
Abstract
Background:
Few studies have examined whether skeletal parameters predict hamstring graft size during anterior cruciate ligament reconstruction (ACLR).
Purpose/Hypothesis:
The purpose of this study was to examine whether preoperative anthropometric and radiographic skeletal parameters could predict hamstring graft size during ACLR. We hypothesized that both anthropometric and skeletal parameters can be used to predict graft size in our double-bundle procedure and that the use of skeletal parameters will improve the accuracy of graft size prediction.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 200 patients were recruited and underwent double-bundle ACLR using a semitendinosus (ST) graft. The harvested tendon was measured to determine graft length (GL) and then split at its midpoint. The graft diameters of the anteromedial (GDAM) and posterolateral bundles (GDPL) were measured at the femoral aspect of the 2-stranded graft. The mean diameters of both bundles were included in the analysis. On the coronal radiograph, femorotibial angle (FTA), femoral interepicondylar distance (IED), and tibial plateau width (coronal tibial width [CTW]) were measured. Blumensaat line length (BLL) and the lateral tibial width (LTW) were measured on the lateral radiograph. A linear regression analysis was conducted using graft size as the dependent variable and age, sex, height, weight, Tegner activity score, and skeletal parameters as the independent variables.
Results:
Mean GL was 258.9 ± 21.9 mm, GDAM was 5.9 ± 0.5 mm, and GDPL was 5.7 ± 0.6 mm. Single regression analysis showed that GL was significantly predicted by sex, height, weight, Tegner activity score, IED, CTW, BLL, and LTW (R 2 range, 0.033-0.342). GD was predicted by sex, height, weight, IED, CTW, BLL, and LTW (R 2 range, 0.094-0.207). Stepwise multiple linear regression analysis significantly confirmed sex, height, and age as the variables to comprehensively predict GL (R 2 = 0.384). With regard to GD, stepwise multiple regression confirmed height and IED as significant variables (R 2 = 0.224).
Conclusion:
Both preoperative anthropometric and radiographic parameters on plain radiographs were able to predict harvested GL and 2-strand GD. Multivariate regression slightly improved the prediction of graft dimensions compared with univariate regression.
Keywords
There exist several choices for autografts in anterior cruciate ligament reconstruction (ACLR), such as the hamstring tendon, 7,30,51 bone–patellar tendon–bone (BTB), 33,41 and quadriceps tendon. 14,39,53 Many previous studies have reported that hamstring autografts show comparable biomechanical properties and clinical outcomes to those of central-third BTB grafts. § Additionally, during harvest, BTB occasionally causes anterior knee pain at the harvested site, 2,17,18,20,48 while morbidity is considered less common after hamstring autografts. 1,4,35 Hamstring autografts are useful because surgeons can control their size by folding them. 4,6,11 Moreover, surgeons are able to choose hamstring tendons as the suitable autograft when they must reconstruct joints other than the knee, such as the elbow or ankle joint. 16,22,45 Thus, the use of hamstring autografts has become increasingly popular in ligament reconstruction surgery.
When a primary ACLR is performed at our institution, only semitendinosus (ST) grafts are harvested, halved for the double-bundle graft, and folded into 2 strands. The gracilis tendon (GT) is preserved as much as possible in preparation for future revision reconstructions 27,40 or other ligament reconstructions such as medial collateral ligament, 21 patellofemoral ligament, 12,23,42 or multiple ligament 8,13,44 injuries. Although hamstring autografts are reportedly preferable for ACLR, harvested hamstring tendons may be of insufficient length and diameter because of the patient’s anthropometrics and the technique used by the surgeon. ∥ Inadequate harvested tendon size will make the graft diminutive. Hence, surgeons need to reconsider how to organize the diminutive graft intraoperatively by augmentation, changing of graft source, or surgical procedure (double- to single-bundle technique) since a smaller diameter is associated with lower strength transplanted grafts and reconstruction failure. 5,11,25,26,28,32 If surgeons can predict hamstring autograft size, they will be able to conduct preoperative planning more carefully.
Most previous studies have aimed to elucidate graft size prediction in ACLR using 4-strand ST or gracilis grafts, and anthropometric parameters were available to predict hamstring autograft size. ¶ According to previous data of a single regression model using anthropometrics, the reproducibility of predicting the graft size appears not high. 4,47,52 Few studies have been designed to predict 2-strand grafts in double-bundle ACLR using the ST. The current study aimed to evaluate whether a patient’s preoperative anthropometric characteristics can be used to similarly predict 2-strand graft size in double-bundle ACLR using ST. Additionally, as a novel factor, we evaluated whether skeletal radiographic parameters predict ST graft size. Our hypothesis was that both anthropometric and radiographic parameters can be used to predict graft size in our double-bundle procedure and that radiographic parameter improves graft size prediction accuracy.
Methods
A total of 208 patients underwent primary double-bundle ACLR with an autologous hamstring tendon graft at our institution between April 2010 and April 2015. When the harvested ST was less than 230 mm or the 2-strand graft diameter was less than 5.0 mm, the GT was additionally harvested and augmented to the anteromedial bundle (AM) graft. In the current series, 6 patients were augmented by GT. Eight patients were not enrolled in the study because of insufficient data. Ultimately, 200 patients (87 men and 113 women) who underwent ACLR using the ST participated in this study. Anthropometric characteristics such as height and weight were obtained from the medical and surgical records. Tegner activity score was also obtained. Leg length and thigh circumference were not recorded since these parameters were less accurate indicators of graft dimensions, compared with height. 10,36,47 Each patient was informed of the current study’s aims and risks, and all agreed to participate. The ethical committee of our hospital approved this study.
Radiographic Measurements
Radiographs in the current study were obtained by experienced radiologic technicians with a film-focus distance of 130 cm, 60 kV, 200 mA, and 50 ms. The weightbearing anteroposterior knee radiographs were obtained with the knee fully extended and rotated, with the patella in the center of the femoral condyle. The beam was aligned relative to the joint space and positioned parallel to the floor with no angle. The distance between the medial and lateral femoral epicondyles (interepicondylar distance [IED]) was measured on the anteroposterior radiograph. The tibial plateau width (coronal tibial width [CTW]) was also measured (Figure 1). In addition, the femorotibial angle (FTA) was measured by the axis of the femoral and tibial shafts.
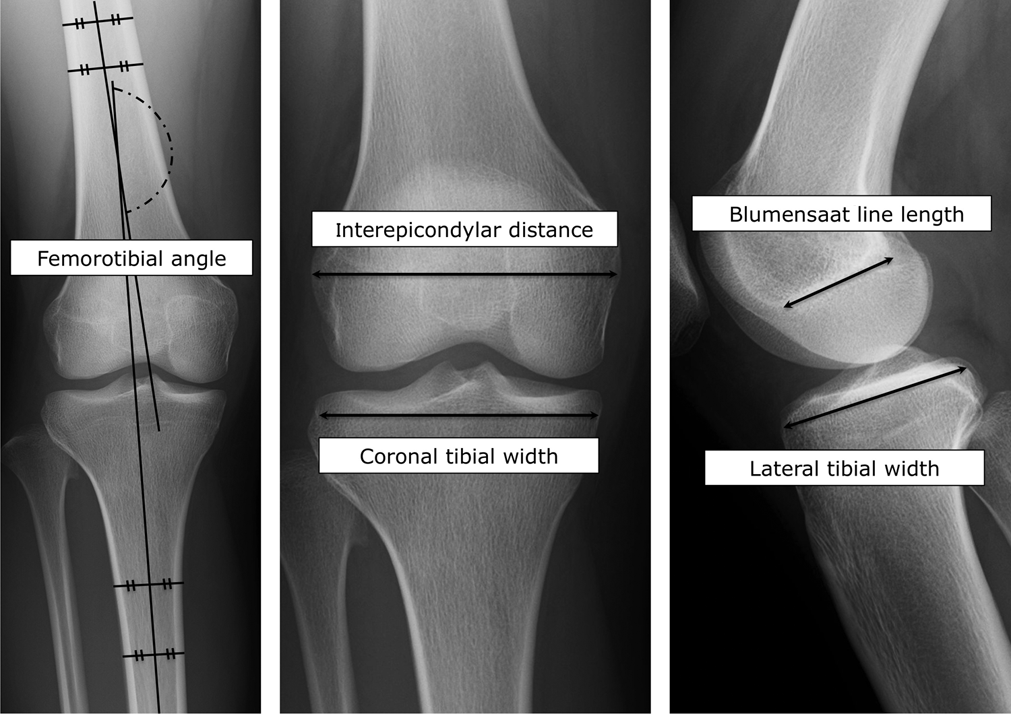
Radiographic evaluation of the skeletal parameters. The tibial plateau size was measured at the level of the subchondral bone. The Blumensaat line was measured as the line connecting its anterior and posterior edges.
The lateral knee radiographs were obtained with the knee flexed at 55°. The beam was aligned relative to the joint space and angled 5° caudally. On the lateral radiograph, the Blumensaat line length (BLL) and tibial plateau length (lateral tibial width [LTW]) were measured (Figure 1). Tibial plateau size was measured at the level of the subchondral bone. Blinding the information of graft dimension, all the radiographic parameters were measured by a single orthopaedic surgeon (9-year career) in our hospital using a picture archiving and communication system; the intrarater reliability (intraclass correlation [1, 1]) was 0.965 for IED, 0.932 for CTW, 0.891 for BLL, and 0.924 for LTW.
Intraoperative Graft Preparation and Evaluation
The ST graft was harvested through an anteromedial incision over the attachment of the pes anserinus on the tibial side. The insertion of the ST was sharply elevated off of the tibia along with periosteum. The proximal tendon was then harvested with a closed tendon stripper. Proximal muscle fibers and adipose tissue around the harvested tendon were removed. The total graft length (GL, mm) of the removed tendon was measured from end to end in 10-mm increments using a ruler (Figure 2A).

Evaluation of graft lengths and diameter. (A) Evaluation of graft length of the semitendinosus tendon. (B) Overview of the 2-strand graft. (C) Evaluation of the 2-strand graft diameter; measurements were calculated from the end of the femoral socket (2-strand graft was passed through the cylindrical device in the direction indicated by the arrow).
The harvested tendon was cut at its midpoint, stitched with a nonabsorbable suture at both ends, and folded to create the 2-strand graft (Figure 2B). The graft diameter (GD, mm) of the 2-strand graft was measured at the folded end in 0.5-mm increments using a cylinder device (Figure 2C), and the folded end was inserted into the femoral socket. The GD of the stitched end was measured in the same manner, and the stitched end was inserted into the tibial socket. In this study, the GD of the folded end was applied since the stitched end was increased in diameter because of the suture. 52 Finally, the GD was measured as the mean value of the femoral socket AM and posterolateral (PL) grafts.
Statistical Analysis
Statistical analyses were performed using SPSS version 22.0 (SPSS Inc). An unpaired t test was used to compare mean continuous values between men and women. The relationship between the GL or GD and anthropometric and radiographic parameters was investigated using the Pearson correlation coefficient. To establish the equation for predicting the graft dimension, single and multiple regression analyses were used with the GL or GD as the dependent variable and with anthropometric and radiographic parameters as independent variables in each regression. The stepwise selection method of the multiple regression analyses was used for determining significant predictor variables. Values of P < .05 were considered statistically significant.
Results
The mean GL was 258.9 ± 21.9 mm, and the mean GD was 5.8 ± 0.5 mm. Mean age, height, weight, body mass index, IED, CTW, BLL, LTW, GL, and GD were significantly higher in males than in females (Table 1). GL was positively correlated with height, weight, Tegner activity score, IED, CTW, BLL, and LTW. Of these parameters, height had the highest coefficient (r = 0.588) and was moderately correlated with GL. GD was positively correlated with height, weight, Tegner activity score, IED, CTW, BLL, and LTW. Of these parameters, height and IED had the highest coefficients but again were only moderately correlated with GD. The correlation coefficients of weight and IED were higher in GD than in GL (Table 2).
Demographic and Radiographic Data a

a AM, anteromedial bundle; BLL, Blumensaat line length; BMI, body mass index; CTW, coronal tibial width; FTA, femorotibial angle; GD, graft diameter; GL, graft length; IED, interepicondylar distance; LTW, lateral tibial width; PL, posterolateral bundle.
bP < .05 compared with females.
Statistical Analysis: Pearson Correlation (r) Between Graft Size and Demographic and Radiographic Data a

a AM, anteromedial bundle; BLL, Blumensaat line length; BMI, body mass index; CTW, coronal tibial width; FTA, femorotibial angle; GD, graft diameter; GL, graft length; IED, interepicondylar distance; LTW, lateral tibial width; PL, posterolateral bundle.
bP < .05.
cP < .01.
Single regression analysis showed a significant relationship between GL and sex, height, weight, Tegner activity score, IED, CTW, BLL, and LTW. In these parameters, height (R 2 = 0.342; B = 1.601; β = 0.588; P < .001) was most predictive of GL. Additionally, GD was significantly correlated with sex, height, weight, IED, CTW, BLL, and LTW. IED (R 2 = 0.207; B = 0.030; β = 0.460; P < .001) was most predictive of GD. Stepwise multiple regression analysis determined sex, height, and age as significant predictor variables of GL. This multiple regression model slightly improved the accuracy of accounting for GL, from 34.2% to 38.4% (R 2: from 0.342 to 0.384). Similarly, stepwise multiple regression analysis determined IED and height as significant predictor variables of GD. This multiple regression model also showed slight improvement in the accuracy of accounting for GD, from 20.7% to 22.4% (R 2: from 0.207 to 0.224) (Table 3). The multiple regression model showed the following formulas to predict GL or GD:


Multiple Regression Model for Graft Size Prediction a
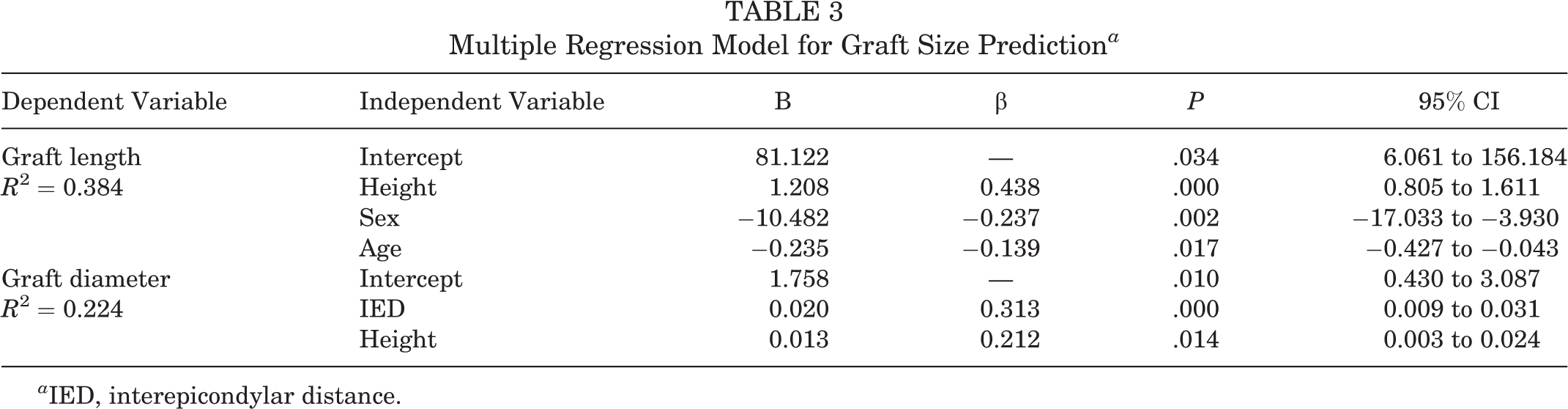
a IED, interepicondylar distance.
Discussion
To our knowledge, the current study is the first to derive a regression equation to predict harvested GL and 2-strand GD from anthropometric and radiographic parameters in double-bundle ACLR with ST tendon. The univariate regression model showed that height most accurately predicted GL, while the radiographic parameter (IED) predicted GD more accurately than height. Nevertheless, both parameters had only modest R 2 values. The stepwise multivariate regression model showed that height, sex, and age comprehensively predicted GL, and this model slightly improved the accuracy of predicting GL compared with that of the univariate regression model (R 2: from 0.342 to 0.384). Additionally, height and IED on the coronal radiograph also predicted GD comprehensively with slightly improved accuracy (R 2: from 0.207 to 0.224). According to the multiple regression model and our criteria for additional harvesting GT, 40 (1) height <150 cm, (2) female sex, and (3) patients aged ≥30 years were at risk of having a GL <230 cm, whereas patients who (1) have an IED <70 mm and (2) are <150 cm in height were also at risk of having a GD <5.0 mm.
In relation to the multiple regression model for GL, aging may affect the collagenous degeneration and the fragility of the harvested graft. Thus, the harvested ST tended to be shorter in older patients. The mean harvested GL of the ST was similar that of Chinese patients. 52 Previous studies have shown that the GL of white patients was longer than that of Chinese patients. 4,47,52 Including our data, Asians have a more diminutive graft size than whites because of physical size differences. According to the regression models in previous studies 4,47,52 as well as the present study, anthropometric factors can predict graft dimensions in both Asian and white populations. 4,47,52 However, comparing the coefficient of determination (R 2) in both races, the regression model was able to predict the graft dimensions more accurately in whites (maximum R 2 in GL, 0.48; maximum R 2 in GD, 0.41) 47 than in Asians (maximum R 2 in GL, 0.37; maximum R 2 in GD, 0.22). 4,52 Thus, racial differences may enable the prediction of graft dimensions according to physical size. Otherwise, anthropometric factors may predict graft dimensions more effectively in patients who have longer or larger skeletal structures.
To our knowledge, little research has been conducted to determine whether radiographic parameters can predict the harvested graft size of the hamstring tendon. The current data show that radiographic parameters are able to predict ST graft length and 2-stranded GD. It is noteworthy that radiographic parameters predicted GD more accurately than anthropometric parameters. Thus, radiographic parameters should be included for predicting ST graft size. Additionally, most previous studies did not mention whether multivariate regression analysis were able to predict GD more accurately. In the current study, the multivariate regression model slightly but significantly improved the accuracy of GD prediction. With regard to our multivariate regression model, both height and IED were selected as significant predictor variables of GD. Future studies can be carried out to predict GD more accurately by combining various parameters in patients who undergo ACLR using hamstring autografts.
Several limitations of the current study must be emphasized. First, only plain radiographs were used for the skeletal measurements, whereas computed tomography or magnetic resonance imaging scans can evaluate skeletal structures in 3 dimensions. In addition, FTA evaluation is more valid when performed using long-standing radiograph. More detailed skeletal evaluations may improve GD predictions. Second, the graft size was affected by surgical skill, and the ST was harvested by several different surgeons. 32,34,38,46,47,52 Third, the GD was measured by a ready-made cylindrical device that could make measurements in only 0.5-mm increments. Finally, the GL was measured and recorded in 10-mm increments. Despite these limitations, the current study has described a novel method for predicting graft dimensions using anthropometric data and skeletal parameters on a plain radiograph. Future studies warrant detailed mechanisms to predict the GD from the aspect of skeletal morphology.
In summary, the univariate regression model demonstrated that both preoperative anthropometric data and skeletal parameters on a plain radiograph could be used to predict GL and 2-strand graft diameter during primary double-bundle ACL reconstruction using ST. Use of the multivariate regression model slightly improved the GD prediction.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the ethical committee of Hirosaki University Hospital.