
Abstract
The principle of periarticular fracture is well established. However, the gold standard in treating tibial plateau fracture remains controversial. Lack of adequate soft tissue and complexity of the fracture involved succumbs to poor postoperative outcomes and high complication rate for infection, implant failure and non-union. Furthermore, the treatment of the elderly complicates the decision. It is because time is an essence since decubitus complication is associated with prolonged immobilisation. In addition, other complication related to this fracture such as accelerated secondary osteoarthritis and pain leads to further immobilisation. Traditionally, secondary total knee replacement (TKR) is indicated for this type of fracture, while the initial aim is to achieve bone healing. However, its failure related complication, the detrimental challenge in addressing ligament balance, extensor mechanism scarring and patella mal-tracking, thus, it is not commonly practised. The author has successfully demonstrated the use of primary TKR with supplementary locking plate in a post-traumatic Schatzker V tibial plateau fracture in a 75-year-old gentleman to allow immediate weightbearing. Thus, removing the complication associated with immobilisation and exhibit the advantage of TKR in obtaining a painless functional knee. In successive follow-up shows a favourable outcome and improved functional knee outcome compared to the premorbid state.
Introduction
Tibial plateau fracture in an orthogeriatric patient is not uncommon, but optimal treatment remains controversial. Factors including fracture configuration, associated injury, bone quality, and surgeon skill capability are being taken into treatment consideration. Besides, a complication related to open reduction and internal fixation in these particular groups poses high complication rates, including infection, peroneal nerve palsy, inadequate reduction and inevitably, rapid progression to secondary osteoarthritis (OA). 1 Delayed weight-bearing may lead to decubitus complications associated with high mortality. Secondary total knee replacement in present failure or worsening post-traumatic OA poses a detrimental challenge in addressing ligament balance, extensor mechanism scarring, and patella mal tracking. 2 Thus, the recent hypothesis that primary total knee arthroplasty (TKA) for complex tibial plateau fracture in the elderly may provide a beneficial alternative. With the complete replacement of articular surface and stable fixation, early weight-bearing is possible. Recent studies have supported this idea for the simplest to moderate tibial plateau fractures. However, in fractures that involved the metaphyseal region, this simple idea may not be feasible.
Our case report described the surgical treatment of a challenging tibial plateau fracture involving the metaphyseal area and clinical outcome after one year. The patient was managed with total knee replacement with adjuvant osteosynthesis. The patient was able to ambulate postoperatively, and successive follow-up confirms a favourable outcome with the oxford knee score improved to good functional joint and pain. His pain was reported better than in the preoperative state.
Case report
A 75-year-old gentleman presented a history of a motor vehicle accident with pain over the right knee. Premorbid, he was an active man that jogs regularly. Physical examination revealed swelling and tenderness over the right knee with no vascular compromise and no open wound seen. Radiographs of the knee indicate a closed fracture of the right tibial plateau (Schatzker V). (Figure 1).
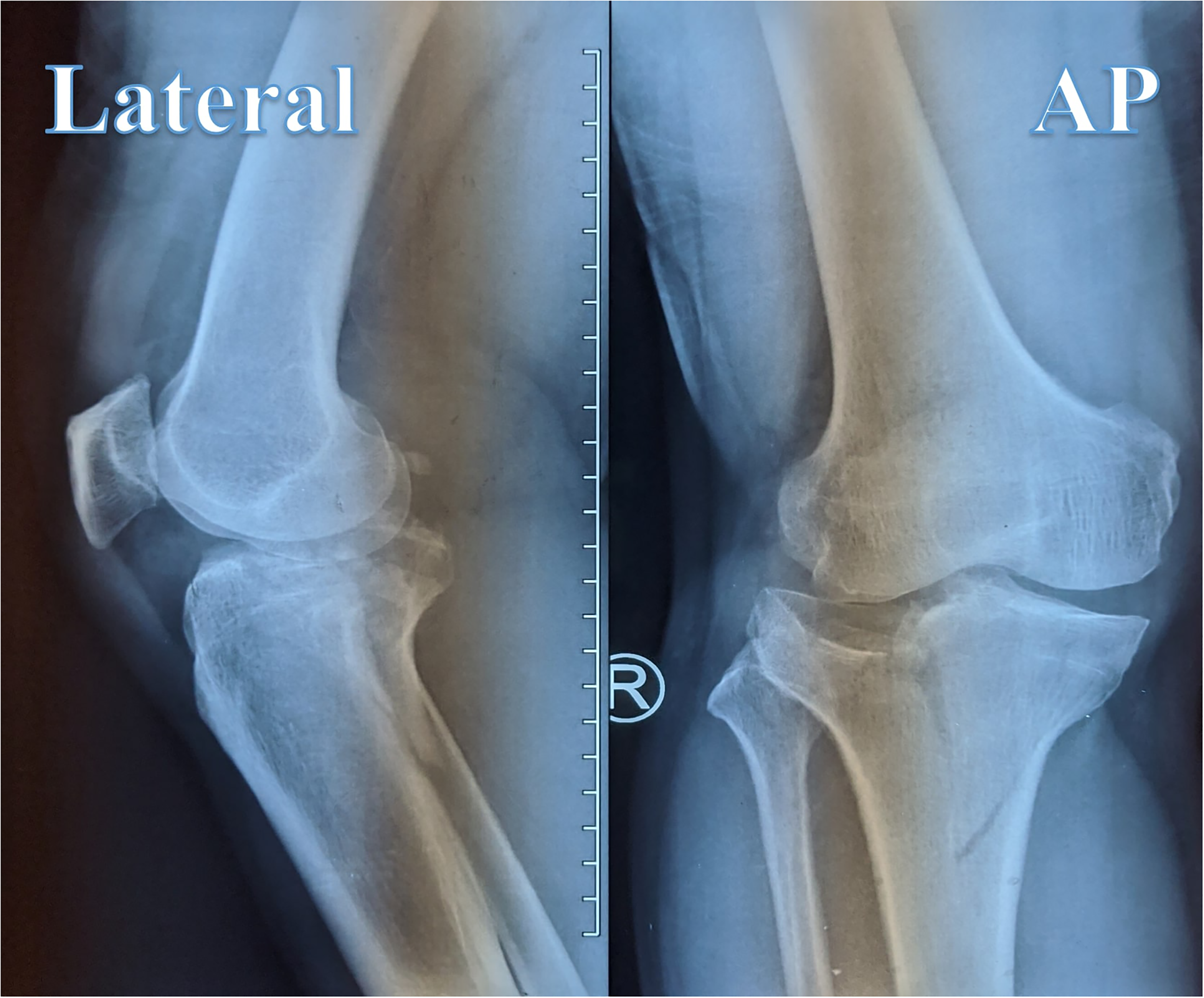
Preoperative radiograph showing tibial plateau fracture (schatzker V), anteroposterior view: displacement of the medial tibial plateau and fracture depression of lateral tibial plateau, lateral view: posterior displacement of posteromedial fragment.
The fracture's complexity warrants a computed tomography of the right knee that revealed a sizeable posteromedial piece with the comminuted medial tibial plateau. (Figure 2) (Figure 3).
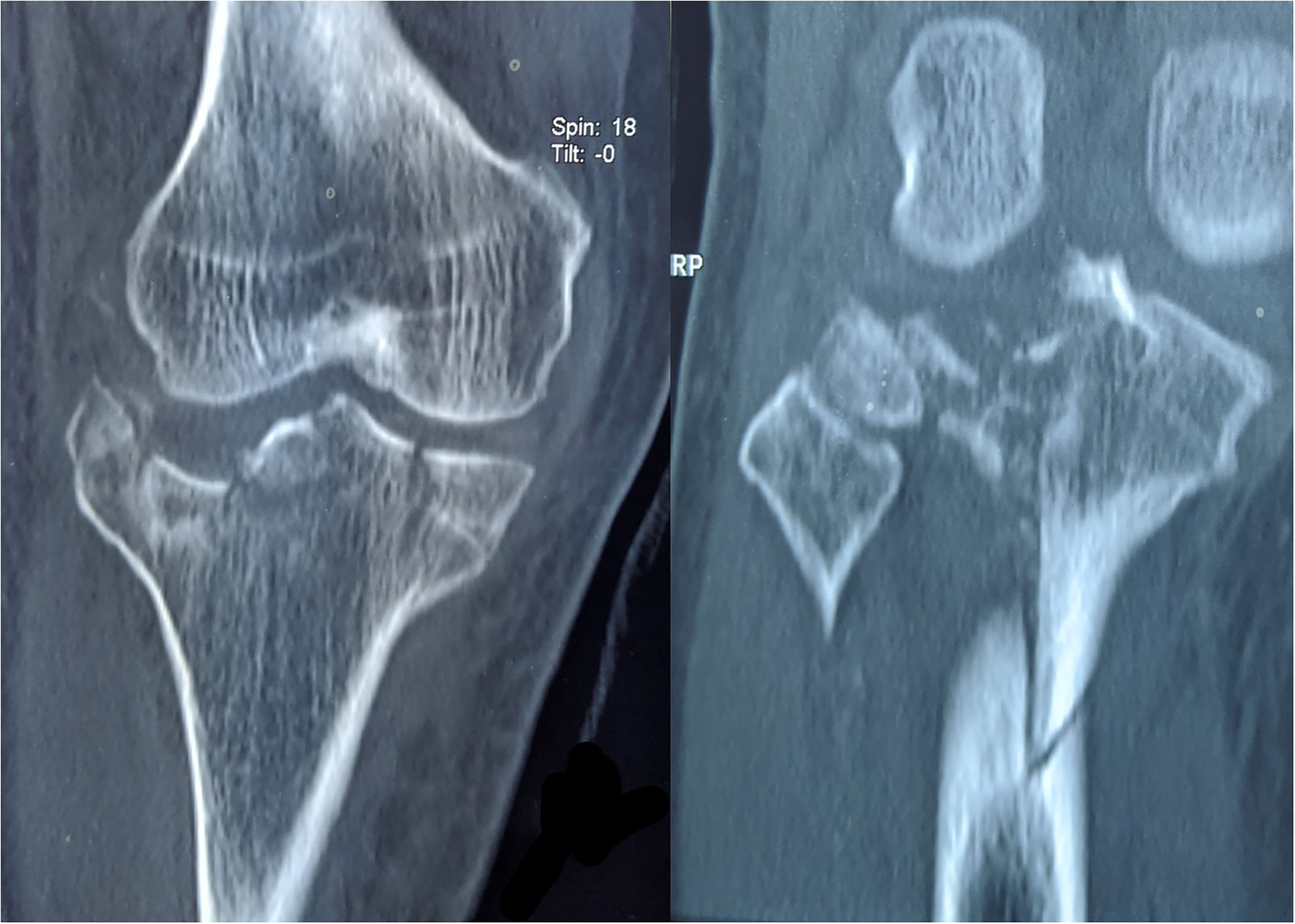
Coronal cut from CT scan shows multi fragmented fracture depression over the medial and lateral tibial plateau.
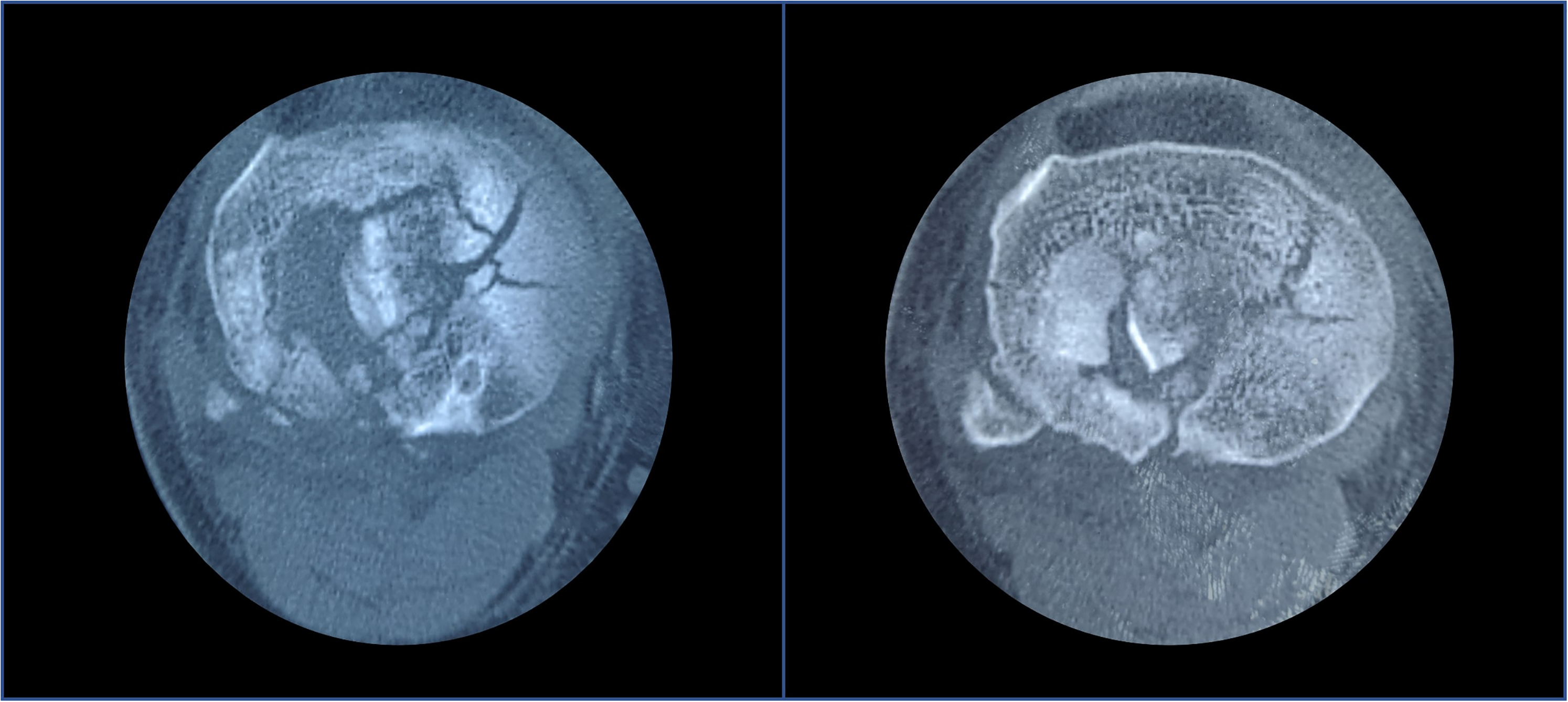
Axial cut from CT scan shows extension of the depression over lateral tibial plateau up to the head of the fibula.
After exploring his expectation, he wishes to return to his premorbid status with the slightest complication. Thus, he opted for open reduction internal fixation and primary total knee replacement with an extended tibial stem. Due to the initial condition of his soft tissue, elevation and cryo-cuff therapy were applied few days before the operation.
General anaesthesia was administered, and the patient was placed in a supine position. A midline incision with a medial parapatellar approach was used. The medial tibial plateau component was initially addressed. The medial fragment was fixed with four 4.0 mm cannulated screws angled away from the intramedullary supported with a medial proximal locking plate. The reduced medial piece was crucial as it was used as a reference for the proximal tibial cut. The femoral cut was done as primary total knee replacement. The extension and flexion gap were adequate. The tibia intramedullary was reamed for stem placement, ensuring good bone contact for press-fit and bypassing fracture site. A tibial tray with an uncemented long fluted tibia stem (14 mm) was placed. Immediate postoperative fluoroscopy shows adequate tray placement of both femur and tibia components with the restoration of the metaphyseal region. (Figure 4).
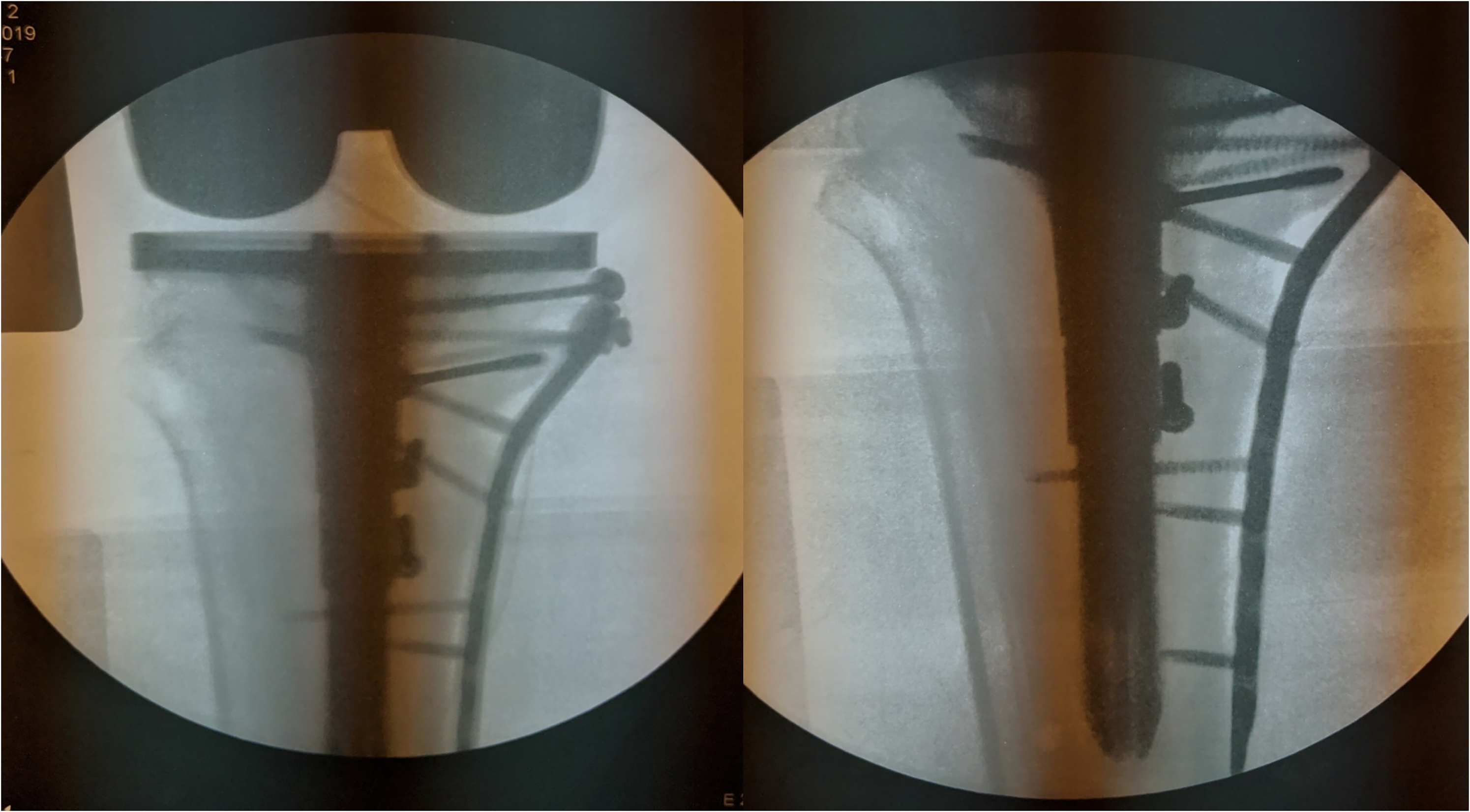
Immediate postoperative fluoroscopy shows the correct placement of tibial component with anatomical reduction of remaining fracture fragments with four 4.0 mm half-threaded cannulated screws supplement with a locking compression plate.
Postoperatively, the pain was well controlled with analgesia. Range of motion exercise was started, followed by walking frame training after three days. The patient was compliant, well progressed and was discharged after five days of hospital stay.
During his subsequent follow-up, the patient was pain-free. He made a complaint of occasional swelling but resolved with elevation and an ice pack. His range of motion was maintained at 0–90 degree throughout the follow-up, and he was pain-free. 6-month postoperative shows complete bone union with no sign of loosening. (Figure 5).
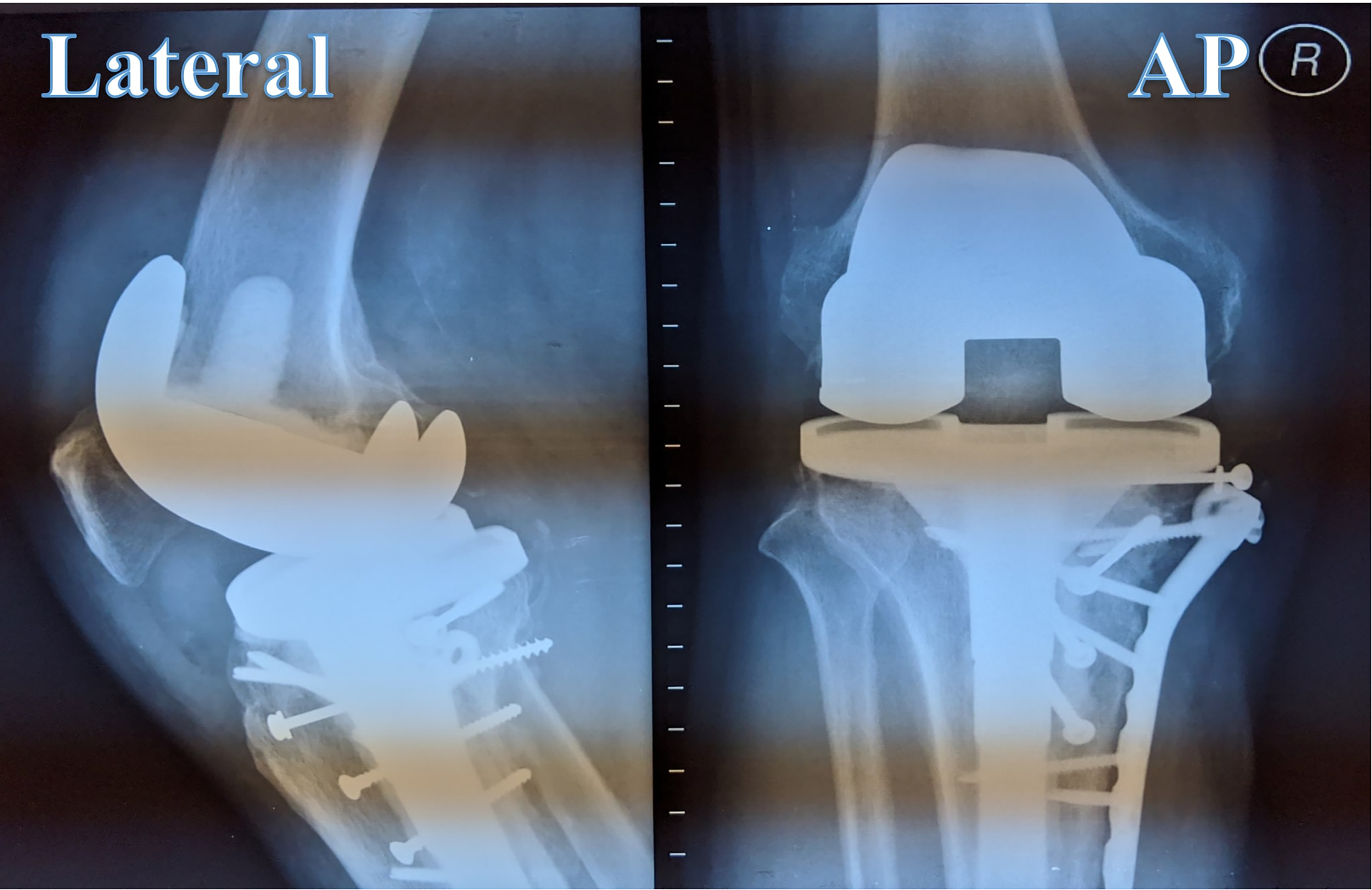
A year postoperative radiograph shows a complete bone union of tibial plateau fracture with no tibial and femoral component loosening and secondary displacement.
Discussion
Tibial plateau fracture in the elderly remains challenging. It is associated with a high rate of complication regardless of treating it conservative or surgically. Conservative management remains an option for a patient that is not fit for operation. They are subjected to decubitus complications, including bedsore, lung infections and thromboembolism. Thus, in most cases, this fracture is treated surgically. However, in the elderly, poor bone stick and complexity of fracture remains a challenge, 3 even with adequate fixation, complication rate related to open reduction including infection, stiffness, implant failure and post-traumatic knee OA. Current studies have shown that primary TKA in the elderly with acute tibial plateau fracture is associated with promising clinical, functional, and radiological outcomes.2,4 It avoids the complication of primary plate fixation and post-traumatic TKA, which can be detrimental. It seems superior to TKA in post-traumatic knee OA as it is scar-free. 3 However, the recommended choice of implant techniques for fixation and augmentation remains debatable. Abdelbadie demonstrates that TKA is a viable option for complex fracture; however, they have excluded bicondylar tibial plateau fractures from the study given the complexity of reconstruction. 1 Others recommend TKA for acute tibial plateau fracture with a partial articular fracture. The principle of zonal fixation in TKA was adopted from Morgan-Jones and his team in tackling complex tibial plateau fractures. 5
Addressing the metaphyseal region remain the mainstay as failure to gain adequate fixation in these regions will increase shearing stress and early failure and loosening of the implant. 6 Thus, we have chosen to fix the metaphyseal region for this purpose. The key-steps in achieving immediate immobilisation post operatively is by using an extended tibial stem was used. It is worthy to note that the stem should bypass the fracture side at least 5cm or at the level of the fracture site. 2 The stem serves to offload the metaphyseal region until it regains union is crucial as it protects the implant-cement interface from failing. We have chosen uncemented for two main reasons; adequate bone stock and creating a cement-free area for adequate fracture healing. 4 Extended stem, either cemented or uncemented, depends on the patient's bone stock.
This case is unique and novel as it combined a primary total knee replacement with a supplementary locking plate to address the fracture's complexity. Many cases reported opting for either total knee replacement or open reduction internal fixation.1,3,4 However, in this case, choosing either of these options is not feasible as the metaphyseal area is profoundly affected. Hence, we have decided to fix the metaphyseal area using internal fixation and replace the articular surface with a primary total knee replacement. We believe that reconstructing the metaphyseal area is essential as it prevents collapse and, later, failure and loosening of total knee replacement. Bypassing the metaphyseal area using an extended tibia stem shifted the load away from the fracture site, allowing it to heal without compromising mobilisation. Also, with an immediate range of motion exercise, stiffness can be prevented with the help of adequate multimodal pain management. 4
In conclusion, primary total knee replacement in complex tibial plateau fracture in the elderly is a viable option as it provides pain-free, early mobilisation knee joint postoperatively. However, it is technically demanding and requires proper preoperative counselling and preparation to optimise success. In addition, a study to determine its short term and long-term outcomes should be explored.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.