
Abstract
Background:
Tendon injury such as tendinopathy or rupture is common and has multiple etiologies, including both intrinsic and extrinsic factors. The genetic influence on susceptibility to tendon injury is not well understood.
Purpose:
To analyze the published literature regarding genetic factors associated with tendon injury.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A systematic review of published literature was performed in concordance with the Preferred Reporting Items of Systematic Reviews and Meta-analysis (PRISMA) guidelines to identify current evidence for genetic predisposition to tendon injury. PubMed, Ovid, and ScienceDirect databases were searched. Studies were included for review if they specifically addressed genetic factors and tendon injuries in humans. Reviews, animal studies, or studies evaluating the influence of posttranscription factors and modifications (eg, proteins) were excluded.
Results:
Overall, 460 studies were available for initial review. After application of inclusion and exclusion criteria, 11 articles were ultimately included for qualitative synthesis. Upon screening of references of these 11 articles, an additional 15 studies were included in the final review, for a total of 26 studies. The genetic factors with the strongest evidence of association with tendon injury were those involving type V collagen A1, tenascin-C, matrix metalloproteinase–3, and estrogen-related receptor beta.
Conclusion:
The published literature is limited to relatively homogenous populations, with only level 3 and level 4 data. Additional research is needed to make further conclusions about the genetic factors involved in tendon injury.
Keywords
Tendon injuries are associated with pain, morbidity, and time away from work and sports. 10,74 The series of events leading to tendon injury is multifactorial and involves a complex interaction of extrinsic and intrinsic patient factors. Repetitive forces, overuse, and drugs such as fluoroquinolones and steroids have been implicated as extrinsic factors that contribute to tendon damage, 31,41,66 while inherited disorders such as Ehlers-Danlos syndrome, endocrine and metabolic diseases such as amyloidosis, and rheumatologic diseases are intrinsic factors implicated in tendon pathogenesis. 50 In addition, several specific genetic mutations have been linked to tendon injury. 48 These pathologic genes sometimes involve single nucleotide polymorphisms (SNPs), a change in a nucleotide of a gene (eg, a thymine to cytosine). While some SNPs cause no discernible changes in gene expression, others can cause alterations in gene expression or stability. 75 The genes often involve structural proteins, such as collagen, or the repair process, such as matrix metalloproteinases (MMPs) or components of the apoptosis pathway. 38 For example, type V collagen A1 (COL5A1) has been associated with anterior cruciate ligament (ACL) tears, 62,76 while MMP3 has been associated with arthritis. 11,34
Few reviews exist in the literature that investigate the roles of genetic mutations in musculoskeletal injuries, 19,38,48 and to our knowledge, no comprehensive review of genetic factors associated with tendon injury has been published. Therefore, the purpose of this article is to systematically review the literature to summarize the genetic components that have been linked to tendon injury. We hypothesized that there are genetic factors that predispose individuals to tendon injury. As genetic testing becomes more affordable, recognition of these factors may help identify at-risk individuals, prompting heightened awareness and possible behavioral and sport modifications. Finally, while much of targeted gene therapy involving tendon rupture has looked at the reparative process, 33 the identification of predisposing factors to tendon rupture may provide additional targets for intervention, perhaps even permitting alteration of the tendon structure before the injury occurs.
Methods
Our methodology and study design for systematic review were in accordance with Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. 46 The PROSPERO database, a prospective public-access register of systematic reviews, was checked for similar protocols prior to the initiation of this project.
Search Methodology
The PubMed, Ovid, and ScienceDirect databases were searched from their inception until March 14, 2016, using search terms specific to our topic (Table 1). Only English-language papers were included in the search. In addition, a secondary search was conducted to screen the references of full-text studies included in the systematic review. The search results were imported into reference-manager software (EndNote X7; Clarivate Analytics), and duplicates were removed. The reference-manager program Mendeley (Elsevier) was used during manuscript preparation.
Search Terms and Results a
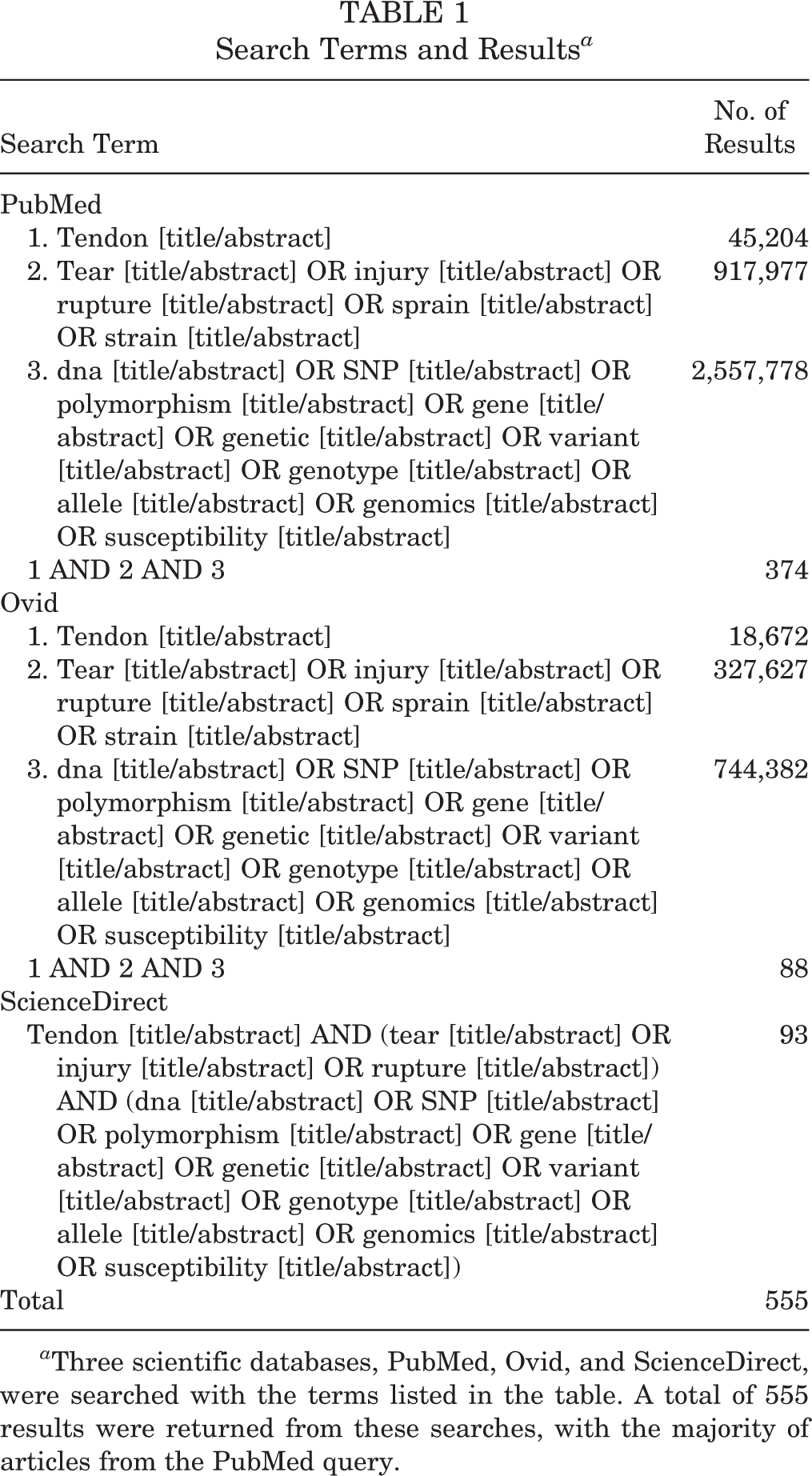
a Three scientific databases, PubMed, Ovid, and ScienceDirect, were searched with the terms listed in the table. A total of 555 results were returned from these searches, with the majority of articles from the PubMed query.
Inclusion and Exclusion Criteria
Studies were included if they specifically addressed genetics and tendon injuries, including both complete and partial tendon ruptures, tendinosis, tendinopathy, and tendinitis. Review papers, abstracts, meeting letters, letters to editors, and commentaries were excluded. Animal studies and those studies that explored genetics of tendon healing rather than injury were also excluded. To eliminate heterogeneity among our included studies, only studies that evaluated genotypic variations were included. Studies that addressed posttranscriptional factors, such as protein and mRNA expression, rather than genotypic variations were excluded. Studies that involved genetically linked systemic diseases known to have an association with tendon injury (eg, rheumatoid arthritis or alkaptonuria) were excluded.
Data Collection
The study results were screened and analyzed by 2 observers independently. Both observers screened potential articles for eligibility using the abstracts of imported studies. After initial screening, the remaining articles were printed in full text and were analyzed for inclusion/exclusion criteria (Figure 1). Decision-making conflicts between the 2 observers regarding an article’s inclusion or exclusion from the study were resolved by the senior author. A standardized form was used to mine and record information, such as authors, title, year published, type of study, level of evidence, tendons involved, gene involved, study purpose, genetic background, sample size, sample type, findings, conclusion, and references. All authors assessed the level of evidence and quality of each article using the 2003 Journal of Bone and Joint Surgery definitions for orthopaedic publications. 83 Statistical pooled quantitative data analysis could not be performed due to study heterogeneity.

PRISMA (Preferred Reporting Items of Systematic Reviews and Meta-analysis) flow diagram of the search strategy. After duplicates were removed and exclusion criteria were applied, the abstracts were hand-reviewed. Additional articles were identified from cross-referencing the studies identified.
Results
A summary of the findings is presented in Table 2. Most studies focused on a population with a specific tendon injury, most commonly Achilles tendon, and a specific gene or family of genes.
Summary of Findings (N = 26 studies) a

a ADAM, A disintegrin and metalloproteinase; BMP, bone morphogenic protein; CASP, caspase; COL, collagen; COMP, cartilage oligomeric matric protein; DEF, defensin; DENN, differentially expressed in normal and neoplastic cells; EPL, extensor pollicis longus; ESRRB: estrogen-related receptor beta; FGF, fibroblast growth factor; FGFR, fibroblast growth factor receptor; GDF, growth/differentiation factor; IL, interleukin; LOE, level of evidence; MIR, micro RNA; MMP, matrix metalloproteinase; NOS, nitric oxide synthase; TGF, transforming growth factor; THBS, thrombospondin; TIMP, tissue inhibitor of metalloproteinases; TNC, tenascin; TS, (with) thrombospondin motifs; UTR, untranslated region.
Specific Genes
ABO Blood Type
Multiple studies have attempted to define the relationship between ABO blood type and tendon injury. 40,43,45,49 In the largest study exploring the genetics of tendon ruptures, Jozsa et al 40 compared 749 patients with tendon ruptures (292 with Achilles tendon rupture, 274 with biceps tendon rupture, 113 with extensor pollicis longus [EPL] tendon rupture, 49 with quadriceps tendon rupture, and 21 with “other” tendon ruptures) to a Hungarian population consisting of 1,200,000 patient samples. They discussed blood type frequency as ratios within each group. Type O was overrepresented in tendon rupture patients compared to the general population (P < .005). The ratio of type A to type O among the tendon rupture patients was significantly different than the general population: the A:O ratio was 0.51 for subjects who sustained any tendon rupture (0.46 for quadriceps tendon rupture, 0.53 for Achilles tendon rupture, 0.60 for long head biceps tendon rupture, and 0.49 for EPL tendon rupture) compared to 1.36 in the general population. The ratio was also lower in those patients with a rerupture (0.30) and multiple rupture sites (0.20).
Similarly, Kujala et al 43 found significantly lower A:O ratios in those with Achilles tendon rupture (n = 86, A:O ratio, 1.0; P = .03) and Achilles tendinitis (n = 63, A:O ratio, 0.70; P = .10) than in a control population of 5536 young Finnish male adults (A:O ratio, 1.42). Their study also included 142 patients with rotator cuff impingement or rupture. In this case, however, they did not find a significant difference in A:O ratios between the rotator cuff pathology patients and the control patients.
Maffulli et al 49 compared 78 patients with Achilles tendon rupture to a control population of 24,501 from the general population in Scotland (blood donors over a 5-year course at a transfusion center). They found a trend toward a lower A:O ratio among 78 patients with tendon rupture (A:O, 0.47) compared to control patients (A:O, 0.68), although this did not reach statistical significance (P > .05). Interestingly, the overall prevalence of type O blood was much higher in this control population when compared to the other studies (31% of controls in Leppilahti et al 45 study, 31% of controls in Kujala et al 43 study, and 31% of controls in Jozsa et al 40 study vs 51% of controls in Maffulli et al 49 study).
To contrast, Leppilahti et al 45 analyzed 215 Achilles tendon rupture patients (179 men, 36 women) and compared them to 5536 healthy adult Finnish males as a control group (the same used in the Kujala et al 43 study); they found no significant differences in A:O ratios between the 2 groups (1.42 in controls vs 1.82 in rupture patients, P > .05).
Tenascin-C (TNC)
TNC is a glycoprotein that appears to play a role in cell adhesion and signaling, including cell proliferation and migration. 25,39,67 Two studies demonstrated an association between the TNC gene and Achilles tendinopathy. In one of the first case-control genetic association studies investigating tendinopathies, Mokone et al 55 discovered an overrepresentation of 12 or 14 GT dinucleotide repeats (P < .001) and underrepresentation of 13 or 17 allele repeats (P < .001) within the TNC gene among South African recreational athletes suffering from Achilles tendinopathy (n = 72) or tendon rupture (n = 42) compared to age- and sex-matched controls (n = 127). Using a similar study population with the addition of an Australian population, Saunders et al 70 genotyped subjects for the rs13321, rs2104772, and rs1330363 polymorphisms of the TNC gene and found that those with Achilles tendinopathy contained the T allele within rs2104772 less frequently (0.43 and 0.46 in controls vs 0.38 and 0.37 in Australian and South African populations, respectively; P = .017) and the G allele within rs1330363 more frequently (0.43 and 0.38 in controls vs 0.52 and 0.46 in Australian and South African populations, respectively; P = .02) than controls. They also found no significant difference between groups when testing several polymorphisms of COL27A1 within the same populations.
COL5A1
The COL5A1 gene provides instructions for production of type V collagen, which is important in regulating the width of collagen. 17 Five studies investigated the association of the gene COL5A1 and tendon pathology. 1,29,47,56,71 The rs12722 BstUI polymorphism has been consistently linked to tendon injury. Galasso et al 29 and Longo et al 47 each described a case of the rs12722 polymorphism (with a C to T mutation at position 6166 for a TT code) associated with spontaneous bilateral quadriceps tendon ruptures, which, in at least 1 case, occurred within a tendon containing histologically disoriented collagen and decreased type V collagen expression when compared to 3 healthy control samples. A case-control study by Mokone et al 56 (South African population, 111 tendinopathy patients vs 129 controls; P = .004) demonstrated a protective effect of the A2 allele of the BstUI polymorphism (29.8% of control subjects vs 18.0% of tendinopathy patients; P = .004), which appears to confer against the development of Achilles tendinopathy. This was corroborated in a follow-up study in South African and Australian patients by September et al 71 in 2009, with a lower risk of chronic tendinopathy in patients with a CC genotype in both Australian and South African populations (odds ratio [OR], 0.42 and 0.38, respectively; P = .017 and .008, respectively). In addition, unlike in the aforementioned South African population, the rs3196378 polymorphism was associated with Achilles tendinopathy in the Australian population, with the AC genotype significantly overrepresented (OR, 2.3; 95% confidence interval [CI], 1.3-4.1; P = .004). In the same study, the authors discovered that the TC-inferred haplotype (rs12722, rs3196378) was more common in the Achilles tendinopathy group compared with all other haplotypes.
Abrahams et al 1 investigated variants of the untranslated region of the COL5A1 gene: rs71746744, rs16399, and rs1134170. In this case-control study of 342 control and 160 tendinopathy patients, overrepresentation of the AGGG/AGGG variant of rs71746744 (P = .008), the –/– ATCT variant of rs16399 (P = .015), and the TT variant of rs1134170 (P = .014) was present within the tendinopathy population, again demonstrating a significant association between this gene and tendon injury.
COL1A1
The COL1A1 gene is responsible for providing the blueprint for production of the pro-α1(I) chain of type I collagen, the most common structural collagen in humans. 16 Two studies independently found no association between tendinopathy and rs1800012 variations at the COL1A1 gene. Posthumus et al 63 studied the COL1A1 gene at its Sp-1 transcription factor binding site, SNP rs1800012 (TT, GT, or GG), and found no significant difference between groups containing 85 Achilles tendinopathy patients, 41 Achilles rupture patients, and 125 asymptomatic controls. Erduran et al 24 investigated the relationship between the same rs1800012 SNP of the COL1A1 gene and tendinopathy of the extensor tendons at the lateral epicondyle of the elbow (ie, tennis elbow). The authors found no difference in the genotypic frequencies of a variant of rs1800012 (guanine to thymine substitution at position 1546 at the first intron) between the study group and 103 control patients matched for country of birth, sex, age, and hand dominance.
COL11A1 and COL11A2
The COL11A1 and COL11A2 genes encode for pro-α1(XI) and pro-α2(XI) chains of type XI collagen. Type XI collagen is found in cartilage and is responsible for maintaining the spacing and diameter of type II collagen, important in articular cartilage. 12,13 Due to the structural and functional similarities of type XI collagen to type V collagen, Hay et al 32 investigated the genes COL11A1 (rs1676486, C/T, and rs3753841, T/C) and COL11A2 (rs1799907, T/A) and showed no differences between independent gene frequencies between 184 Achilles tendinopathy and 338 control patients. However, in the same study, the authors constructed frequencies of “pseudohaplotypes” with various permutations of the 3 SNPs and discovered that the TCT(AGGG) variant was significantly overrepresented in tendinopathy groups (25.2% vs 9.1%, P = .003). This association was seen independently and combined in the South African and Australian populations included.
COL12A1 and COL14A1
The COL12A1 gene and COL14A1 gene encode the alpha chains of type XII and type XIV collagen, respectively. Type XII collagen is involved with interactions between collagen I fibrils and the surrounding matrix, 14 while type XIV collagen assists in the regulation of fibrillogenesis. 15 In a case-control study, September et al 73 demonstrated no significant differences between 137 subjects with Achilles tendon pathology and 131 asymptomatic controls when COL12A1 (BsrI, rs240736, and AluI, rs970547) and COL14A1 (BstYI, rs4870723, and SspI, rs1563392) (genes selected for high heterozygous frequencies with preference toward nonsynonymous coding variants) were compared.
MMP3
MMPs are a family of proteins involved in the breakdown of extracellular matrix in normal physiological processes, such as tissue remodeling. In particular, the MMP3 gene encodes an enzyme that degrades fibronectin; laminin; collagens III, IV, IX, and X; and cartilage proteoglycans. 54 Two studies have studied potential relationships between the MMP3 rs679620 allele and tendon injury.
In a study by Raleigh et al, 65 3 genotypes—the GG genotype of rs679620 (37% of tendinopathy group vs 19% of controls, P = .01), the CC genotype of rs591058 (36% of tendinopathy group vs 20% of controls, P = .023), and the AA genotype of rs650108 (10% of tendinopathy group vs 2% of controls, P = .043)—were associated with an increased risk of tendinopathy. This same study failed to demonstrate any increased risk of tendon rupture among those with these genotypes (rs679620, P = .67; rs591058, P = .73; rs650108, P = .63). Interestingly, the study revealed a relationship between the MMP3 and COL5A1 genes: The lowest risk of Achilles tendinopathy corresponded with the AA or AG genotype within the MMP3 rs679620 allele in combination with the CC genotype of the COL5A1 rs12722 allele.
In a case-control cohort of white British patients, El Khoury et al 23 found no significant differences in MMP3 SNP rs679620 between those with Achilles tendinopathy and controls. When the population was grouped by sex, the variation did reach significance: MMP3 rs679620 within the male population had an overrepresentation of the AG genotype in control patients (P = .046) and the GG genotype in the rupture group (P = .009; OR, 3.3; CI, 1.4-8.2). 23
TGFB1 and GDF5
The TGFB1 gene is responsible for encoding the transforming growth factor beta–1 protein. This protein appears to be important in facilitating cell differentiation, motility, and apoptosis and is abundant within skeletal tissues and the extracellular matrix. 79 The GDF5 gene is responsible for producing growth differentiation factor 5, a ligand that binds TGFB receptors and thus regulates gene expression. 30 Posthumus et al 60 explored the relationship between the TGFB family and Achilles tendinopathy using 132 patients with tendinopathy, 39 patients with tendon rupture, and 238 control patients. While no significant differences in the TGFB1 rs1800469 genotype (P = .49) existed between groups, the TT genotype of the GDF5 rs143383 variants was found with a higher frequency among the tendinopathy patients versus controls (P = .004).
IL1B, IL1RN, and IL6
Interleukins are a family of proteins made primarily by the immune system and involved with inflammatory response. The IL1B gene encodes for interleukin-1β, a cytokine important in mediating the inflammatory response by influencing cell proliferation, differentiation, and apotosis. 35 The IL1RN gene is responsible for producing the interleukin-1 receptor antagonist, a protein that modulates a variety of interleukin-1–related immune and inflammatory responses by inhibiting the activities of interleukin-1α (IL1A) and interleukin-1β (IL1B). 36 The IL6 gene contains information necessary for production of interleukin-6, a cytokine that is primarily produced at sites of acute and chronic inflammation and has been linked to inflammation-induced diseases. 37 September et al 72 investigated variants of the IL1B, IL1RN, and IL6 genes independently and in concert with the COL5A1 BstUI CC genotype to identify associations with Achilles pathology. When comparing 175 patients with Achilles tendinopathy to 369 controls, the authors did not identify any independent associations within the polymorphisms tested: IL1B-31 T→C, rs1143627; IL1B-511 C→T, rs16944; IL6-172 G→C, rs1800795; and IL1RN-VNTR, rs2234663. However, when these alleles were found in combination with COL5A1 BstUI, a significant association with Achilles tendinopathy was revealed (P = .014).
CASP8
The CASP8 gene contains material required to generate cysteine-aspartic acid protease (caspase) 8, a proenzyme that plays a central role in executing cell apoptosis. 9 Nell et al 58 found that 2 CASP8 genotypes, rs3834129 (P = .029) and rs1045485 (P = .021), were significantly associated with Achilles tendinopathy. Greater risk of Achilles tendinopathy was seen with rs3834129 deletion/deletion than deletion/insertion or insertion/insertion.
NOS2 and NOS3
The NOS2 and NOS3 genes encode nitric oxide synthases 2 and 3, respectively, which synthesize nitric oxide. Nitric oxide is a messenger molecule that has many functions, including encouraging production of proinflammatory mediators such as IL6 and IL8. 59 In a case-control study, Nell et al 58 found no significant differences in NOS3 rs1799983 and NOS2 rs2779249 genotypes between 166 patients with Achilles tendinopathy and 358 controls (rs1799983, P = .39; rs2779249, P = .34).
ADAMTS2, ADAMTS5, ADAMTS14, and ADAM12
The ADAMTS2 and ADAMTS14 genes encode disintegrin and metalloproteinase with thrombospondin motifs 2 and 14, respectively, enzymes that process procollagen molecules into collagen molecules, 3,4 while the ADAMTS5 gene produces disintegrin and metalloproteinase with thrombospondin motifs 5, an enzyme that modulates aggrecan, a major proteoglycan of cartilage. 5 The ADAM12 gene provides the material to encode a metalloprotease involved in skeletal muscle regeneration. 2 El Khoury et al 22 investigated the ADAM family of genes using 248 asymptomatic control patients with 134 tendinopathy and 39 tendon rupture patients. There were no significant differences within the ADAMTS2 rs1054480, ADAMTS5 rr226794, ADAMTS14 rs4747096, or ADAM12 rs3740199 polymorphisms. However, the ADAMTS14 rs4747096 GG genotype was associated with a later onset of Achilles tendon injury (55 years vs 39 years, P = .024).
TIMP2
The TIMP2 gene provides the instructions necessary to produce TIMP metallopeptidase inhibitor 2, which appears to suppress the proliferative response of quiescent tissues to angiogenic factors and inhibit the activity of MMPs that degrade extracellular matrix. 81 In a case-control study using Australian and South African populations, El Khoury et al 22 found that TIMP2 rs4789932 SNP was significantly associated with Achilles tendinopathy risk, with overrepresentation of the CT genotype in patients with tendinopathy (P = .004; OR, 1.77; CI, 1.2-2.6). In a follow-up study using 118 patients with Achilles injuries (93 tendinopathy, 25 rupture) and 131 white British participants, El Khoury et al 23 again linked differences in TIMP2 rs4789932 SNP with Achilles tendon injury (P = .038). However, a different genotype, CC instead of CT, was overrepresented in tendinopathy patients (P = .012; OR, 2.5; CI, 1.2-5.1) compared to controls.
MIR608
The MIR family of genes is responsible for producing microRNAs, which are short, noncoding RNAs that regulate gene expression by altering the stability and translation of mRNAs. 53 Orthopaedically, this gene appears to regulate chondrocyte sonic hedgehog expression. 6 In addition to studying COL5A1 3′-UTR, Abrahams et al 1 explored the effects of variations in the MIR608 gene alone and in combination with COL5A1 gene alterations. Their work revealed a significant association of CC genotype at the rs4919510 SNP among those with tendinopathy (OR, 1.6; CI, 1.1-2.5; P = .023). The MIR608 CC and COL5A1 CA genotypes were overrepresented in the tendinopathy group when the MIR608 rs4919510 and the binding site on COL5A1 at rs3196378 were analyzed (OR, 1.6; CI, 1.1-2.5; P = .022).
COMP and THBS2
The COMP gene and THBS2 genes provide blueprints for creating cartilage oligomeric matrix protein (COMP) and thrombospondin 2, respectively. Both proteins are believed to be involved in cell-to-cell adhesion and communication. 20,80 Saunders et al 69 investigated the COMP and THBS2 genes in 178 Achilles tendinopathy and 340 control patients. They failed to find any significant differences in genotype distributions for the COMP variants rs730079 (P = .73) and rs28494505 (P = .99) or for the THBS2 variants rs9505888 (P = .24), rs6422747 (P = .65), and rs 9283850 (P = .60).
FGF3, FGF10, and FGFR1
The FGF3 and FGF10 genes provide the genetic information to synthesize fibroblast growth factors 3 and 10, respectively, that can bind to proteins, such as fibroblast growth factor receptor–1, a protein encoded by FGFR1. FGF proteins bind FGFRs, which span cell membranes and, when bound, trigger a cascade of intracellular events leading to cell maturation. 27,28 Salles et al 68 (2015) described 52 patients with tendinopathy among elite male Brazilian volleyball players and compared them to 86 asymptomatic volleyball players at the same level of competition (age, 18-35 years). Although FGF3 (5 SNPs), FGF10 (4 SNPs), and FGFR1 (1 SNP) genes were studied, no significant differences among these SNPs were found between those with tendinopathy and controls. When controlling for age, FGF10 rs900379 (P = .05) and FGF3 TGGTA haplotype both had borderline associations with tendinopathy (P = .05).
In a case-control study of 203 patients with rotator cuff disease and 207 control patients, Motta et al 57 found significant associations within the FGF3 gene (rs12574452, A to G base change, P = .02/.01; OR, 0.31) and the FGFR1 gene (rs13317, C to T base change, P = .08/.02; OR, 2.67; CC overrepresented in control patients) among those with rotator cuff disease. FGF10 rs11750845 (P = .03; OR, 1.52) and rs1011814 (P = .01; OR, 1.23) were noted to be significantly variant polymorphisms after the groups were adjusted for ethnic group and sex. Conversely, Teerlink et al 78 failed to find any significant associations within the FGF3, FGF10, and FGFR1 genes in a cohort of patients with magnetic resonance imaging (MRI)–confirmed rotator cuff tears and controls.
BMP4
The BMP4 gene encodes bone morphogenic protein 4, a cytokine important in the induction of bone and cartilage formation. 8 In a case-control study of volleyball players with tendinopathy, Salles et al 68 identified a significant association between BMP4’s SNP rs2761884 and tendinopathy, with patients carrying the T allele twice as likely to have tendinopathy (P = .007; OR, 2.0; CI, 1.2-3.5).
ESRRB
The ESRRB gene affords the template for the production of estrogen-related receptor β, the exact function of which is unknown but appears to induce the expression of PPARGC1 and ESRR-induced regulator muscle 1 (PERM1) in the skeletal muscle. 26 Motta et al 57 identified 2 SNPs, rs4903399 (C to T base change, P = .09/.03; OR, 0.64) and rs1676303 (C to T base change, P = .0002/.0008; OR, 0.23), that were significantly overrepresented in the rotator cuff disease group compared to controls. Teerlink et al 78 compared 175 patients with an MRI-confirmed full-thickness rotator cuff tear to 2595 genetically matched controls and found that the ESRRB SNP rs17583842 was significantly associated with rotator cuff tear (P = 4.4 × 10–4), with a higher minor allele frequency in tear patients versus controls (OR, 1.4; CI, 1.1-1.8). They also constructed gene haplotypes to identify frequencies in control versus tear patients and found 2 haplotypes containing the risk allele of rs17583842 that were much more frequent in the tear patients (13.9% vs 2.2% in controls, P < .0001; 12.9% vs 2.7% in controls, P < .0001).
DEFB1
Defensin β1 is a peptide encoded by DEFB1, produced by neutrophils, and believed to be important in resisting microbes from binding to epithelial surfaces. 21 Motta et al 57 found an association of the DEFB1 SNP rs1800972 (C to G base change, CC genotype underrepresented in RCD, P = .004/.005; OR, 1.98) with rotator cuff disease.
Injury severity
Only 1 study attempted to correlate severity of injury with genotype. Pruna et al 64 studied soft tissue injuries in elite soccer athletes. Of 73 injured athletes studied, 15 patients had various severities of patellar tendon injury. The authors found no significant differences between athletes with mild, moderate, or severe injuries when comparing genotypes COL1A1 (rs1800012, GG/GA/AA), COL5A1 (rs12722, TT/TC/CC), TNC gene (rs2104772, AA/AT/TT), elastin (rs2289360, AA/AG/GG), titin (rs2742327, AA/AG/GG), SRY-related HMG box (rs4227, TT/TG/GG), insulin-like growth factor 2 (rs3213221, CC/CG/GG), and chemokine (CC motif) ligand 2 (rs2857656, GG/GC/CC). They did not include a comparison to a control population.
Discussion
A total of 26 articles were included in this review, and 34 different genes were investigated (Table 2). These genes were selected for their relationship to tendon form or function (eg, reparative pathways, responses to injury, tendon assembly). Over one-third (10/26) of the studies included in this review found no significant associations between the genes studied and tendinopathy. Thirteen independent genes had polymorphisms that correlated with tendon injury (tendinopathy or rupture). The strongest of these associations were seen with the genes involving type V collagen A1, tenascin-C, matrix metalloproteinase–3, and estrogen-related receptor beta. The majority of the studies involved subjects with Achilles tendon pathology.
The most convincing and consistent data supported a genetic association between tendon injury and COL5A1. While contributing relatively little to overall tendon composition, the molecule plays an important role in fibril formation by interacting with type I collagen to help regulate overall fibril size and matrix organization. 82 Several articles, including 2 patients with bilateral quadriceps tendon rupture 29,47 and 2 case-control genetic studies, 56,71 revealed an association between the rs12722 variant (BstUI within the 3′-UTR of COL5A1) and tendon injury. Other loci within the 3′-UTR were independently associated with tendon injury. 1 In addition to an association with tendon injury, COL5A1 has been linked to inherited musculoskeletal disorders such as Ehlers-Danlos, 51 acquired injuries such as ACL tears, 62,76 and overall joint range of motion. 18
Besides those focusing on the COL5A1 gene, several other studies identified significant associations between SNPs and tendon injury. No clear functional group (eg, genes involved in tendon repair or collagen structure) has a predominant association with tendon injury. Rather, SNPs that have been associated with tendon injury have a diverse array of functions. Some genes that are associated with tendon injury have a clear relationship to the structure and maintenance of musculoskeletal tissues, for example, MMP3 (rs679620, rs591058, rs650108) 65 and GDF5 (rs143383), 60 and have been previously associated with other orthopaedic conditions. 5,9,15,35,70 However, other significantly associated polymorphisms, such as BMP4 (rs2761884), 68 CASP8 (rs1045485, rs3834129), 58 ESRRB (rs4903399, rs1676303, rs17583842), 57,83 MIR608 (rs4919510), 1 TIMP2 (rs4789932), 22,23 TNC (rs2104772, rs1330363), 37,75 and DEFβ1 (rs1800972), 57 have less clear roles in tendon repair and function.
Interestingly, a number of other collagen genes investigated (COL1A1, COL2A1, COL11A1, COL11A2, COL12A1, COL14A1) did not have a significant independent association with tendon injury, even though they have been linked to other musculoskeletal injuries (eg, COL1A1 Sp1 with ACL tears, shoulder dislocations, osteogenesis imperfecta, and lumbar disc disease; COL2A1 with spondyloepiphyseal dysplasia). 7,24,32,42,63,70,73,77 Similarly, other genes involved in the mechanical environment, formation, and matrix structure of tendons (ADAM12, ADAMTS, COMP, DENND2, TGFB, TTN) and those involved in inflammation and tissue repair (CCL2, ELN, IGF2, IL1B, IL1RN, IL6, NOS, SOX15, THBS2) were not seen to have significant associations in the SNPs and populations studied.
A number of genes, including FGR and ABO groups, had conflicting results. Two studies identified relationships between FGF3, FGF10, and FGFR1 and the development of tendinopathy 57,68 ; however, these associations were not replicated in the study by Teerlink et al. 78 One of the most studied, the ABO gene, located on chromosome 9 near COL5A, was similarly controversial in its role in tendinopathy; 4 studies investigating the ABO gene and tendon injury had conflicting results. Some authors found a higher prevalence of type O blood in those with tendon rupture, while others failed to confirm this difference. 40,43,45,49 While having no apparent relationship to tendon form or function, the ABO gene has been speculated to be genetically associated to tendon injury due to its close proximity to genes encoding for tenascin-C and type V collagen. 43,49 Presently, there is insufficient data to definitively conclude that blood type is an independent risk factor for tendon injury.
Longo et al 48 (2015) published a selective review of the genetic susceptibility to ligamentous and tendinous injuries. Our systematic review includes an additional 16 studies to this previous selective review. The authors described 8 different genes (COL1A1, COL5A1, COL12A1, COL14A1, TNC, MMP3, TFGB1, and GDF5) in their review and discuss the associations of variants within these genes to tendon injury as well as to other types of orthopaedic injuries, most notably ACL injury. Each of the tendon injury studies described in their review was included in our study. ‡ When other musculoskeletal disorders (ACL tears and shoulder dislocations) were included, there were significant relationships seen with COL1A1 42 and COL12A1, 61 whereas these associations were not seen when tendon ruptures were investigated in isolation. In addition to their associations with tendon injuries, COL5A1 and MMP3 variants have been significantly associated with ACL ruptures. 52,62 Their review included gene expression analyses, which we specifically excluded. They reported differences in the mRNA stability of variants of COL5A1 in patients with tendinopathy versus controls. 44
John et al 38 performed a systematic review assessing genetic risks associated with ACL tears. They included 16 genetic case-control association studies and 1 cross-sectional study. The articles included looked at 20 specific genetic polymorphisms and identified positive associations in half. As seen in our investigation, many of the studies included were derived from a South African population. The authors reported conflicting results regarding significant associations of ACL injury with COL5A1 and MMP genes, unlike the consistent findings of an association seen with tendon injury in our review. These authors found genetic associations with ACL injury, including COL3A1, COL12A1, and COL1A1 among others, that we did not find to correlate with tendon injury.
This systematic review provided a thorough investigation of the current literature defining the genetic influence on tendon injury. Despite the significance of the findings, this study has several limitations. First, there is homogeneity of the populations studied: 14 of the 26 studies investigated South African and Australian patient groups identified by Mokone et al 55 in 2005 and September et al 71 in 2009. These groups may or may not be representative of the global population. In addition, the majority of these studies focused on Achilles tendinopathy specifically, and the findings may not be generalizable to other tendons. Second, most of the studies included in this review included relatively few (100-200) patients in the study groups. Third, our data collection is limited by publication bias. The studies are limited to level 3 and level 4 data. Fourth, quantitative synthesis could not be performed due to individual study heterogeneity. Finally, tendon healing was not specifically included in the search, and different genetic factors may be involved in the reparative process than in the injury process. There may be other unrecognized genes that play a large role in tendon pathology that have not yet been identified.
It may be premature and cost-prohibitive to perform genetic testing as a screening tool for these polymorphisms, especially given the multifactorial nature of tendon injury. However, this review demonstrates that there are several genes that are highly associated with tendinopathy and tendon rupture and may be useful in constructing a targeted gene panel for patients who have had multiple tendinous injuries or in families in which there appears to be a pattern of tendon injury.
Conclusion
Many studies have identified possible associations between genetic factors and tendon injury. The genetic factors with the strongest evidence of association with tendon injury were type V collagen A1, tenascin-C, matrix metalloproteinase–3, and estrogen-related receptor beta. However, the published literature is limited to relatively homogenous populations with only level 3 and level 4 data. Additional research is needed to make further conclusions about the genetic factors involved in tendon injury.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.D. is a paid consultant for Smith & Nephew and Biomet. R.A.G. receives research funding from Aesculap and has received reimbursement for speaking from Smith & Nephew.