
Abstract
Background:
There are limited data on the incidence of concussion and concussion symptom nondisclosure among collegiate women’s ice hockey athletes.
Purpose:
To determine the incidence of sports-related concussion (SRC) in National Collegiate Athletic Association (NCAA) women’s ice hockey athletes.
Study Design:
Descriptive epidemiology study.
Methods:
An anonymous online survey was completed by 459 NCAA women’s ice hockey athletes. Players reported diagnosed concussions as well as incidents where they experienced an impact or blow to the head followed by symptoms associated with a concussion; reports spanned the duration of the 2014-2015 season and throughout players’ organized hockey career.
Results:
About half (n = 219, 47.7%) of respondents reported at least 1 diagnosed concussion over the duration of their entire organized ice hockey career. A total of 13.3% (n = 61) of respondents reported a diagnosed concussion during the 2014-2015 season. The incidence rate was 1.18 (95% CI, 0.92-1.51) per 1000 athlete-exposures to a game or practice and 0.58 (95% CI, 0.45-0.74) per 1000 hours of ice time. One-third (34.2%, n = 157) of players reported at least 1 impact where they experienced concussion-like symptoms during the 2014-2015 season; 82.8% of these players reported that they continued to play after at least 1 of these impacts, and 66.8% of players reported at least 1 impact where they never disclosed any symptoms.
Conclusion:
There is a high incidence of SRC in collegiate women’s ice hockey and a concerning level of symptom nondisclosure. Additional research is needed to understand the causes of concussion and reasons for the lack of symptom disclosure, including factors specific to female athletes and contextual issues specific to women’s collegiate ice hockey.
In sports that involve contact or collision, sports-related concussions (SRCs) are now recognized as a potentially serious injury among both male and female athletes. 18,39 A concussion is defined as a pathophysiological process that affects the brain and is caused by a direct blow to the head or neck or a jarring force, such as during a whiplash injury. 18 A concussion may result in rapid or delayed onset of symptoms that resolve spontaneously over time and may or may not involve loss of consciousness. 18 Thus, SRCs are often difficult to diagnose, as there is a dependence on the athlete to disclose his or her symptoms, which may be nonspecific. Incidence of diagnosed SRCs in the United States has risen rapidly over the past 2 decades, from an estimated 300,000 reported concussions per year in 1998 to 1.6 to 3.8 million reported concussions in 2006. 17,30 Recent estimates of SRC incidence rates (IRs) from 2009 to 2014 in sports participating in the National Collegiate Athletic Association (NCAA) indicate that, while the overall incidence of concussion across all sports has remained steady, incidence continues to increase within individual sports such as men’s football, men’s ice hockey, and women’s ice hockey. 39
Women’s ice hockey was officially added to the NCAA in the 2000-2001 season and is one of the fastest growing sports at the collegiate level, increasing from 63 programs with a total of 1380 athletes in its inaugural season to 91 programs and 2175 athletes in the 2014-2015 season. 8 The sport continues to evolve rapidly as the player pool increases in both number and skill. Participation at the high school level has also increased significantly over this time period, allowing for further development of the sport at the collegiate level. 23,24
Both men’s and women’s ice hockey are recognized as physical, high-speed sports with significant collision and concussion potential. The greatest difference between men’s and women’s ice hockey is body checking. Deliberate body checking, a motion using the trunk of the body (hips and shoulders) to force or separate an opponent from the puck, is not allowed in women’s ice hockey at any level of competition. However, incidental and legal body contact remains a frequent occurrence and is defined by USA Hockey as “contact that occurs between opponents during the normal process of playing the puck, provided there has been no overt hip, shoulder, or arm contact to physically force the opponent off of the puck.” 25,32 Such contact places women’s ice hockey athletes at risk for injuries, and particularly head injuries. Several studies have indicated that even in the absence of deliberate body checking, player-to-player contact was the cause of approximately 50% of concussions in game situations in women’s hockey. 1,2,29,36
Collegiate men’s and women’s ice hockey have two of the highest concussion IRs among collegiate sports, along with men’s football and wrestling. 39 A recent epidemiologic study using data collected from the NCAA injury surveillance program during 2009-2014 indicates that women’s ice hockey has the highest concussion IR across all collegiate female sports (7.50 [5.91-9.1] concussions per 10,000 athlete-exposures [AEs]). 39 However, utilization of the NCAA injury surveillance program to calculate IRs has limitations, as participation in the system is voluntary at the institutional level. Fewer than 20 colleges and universities that sponsor women’s ice hockey participated in data collection in the 2013-2014 season. 22 It is possible that attention to concussion safety, and potentially concussion IRs, are different at schools that do and do not participate in this injury surveillance program. Another limitation of the NCAA surveillance program is the criteria for reported injury. In order to report an injury, it must be a direct result of participation in organized intercollegiate practice or competition, require medical attention by a team athletic trainer or physician, and result in restriction of the participation of the student athlete for 1 or more days beyond the day of injury. 22 Therefore, undisclosed injuries or any incidents where a player is put back into play after evaluation by the medical team are not included in the injury surveillance data. Outside of NCAA surveillance data, there is little published literature on the incidence of head injuries and concussions in women’s ice hockey, potentially because of the newness of the sport. As a result, there is a lack of knowledge on the incidence, risk factors, and consequences of both diagnosed and undisclosed symptoms of SRC in collegiate women’s ice hockey.
A growing number of studies suggest that many concussions are not disclosed. 6,11,20 Previous research that assessed concussion symptom nondisclosure has used survey-based methodology, asking athletes whether they believed they had experienced a concussion or a given set of postimpact symptoms that may indicate a concussion, but chose not to disclose the incident to a coach or medical provider. 10,15 A recent study showed that athletes who do not immediately disclose concussion symptoms and continue to participate in practice or competition are at risk for a longer recovery when compared to athletes who immediately disclose their symptoms. 3 While rare, death can occur as a direct result of brain trauma in sport if an athlete sustains an additional impact during a period of heightened neurologic vulnerability after an initial injury. 4,34 No studies to date have assessed the rate of nondisclosure of concussion symptoms in collegiate women’s ice hockey. Prior literature has found a higher concussion IR among males as compared with females in rule-matched sports, but it has also found a higher rate of intention to disclose concussion symptoms among female athletes. 9,21,31 However, intention to disclose may only explain a small fraction of the variability in player behaviors. 12 Consequently, there is also a need to understand the extent to which these athletes are choosing not to disclose concussion-like symptoms.
The purpose of this study was twofold. First, we aimed to assess the incidence of concussions among NCAA women’s ice hockey players, and second to determine the incidence of undisclosed impacts followed by concussion-like symptoms in this population. We hypothesized that the incidence of concussions is higher than previously reported in the literature and that many concussion-like symptoms are not disclosed. Achieving a greater understanding of how frequently concussions occur, and the characteristics of players who experience potentially concussive symptoms but choose not to disclose them, may help determine a course of action to reduce the burden of SRC in women’s ice hockey.
Methods
Sample and Procedure
This study was reviewed by our institutional review board and received exempt status. Survey distribution and data collection occurred in November and December 2015. Inclusion criteria were females actively rostered on a varsity NCAA ice hockey team and older than 18 years. A recruitment email was sent to the head coach and athletic director of all NCAA participating colleges and universities with a varsity women’s ice hockey program. A total of 98 women’s ice hockey programs were contacted through email. The athletic director and head coach were asked to allow their athletes to participate in the voluntary study survey. A total of 50 programs (51%) agreed to participate, and head coaches emailed an online survey to all players actively rostered on their varsity team. In order to increase the response rate, one follow-up email was sent to head coaches to remind athletes to complete the survey. NCAA participation estimates for the 2014-2015 season indicated an average of 23.9 players per team, therefore, approximately 1200 players were sent a link to the survey. 8 Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted by Partners HealthCare Research Computing, Enterprise Research Infrastructure & Services (ERIS) group. REDCap is a secure, web-based application designed to support data capture for research studies. 7
Measures
Our primary outcome of interest was history of diagnosed concussion. Participants were asked to report any history of concussion that was diagnosed by a medical professional. This was assessed for 2 time periods: (1) in the 2014-2015 ice hockey season, and (2) at any time during the player’s organized ice hockey career. To quantify career length, players were asked to report the length of their organized ice hockey career in years. If the participant reported a diagnosed concussion in the past season, she was prompted to answer questions that asked about the timing of the injury, mechanism, and setting (see the Appendix).
Nondisclosure of Concussion-like Symptoms
As a secondary analysis, we assessed the history of an impact or blow to the head followed by symptoms as a proxy for incidence of potentially concussive symptoms that require evaluation by a medical professional. Participants were asked if they experienced an impact or blow to the head during play followed by any of a list of symptoms commonly associated with a concussion (see the Appendix). Participants were then asked how many times they experienced an impact or blow to the head followed by such symptoms during 2 time periods: (1) the 2014-2015 hockey season, and (2) any time during their hockey career.
Players who reported an incident where they experienced concussion-like symptoms were prompted to answer questions about symptom disclosure. Players were first asked if they had continued to play in a practice or game after experiencing concussion-like symptoms. They were then asked to report the number of occasions where they eventually disclosed their symptoms to a medical professional, coach, or teammate, or if they never disclosed their symptoms.
Statistical Analysis
We calculated the incidence of diagnosed concussion and impacts or blows to the head followed by concussion symptoms as the percentage of respondents answering affirmatively to each question. For the 2014-2015 season, we assessed IRs utilizing 2 methods. First, we assessed the IR of diagnosed concussions over the 2014-2015 NCAA season by calculating the number of concussions over AEs. An AE is defined as 1 athlete competing in 1 practice or game over a given period of time. 39 We assumed there were approximately 6 AEs per week over a 20-week season for NCAA Division II and III players and a 24-week season for Division I players and multiplied the number of athletes participating while considering their school’s division in order to get the total number of AEs across the season. We additionally examined the IR of diagnosed concussions and blows to the head followed by concussion symptoms by calculating the number of events over person-time at risk. Person-time at risk was estimated from the player-reported number of hours spent on the ice for games or practices, assuming a 20-week season for players in Division II and III and a 24-week season for players in Division I.
Next, we evaluated the association between diagnosed concussion and the covariates player position, year in school, and NCAA division. We used the dichotomous outcome of players diagnosed with a concussion in the 2014-2015 NCAA season. The chi-square test was used for univariate analysis. To simultaneously evaluate all covariates, we used multivariable logistic regression for the concussion outcome. We repeated this analysis to evaluate the association between concussion symptom disclosure and covariates, using the dichotomous outcome of whether the player had ever failed to disclose concussion-like symptoms. For this analysis, we included only players reporting an incident where they experienced symptoms associated with a concussion in the 2014-2015 NCAA season. As the incidence of symptom nondisclosure was quite high, odds ratios from logistic regression may overestimate the true effect size, so we used a multivariable modified Poisson regression to evaluate the association between nondisclosure and covariates. 38
Results
A total of 459 athletes completed the survey, for a response rate of 38.3%. Table 1 shows the general demographic profile of participating athletes.
Demographic Profile of Respondents (N = 459) a
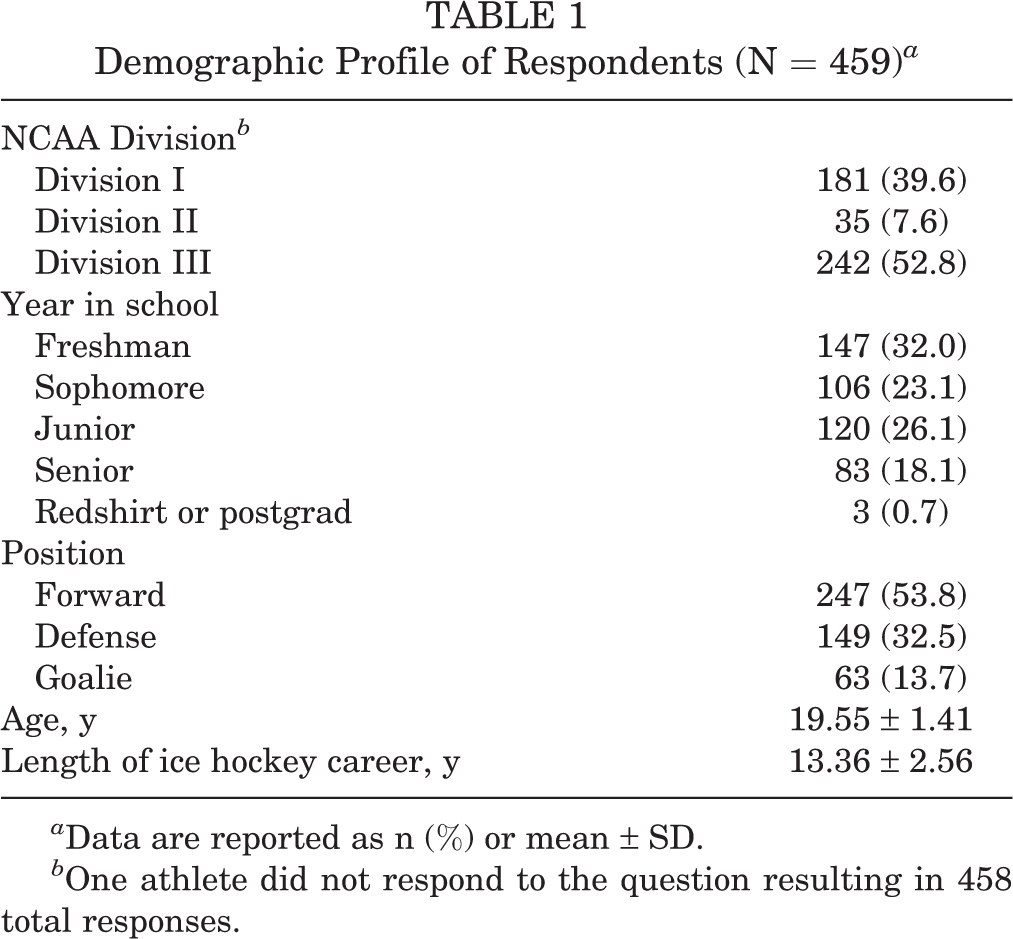
a Data are reported as n (%) or mean ± SD.
b One athlete did not respond to the question resulting in 458 total responses.
In the 2014-2015 season, 13.3% (n = 61) of players reported a total of 70 concussions that were diagnosed by a medical provider. There were a total of 59,304 AEs throughout the 2014-2015 season, for an IR of 1.18 (95% confidence interval [CI], 0.92-1.51) per 1000 AEs. IR was also calculated by hours of ice time per season. Diagnosed concussions occurred during an estimated 119,216 hours of ice time over the duration of the 2014-2015 season, resulting in an IR of 0.58 (95% CI, 0.45-0.74) per 1000 hours of ice time. The number of diagnosed concussions reported in the 2014-2015 season ranged from 1 to 3 (Table 2).
Number of Diagnosed Concussions During the 2014-2015 NCAA Season and the Organized Ice Hockey Career a

a NCAA, National Collegiate Athletic Association.
Diagnosed concussions over the 2014-2015 season were more likely to occur during the regular season (P < .001), in a game setting (P < .001), and as a result of player-to-player contact (P = .006) (Table 3). There were no significant associations between player division, player position, or player year and diagnosed concussion (Table 4).
Results of Chi-Square Test for Timing, Setting, and Mechanism of Injury for Diagnosed Concussions Reported in the 2014-2015 NCAA Season a
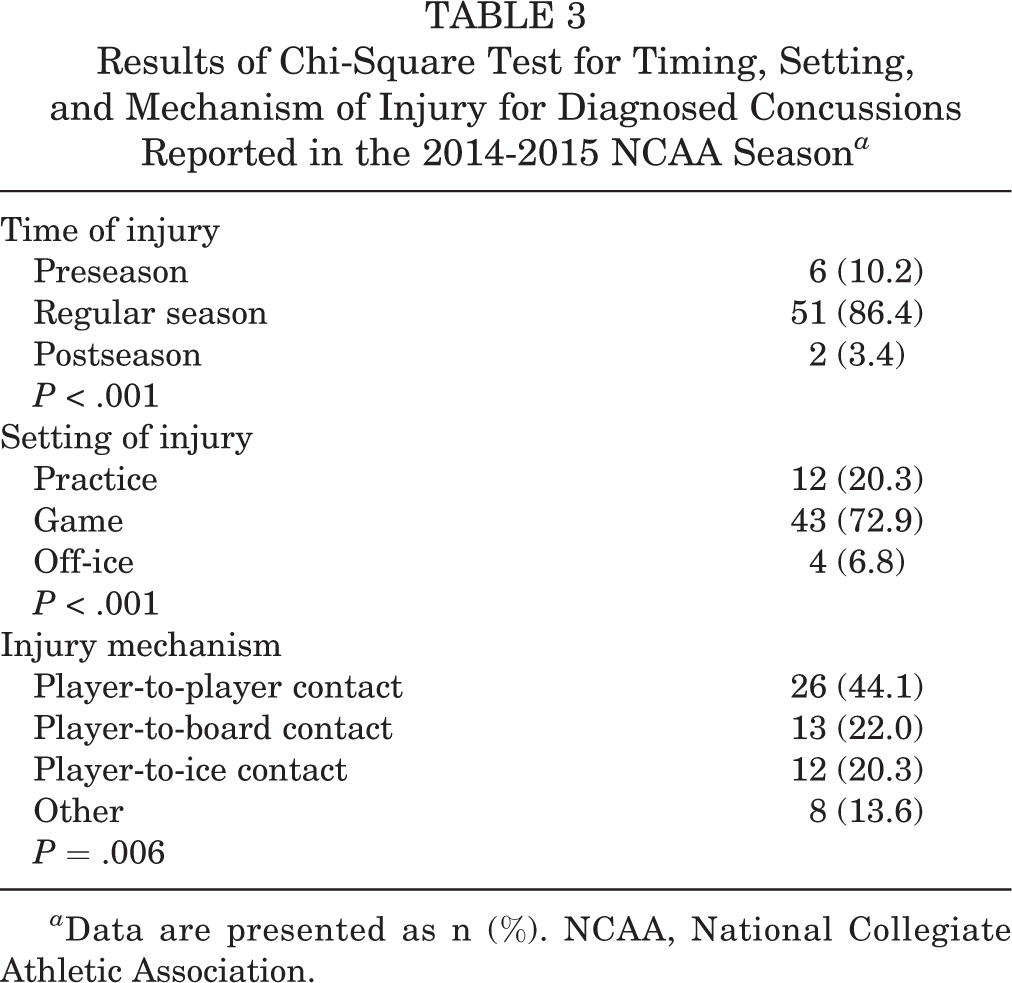
a Data are presented as n (%). NCAA, National Collegiate Athletic Association.
Association Between Player Covariates and Concussion Incidence, and Concussion Symptom Disclosure in the 2014-2015 NCAA Season a

a Significant results are given in boldface. Data are presented as n (%). NCAA, National Collegiate Athletic Association.
b Chi-square test.
c Logistic regression.
d Modified Poisson regression.
The average reported length of the organized ice hockey career was 13.36 ± 2.56 years. Overall, 47.7% (n = 219) of players indicated that they had a history of at least 1 concussion that was diagnosed by a medical provider over the duration of their organized ice hockey career. The number of diagnosed concussions throughout the total ice hockey career ranged from 1 to more than 5 (Table 2).
In the 2014-2015 season, 34.2% (n = 157) respondents reported having sustained an impact or blow to the head followed by concussion-like symptoms. The number of incidents reported ranged from 1 to more than 5 (Table 5). Incidents of a blow to the head followed by concussion symptoms occurred 295 times over 118,080 hours of ice time in the 2014-2015 season, for an IR of 2.50 (95% CI, 2.1-2.97) per 1000 hours of ice time. Overall, 70.5% (n = 324) of respondents reported sustaining a blow to the head followed by symptoms associated with a concussion throughout the duration of their ice hockey career. The number of incidents ranged from 1 to more than 5 (Table 5).
Number of Occasions Where Concussion Symptoms Were Experienced During the 2014-2015 NCAA Season and the Organized Ice Hockey Career a

a NCAA, National Collegiate Athletic Association.
Of the 157 respondents reporting at least 1 occasion where they experienced concussion-like symptoms, 82.8% (n = 130) reported that they continued to play despite the symptoms. Of those who reported at least 1 occasion of symptoms in the 2014-2015 season, 66.8% (n = 105) reported that there was at least 1 incident where they never told a coach or medical provider about their symptoms. Nondisclosure of concussion-like symptoms was associated with player position in both univariate (P = .033) and multivariable (P = .018) analysis. There were no significant associations between nondisclosure and year in school or division, in either univariate or multivariable models (Table 4).
Discussion
The primary aim of the present study was to determine the incidence of diagnosed SRC among NCAA women’s ice hockey athletes. A secondary aim was to determine the incidence of concussion-like symptom nondisclosure and to identify whether there are any specific player factors that are more or less likely to disclose symptoms. During the 2014-2015 season, 13.3% of respondents reported that they were diagnosed with concussion by a physician or athletic trainer, for an IR of 1.18 (95% CI, 0.92-1.51) per 1000 AEs. Previous estimates using the NCAA injury surveillance system found an IR of 0.75 to 0.82 diagnosed concussions per 1000 AEs. 2,39
Calculating an IR using AE methodology does not consider the length in hours of the practice or game. For this reason, we calculated IR as a function of hours spent on the ice in practices or games, as reported by players. This yielded an IR of 0.58 (95% CI, 0.45-0.74) concussions per 1000 hours of ice time. When considering IR calculations, it is important to note the limitations of methodologies used, as incidence calculated by the number of practices or games participated in (AEs) would be higher than the rate as calculated by the number of hours, since many practices or games span across multiple hours. In addition, conveying IRs to the general population of athletes, coaches, and parents may be less accessible when using AE terminology, where hours of playing time is more pertinent. Further research should be conducted to determine which approach to reporting IR is most accurate and accessible.
Studies using the standard AE methodology have reported that the rates of concussion for men’s and women’s ice hockey are similar, with one study reporting an IR of 0.53 (0.21-0.85) per 1000 AEs for men, and 0.58 (0.29-0.87) per 1000 AEs for women. 33,39 The present study found an IR of 1.18 (0.92-1.51) per 1000 AEs, indicating that the incidence of concussion may be higher than previously estimated and higher than previously reported estimates for men’s ice hockey. 39 Ice hockey is unique in the broader context of gendered sports, as the rules differ by sex with regard to intentional body checking. However, one limitation of this comparison lies in the methodologies used to collect data. Previous studies utilized the NCAA injury surveillance program to collect data, while the present study used a survey-based methodology.
Our results indicate that concussions in women’s ice hockey occur more frequently in game settings versus practice settings (P < .001) and were more likely to occur in the regular season compared with pre- or postseason play. The results are consistent with several prior studies examining concussion incidence patterns in ice hockey at the collegiate level, which indicated that more concussions occurred in a game setting when compared with a practice or off-ice setting. 1,35,39 Agel and Harvey 2 reported that the rate of overall injuries was higher in a game setting than in a practice setting for collegiate ice hockey. More broadly, there have been relatively consistent findings of higher concussion incidence during games as compared with practice in other women’s collision sports and in male collision sports. 39 Possible reasons for this difference may include the intensity of a game setting resulting in higher velocity collisions, coaches intentionally restricting game-like play during practices, or for schools with fewer resources, the absence of an athletic trainer or physician who may help facilitate concussion identification at practices.
Our results indicated that player-to-player contact was the mechanism of injury for 44.1% of the reported concussions in the 2014-2015 NCAA season. Player-to-player contact was the most common mechanism of injury compared with player-to-board or player-to-ice contact (P = .006). In the NCAA injury surveillance data reported by Zuckerman et al, 39 49.4% of women’s ice hockey concussions were associated with player-to-player contact. Additionally, a recent cohort study reported that 50% of head impacts were caused by player-to-player contact in Division I women’s ice hockey. 36 The same study found that 50.4% of head impacts in male hockey players were caused by contact with another player. 36 This is especially intriguing because women’s ice hockey disallows deliberate player contact in the form of body checking, yet around half of diagnosed concussions seem to be occurring through a player-to-player mechanism. Additional research is needed to understand whether player-to-player head injuries in women’s ice hockey are occurring within the context of the existing rules or whether they are occurring when a player violates the rules with illegal contact. Understanding more about the nature and mechanism of these injuries may help suggest the appropriate level at which to intervene in order to reduce the incidence of concussion and other injuries related to this type of contact. For example, if concussions are occurring as a result of players’ violating existing rules, greater enforcement of rules by officials may be warranted.
A total of 47.7% of respondents reported having at least 1 concussion diagnosed by a medical provider over the course of their ice hockey career. While some short-term consequences of concussion have been noted in the literature, concern about the potential for long-term consequences, such as the development of chronic traumatic encephalopathy (CTE) has been heightened in the media. 16 Previous literature has reported an association between repetitive closed-head injuries and development of CTE, particularly in men’s football at the professional level. 19 No such connection has been established among women’s ice hockey players, in part because of the relative newness of the sport and thus a lack of prospective data of sufficient duration. However, given our findings, this population should not be ignored in future analyses of long-term consequences of head impacts and concussion.
The present findings indicate that nondisclosure of concussion-like symptoms is occurring at a concerning level in women’s ice hockey. Of those who reported at least 1 occasion where they felt concussion-like symptoms, 82.8% continued to play in the game or practice. Many of these players indicated there was at least 1 occasion where they never disclosed their symptoms to a medical provider, coach, or teammate. It is important to note that experiencing concussion-like symptoms after an impact does not always indicate that a concussion has occurred. However, medical personnel must make this determination and not the athlete, and thus any impact followed by concussion-like symptoms should be reported. Continuing to play and possibly sustaining a second blow to the head after an initial concussion has been shown to increase the magnitude of symptoms and delay recovery. 26,27,37 Thus, more research is needed to understand why so many female ice hockey players are continuing to play despite experiencing symptoms commonly associated with a concussion. Failure to disclose concussion symptoms may reflect a lack of awareness of the signs and symptoms of a concussion or the unwillingness of players to disclose symptoms. Research in other contact and collision sports indicates that factors related to willingness to disclose symptoms, such as team norms related to concussion reporting and player expectations about what will happen if they report symptoms, are among the most important determinants of symptom-reporting behavior. 5,13,15,28 The present findings suggest that efforts to understand symptom nondisclosure in female ice hockey players and develop educational programming are warranted. In addition, efforts to address factors in the sport environment that influence nondisclosure behavior (eg, pressure from coaches and parents) may be more effective than focusing on changing disclosure culture among athletes directly. 14
Limitations
Data were collected through a voluntary online survey, with 38.3% of eligible athletes choosing to participate. The survey was emailed from the head coach of the program to varsity women’s hockey players with the title of “Women’s Ice Hockey Concussion Survey,” and players who may have had prior experience with concussions or who were more concerned about concussion safety may have been more inclined to complete the survey. Thus, these athletes may not be representative of the total population of NCAA women’s ice hockey athletes. Furthermore, only 50% of coaches agreed to forward the recruitment email to their athletes. It is possible that participating coaches had different attitudes about concussion safety than nonparticipating coaches, and this may have made concussion incidence and disclosure behaviors nonequivalent on participating and nonparticipating teams. In addition, surveys were distributed approximately 7 months (November to December 2015) after the conclusion of the 2014-2015 NCAA season, which may have affected recall for incidents of concussion-like symptoms in particular.
Another limitation is that person-time was estimated from the average number of hours per week spent in practice and games. If a participant did not complete a full season due to injury or other reason, this was not reflected in the person-time or AE estimate. Because of the deidentified nature of the survey, we were unable to determine which players made it to postseason play; instead, we determined a set number of participating weeks depending on NCAA division. Therefore, the person-time and number of AEs is likely overestimated, and therefore we may be underestimating the true IR of concussion in collegiate women’s ice hockey. It is also important to note that the present study utilized a survey-based methodology, where players themselves reported a history of concussion, and it may be difficult to compare this method of data collection with previous literature utilizing the NCAA injury surveillance system data for IR calculations.
Conclusion
The present study indicates that despite rules prohibiting deliberate contact through body checking in women’s ice hockey, player-to-player contact is the most common injury mechanism for SRC, and the incidence of SRC is similar to that previously observed in men’s hockey. 39 The results of this study also raise the possibility that, as has been found in other contact and collision sports, there may be substantial nondisclosure of concussion-like symptoms that warrant medical evaluation. These findings suggest a need for greater research and program development focused on women’s ice hockey players. This includes evaluation of the effectiveness of the current NCAA rules and standards of play that disallow deliberate player contact through body checking. It also includes population-specific player education and/or contextual interventions to help ensure that women’s ice hockey players are seeking medical attention for all impacts that are followed by symptoms of a possible concussion.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: E.K. is a research consultant for the NCAA.
Ethical approval for this study was waived by the Partners Human Research Committee (Protocol #2014P001782/BWH).