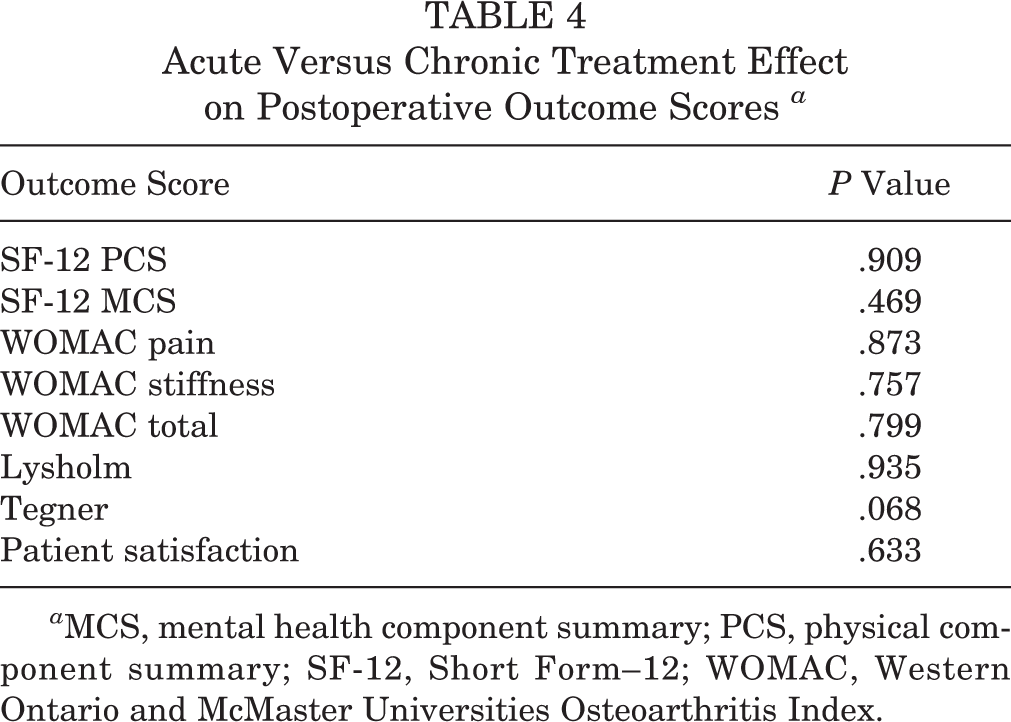
a MCS, mental health component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Reoperations and Complications
Two patients went on to have additional ligament surgeries after sports-related reinjury to the ipsilateral knee: 1 patient had a tear of the PCL grafts and was treated with a revision double-bundle PCL reconstruction, while the other patient had a revision ACL reconstruction after a tear of the ACL graft. Both reinjuries occurred 1 year after the index surgery. None of the patients had arthrofibrosis, infection, deep venous thrombosis, or hardware complications.
Discussion
The most important finding of this study was that significantly improved functional outcomes were achieved in the adolescent population, with high patient satisfaction rates after a single-stage, multiligament reconstructive knee surgery. Despite the fact that multiligament knee injuries are devastating injuries that lead to impaired function as shown by low Tegner, Lysholm, and SF-12 scores, there is a dearth of outcomes literature in the adolescent population. As a result, our findings are particularly helpful to determine prognosis and to counsel patients in this age group on their expected outcome. This study also demonstrated that concomitant meniscal and cartilage abnormalities can further impair function in the otherwise young and active population.
These results are comparable to those of a recent study in the adolescent population 11 as well as earlier studies in the adult population reporting postoperative Tegner scores of 4-5, Lysholm 83-84, and International Knee Documentation Committee (IKDC) 54-75. 10,12,22 In a systematic review, Mook et al 43 reported that patients treated with single-stage surgery after knee dislocations had higher odds of joint stiffness compared with patients treated with staged surgery. Levy et al, 38 however, found no difference in range of motion between the patients treated with single surgery compared with staged surgery. Our results are similar to those reported by Levy et al 38 in that we noted functional improvement after a single-stage surgery, with no complications reported in the follow-up period. Therefore, this study suggests that single-stage multiligament knee reconstructive surgery with early range of motion rehabilitation is a safe procedure that improves function in the adolescent patient.
Data on meniscal and cartilage integrity in multiple knee ligament injuries are lacking. In our cohort, 11 patients (55%) had meniscal lesions and 7 (35%) had chondral lesions at the time of surgery. A high incidence of meniscal and chondral lesions in association with multiligament knee injuries is reported in the adult population. 25 In a cohort of 303 patients with knee dislocations, Moatshe et al 42 reported meniscal injuries in 37.3% of the patients and cartilage injuries in 28.3%. Krych et al 25 reported on 121 patients with multiligament knee injuries, with 76% of patients having a meniscal or chondral injury (55% had a meniscal tear and 48% had a chondral injury). King et al 23 reported significantly lower IKDC scores for patients with cartilage damage or combined medial and lateral meniscal tears at a mean of 6 years in 121 patients with knee dislocations. In our cohort, the prevalence of meniscal tears and chondral lesions was comparable to that of the adult population with multiligament injuries after knee dislocations, despite most of the patients in this cohort not having knee dislocations. This demonstrated that meniscal tears and chondral lesions are also common in multiligament injuries not caused by knee dislocations, thus demonstrating the seriousness of these injuries. A detailed diagnosis and treatment plan is imperative to improve outcomes in these patients.
Most of the patients in our series had medial-sided injuries. This is in accordance with previous reports of a higher prevalence of medial-sided injuries in multiligament knee injuries. Single-stage surgery is reported to facilitate early rehabilitation and is thus recommended. 14 Biomechanical studies have reported increased forces on the ACL and PCL when the PLC was insufficient. 33,34 The FCL is particularly important in unloading the cruciate ligaments by restoring varus stability. 33,34 These data suggest that failure to address all ligamentous abnormalities can lead to nonphysiologic forces and subsequent failure.
While only a subset of our patient cohort had knee dislocations, 1 of the patients in this cohort had peroneal nerve deficits. Peroneal nerve injury is reported to occur in 16% to 40% of patients with knee dislocations and is highly associated with lateral-sided injuries. In a cohort of 303 patients, Moatshe et al 42 reported peroneal nerve injuries in 19.2% of the patients (10.9% partial and 8.3% complete deficit), while vascular injuries were reported in 5%. The odds of having a common peroneal nerve injury were 42 times higher among those with PLC injury than those without. The odds for popliteal artery injury were 9 times higher among those with PLC injuries than other ligament injury types. 42 The observed difference between our findings and those of Moatshe et al 42 can be due to the fact that only a few of the patients in our cohort had knee dislocations, compared with the entire cohort studied by Moatshe et al. 42 Furthermore, although 11 of our patients (55%) had injuries to the lateral side, only 1 patient (5%) had a complete PLC injury, suggesting that the PLC injuries in this cohort were less severe. No significant difference was found in patient-reported outcomes between medial-sided and lateral-sided injuries in this cohort. King et al 22 reported that patients undergoing medial-sided repair in a setting of multiligament knee injury had poorer outcomes in Lysholm and IKDC scores, based on a cohort of 56 patients at a mean follow-up of 6.5 years.
We acknowledge some limitations to our study. The sample size was small and may therefore not be powered to detect differences between groups. However, these injuries are not common, and it is difficult to generate large cohorts from a single center. The diverse injury patterns included in this cohort reflect the nature and complexity of these injuries but also made it difficult to compare groups. Moreover, we did not report objective measures of postoperative laxity, including stress radiographs or KT-1000 arthrometer testing. Similarly, postoperative radiographs were not assessed for the development of osteoarthritis or other objective measures. Last, this study has a relatively short follow-up, especially in this young patient population with injuries placing them at risk for arthritis.
In conclusion, single-stage multiligament knee reconstruction is a reliable procedure that improved knee function and patient-reported outcomes without failures at 2 years of follow-up in adolescent patients. Longer follow-up in a larger series of patients is required to determine the long-term benefits of multiligament reconstructive surgery in this patient population.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. receives royalties from Arthrex and Smith & Nephew; is a paid consultant for Arthrex, Ossur, and Smith & Nephew; and receives research support from Arthrex, Smith & Nephew, Linvatec, and Ossur.
Ethical approval for this study was obtained from Vail Valley Medical Center Institutional Review Board.