
Abstract
Background:
Osteoarthritis (OA) currently affects 10% of the American population. There has been a recent push to determine exactly what causes OA and how it can be treated most effectively. Serum vitamin D levels have been associated with OA and may have an effect on articular cartilage remodeling.
Purpose:
To critically review the published research on the effect of vitamin D on articular cartilage and the development of OA as well as on the mechanism behind cartilage regeneration and degeneration.
Study Design:
Review.
Methods:
A systematic search of PubMed and the Web of Science was performed for relevant studies published in the English language through April 30, 2016, using the terms vitamin D, articular cartilage, and osteoarthritis.
Results:
On a molecular level, 1α,25(OH)2D3, the activated form of vitamin D, plays a role in articular cartilage degeneration. Vitamin D binds to vitamin D receptors, triggering a signaling cascade that leads to chondrocyte hypertrophy. In clinical trials, vitamin D deficiency poses a risk factor for OA, and those with decreased cartilage thickness are more likely to be vitamin D–insufficient.
Conclusion:
The role of vitamin D supplementation in the treatment or prevention of OA remains uncertain. More research is needed to reconcile these conflicting findings.
Osteoarthritis (OA) is the most common joint disorder in the United States. 50 While there are some theories of the pathogenesis of OA, the exact mechanism is not well defined. One promising theory suggests that repetitive mechanical stimulation of articular cartilage prevents it from regenerating properly, which ultimately leads to cartilage degeneration. When traumatized, articular cartilage produces an anabolic response; however, as chondral wear accrues over time, the anabolic response in the articular cartilage declines and the imbalance between chondrocyte synthetic activity and degradative activity leads to progressive thinning of articular cartilage. 10 Vitamin D has been associated with cartilage regeneration in OA, but the exact mechanism is not well defined. Vitamin D deficiency is associated with an increased risk of patients developing OA in some studies, but the results of other studies have been inconsistent. The purpose of this article was to summarize the role of vitamin D in articular cartilage physiology and OA and review the current literature that investigates the role of vitamin D in articular cartilage regeneration.
Osteoarthritis
Currently, symptomatic knee OA occurs in 10% of men and 13% of women aged 60 years or older. 50 According to the Centers for Disease Control and Prevention, 1 in 2 Americans may develop symptomatic knee OA by the age of 85 years. In the obese population, 2 in 3 Americans may develop symptomatic knee OA in their lifetime. As the American population ages and the number of obese Americans increases, the number of people affected with symptomatic OA is likely to increase. 20
To treat OA, various medical and surgical interventions can be performed to slow the progression of the disease but not cure it. For those with non inflammatory OA, acetaminophen is given as needed. For those with inflammatory OA, nonsteroidal anti-inflammatory drugs (NSAIDs) are given in both oral and topical form. If NSAIDs do not work, intra-articular corticosteroids are given. For those in which nonoperative management does not provide relief, surgery is suggested depending on which joint is arthritic. 20 There are currently no disease-modifying drugs available for clinical use. There are some clinical trials for disease-modifying drugs, but more research is needed to determine the pathogenesis of OA to better treat patients in the future.
Articular Cartilage
Articular cartilage can withstand routine mechanical stress produced by the human body. It is an avascular and aneural tissue that is made up of chondrocytes within an extracellular matrix consisting predominantly of type II collagen, proteoglycans, and aggrecans. Articular cartilage is heterogenous, and its material properties change as a function of depth. 50 Each layer contains a complex extracellular matrix made of proteoglycans, aggrecans, and type II collagen. The matrix is produced by chondrocytes, which are the only cells found in adult articular cartilage. 50 These cells are responsible for remodeling and maintaining the structural and functional integrity of the cartilage. 16 Chondrocytes in the superficial zone are densely packed cells that are oriented parallel to the articular surface. 5 Within this layer, type II collagen is oriented parallel to the articular surface, allowing for increased tensile strength. 5,8,26 Chondrocytes in the middle zone are round and are randomly distributed within the extracellular matrix, and chondrocytes in the deep zone are also round like those in the middle zone but form clusters. In the middle and deep zones, type II collagen is randomly distributed and oriented perpendicular to the articular surface, respectively, to allow for both layers to have compressive strength. 2 Of note, both of these layers have increased expression of matrix metalloproteinase (MMP)–13, MMP-9, and a bone morphogenetic protein (BMP) antagonist that is involved with BMP/transforming growth factor–β (TGF-β) signaling. 2
A variety of complex interactions occurs between the matrix and chondrocytes to maintain a fine balance between synthesis and degradation of articular cartilage. 1 The mechanisms that control the balance between these activities remain poorly understood, but cytokines with catabolic and anabolic effects appear to have key roles. 10 In response to various stimuli, chondrocytes anabolically secrete growth factors such as insulin-like growth factor I (IGF-I), TGF-β, and BMPs to stimulate matrix synthesis and chondrocyte proliferation. 33 IGF-1, in particular, stimulates protein and DNA synthesis, glucose uptake and oxidation, and synthesis and secretion of collagen type II and aggrecans. 33 TGF-β inhibits terminal differentiation of chondrocytes in the extracellular matrix, which ultimately blocks cartilage matrix calcification and vascularization in order to maintain extracellular matrix integrity. 53 Articular cartilage degradation involves a catabolic reaction that involves proteolytic degradation of the connective tissue matrix. 13 Interleukin-1 (IL-1), which is synthesized by chondrocytes and mononuclear cells lining the synovium, acts in multiple pathways to suppress the synthesis of type II cartilage and to promote the formation of type I cartilage. It induces catabolic enzymes such as stromelysin and collagenase and suppresses prostaglandin synthesis. 29 In addition, it acts with tumor necrosis factor–α (TNF-α) to inhibit synthesis. 33
Articular Cartilage and Osteoarthritis
Macroscopically, the earliest sign of articular cartilage degeneration is due to fibrillation of its superficial layers. 10 As the disease progresses, the superficial surface irregularities form clefts, the articular surface roughens, and the fibrillations extend deeper into the cartilage until the fissures invade the subchondral bone. 10,50 As the cartilage fissures deepen, the articular cartilage tears, and fragments are released into the joint space, leading to possible irritation. 10 Eventually, enzymatic degradation of the matrix decreases the cartilage, leading to loss of articular cartilage and ultimately the presentation of pain as a symptom of OA. 10,50
Articular cartilage degeneration in OA can be broken down into 3 stages: cartilage matrix damage, chondrocyte response to tissue damage, and decline of chondrocyte synthetic response and progressive loss of chondral tissue. 10 In the first stage, the matrix molecular framework is altered and water content increases. Two principal mechanisms are thought to initiate this stage. 41 In most patients, damage to normal articular cartilage occurs by physical forces; this can be due to a single event of macrotrauma or repeated microtraumas. 35 In response to these traumas, chondrocytes release degradative enzymes. In a smaller percentage of patients who have altered joint biomechanics, past inflammatory joint diseases, congenital abnormalities, or metabolic syndromes, genetically defective cartilage fails under normal joint loading, leading to OA. 40,50 On a microscopic level, articular cartilage loses proteoglycan aggregation and experiences swelling, which leads to hypertrophy. In an attempt to regenerate the extracellular matrix, chondrocytes increase synthesis of types II, IX, and XI collagen, aggrecan, and type IV collagen, which is associated with the formation of fibrillations, matrix depletion, cell clusters, 16 and loss of proteoglycans and cleavage of type II collagen that causes an increase in matrix content and leads to hypertrophy. 42
The second stage occurs when the chondrocytes detect the tissue damage and release mediators that stimulate a cellular response consisting of anabolic and catabolic activity and chondrocyte proliferation. 10 In response to this stress, proliferating chondrocytes surround the newly synthesized matrix molecules and release chemical mediators such as nitric oxide, which diffuses and can induce production of IL-1. 3 IL-1 is capable of inducing the expression of MMPs, aggrecanases, and other catabolic genes and cytokines such as A disintegrin and metalloproteinase with thrombospondin type 1 motif (ADAMTS)–4 and ADAMTS-5. 16 Expression of MMPs, especially MMP-13 and MMP-3, allows for the degradation of collagens II and IX and ultimately disruption of fibril function. 44 Expression of ADAMTS-4 and ADAMTS-5 causes cartilage degeneration. In experiments with mice with single knockout of the ADAMTS-5 gene or double knockout of the ADAMTS-4 and ADAMTS-5 genes, lack of these genes prevented cartilage degradation in surgically and chemically induced murine knee OA models. 51 IL-1 and TNF-α increase synthesis of prostaglandin E2 by stimulating the expression of cyclooxygenase 2, microsomal prostaglandin E synthase–1, and soluble phospholipase A2. In addition, IL-1 induces proinflammatory cytokines such as IL-6, leukocyte migration inhibitory factor (LIF), IL-17, IL-18, and IL-8. 16 The presence of fibronectin fragments or other molecules in the damaged articular cartilage further increases the production of IL-1 and molecules produced downstream of it. 10 As a result, chondrocytes undergo further phenotypic changes. Degradation of types IX and XI collagen and other molecules destabilize the type II collagen meshwork. 10 The superficial zone is disrupted, and loss of aggrecan due to enzymatic degradation increases the stress on the remaining collagen fibril network and chondrocytes. 10
The third stage occurs when the decline in the chondrocytic anabolic and proliferative response leads to progressive loss of articular cartilage. 10 Eventually, the articular cartilage’s anabolic response declines, and the imbalance between chondrocyte synthetic activity and degradative activity leads to progressive thinning of articular cartilage. 32 The thinning and ultimate loss of articular cartilage leads to the clinical syndrome of OA, characterized by joint pain and loss of joint function. 10
Vitamin D
Vitamin D deficiency affects 42% of the American population. 15 Specifically, people who live in northern regions of the United States and those who remain indoors are most prone to deficiency. 21 Once thought to cause solely rickets and decreased bone density, vitamin D deficiency has been associated with several chronic diseases such as multiple sclerosis, type I diabetes, and hypertension. 22
People receive the largest proportion of vitamin D from exposure to the sun. When sunlight hits the skin, the ultraviolet radiation turns 7-dehydrocholesterol to pre–vitamin D3. Pre–vitamin D3 is then converted into 25-hydroxyvitamin D3 by the liver. In the kidney, 25-hydroxyvitamin D3 reacts with 25-hydroxyvitamin D-1α hydroxylase to become 1,25 dihydroxyvitamin D3 (vitamin D). 22 It then enters the bloodstream, where it travels to tissues possessing vitamin D receptors (VDR) such as intestines, kidneys, bone, bone marrow, and chondrocytes. 21 When vitamin D binds to VDRs, the complex binds to vitamin D3 response elements (VDREs) in the promoter region of various target genes. 6,46 In particular, activation of VDRs results in the absorption of calcium to regulate the circulating levels of calcium and phosphate for normal mineralization of bone, both of which are also regulated by the parathyroid hormone. 14 Specifically, when the levels of blood calcium are low, the parathyroid gland releases parathyroid hormone, causing expression of proteins that leads to an increase in total body calcium levels. 43 In the kidney, parathyroid hormone induces the conversion of 25-hydroxyvitamin D to 1,25 dihydroxyvitamin D, which ultimately results in an increase in the transcription of genes responsible for calcium absorption. 43 When the parathyroid hormone is removed, vitamin D cannot function properly within the patient, resulting in hypercalcemia. In order for a patient to have adequate and efficient blood calcium levels, both vitamin D and parathyroid hormone must be present at sufficient levels and function together. 14 According to the National Institutes of Health, serum 25-hydroxyvitamin D concentrations should be greater than or equal to 20 ng/mL and less than or equal to 50 ng/mL. 38 Concentrations less than 12 ng/mL are deemed deficient and could lead to rickets in children and osteomalacia in adults. Concentrations between 12 and 20 ng/mL are considered inadequate for bone health in adults. Concentrations greater than 50 ng/mL may lead to deleterious health effects.
Vitamin D and Inflammation
Vitamin D is a key immunoregulator in the reduction of inflammation, and it has been shown to exert influence on T and B lymphocytes, macrophages, and dendritic cells. 18 VDRs are present in immune cells, and when vitamin D binds to VDRs, VDREs are activated. Activation of the VDREs in the promoter region of cytokine genes blocks transcription of nuclear transcription factors such as NF-AT (nuclear factor of activated T cells) and NF-κB. 18 This interference blocks the cellular response to TNF-α and IL-1 and allows for the upregulation of IL-10. 7 A recent study on vitamin D–deficient IL-10 knockout mice with inflammatory bowel disease showed that when mice were given vitamin D, their inflammatory bowel disease was mitigated due to the effect of vitamin D on TNF-α. 54 In a murine colitis model, increase in IL-10 production by 1,25(OH)2D3 allowed for Treg (regulatory T cells) induction. 12 Because of its anti-inflammatory nature, vitamin D is sometimes used as a medication for patients with chronic diseases such as rheumatoid arthritis, multiple sclerosis, and systemic lupus erythematous. 37 Further investigation, however, is needed to more fully understand the specific mechanisms by which vitamin D acts to reduce inflammation.
Vitamin D and Articular Cartilage
Recent evidence suggests that the role of vitamin D in the progression of OA is promising. Articular cartilage degenerates in OA patients due to a homeostatic imbalance in which catabolic processes overrule anabolic processes. As a result of this reaction, articular cartilage becomes hypertrophic and eventually deteriorates. Several studies have shown that VDRs are upregulated on damaged cartilage. Tetlow and Woolley 47 showed that VDR expression is increased in areas of erosion in patients with late-stage rheumatoid arthritis. The same research group 48 and Orfanidou et al 39 showed similar results in patients with OA. When vitamin D binds to VDRs, a signaling cascade effect occurs. Tetlow et al 48 demonstrated that chondrocytes expressed increased levels of MMPs 1, 3, and 9 in vivo. This leads to degradation of bone at increased rates. 30 VDRs also signal increase in fibroblast growth factor 23, caspase 9, and extracellular signal-regulated kinase 1/2. When VDR is inhibited, downregulation occurs. 39 The upregulation of vitamin D signaling in an arthritic joint is the body’s response to joint degeneration through an attempt to spread joint contact pressures through new bone formation in the form of osteophytes, but it is unclear whether this is a positive or ultimately detrimental response. Future research should aim to investigate the extent and severity of these actions and their implications on the development and progression of OA in relation to articular cartilage.
Vitamin D and Osteoarthritis
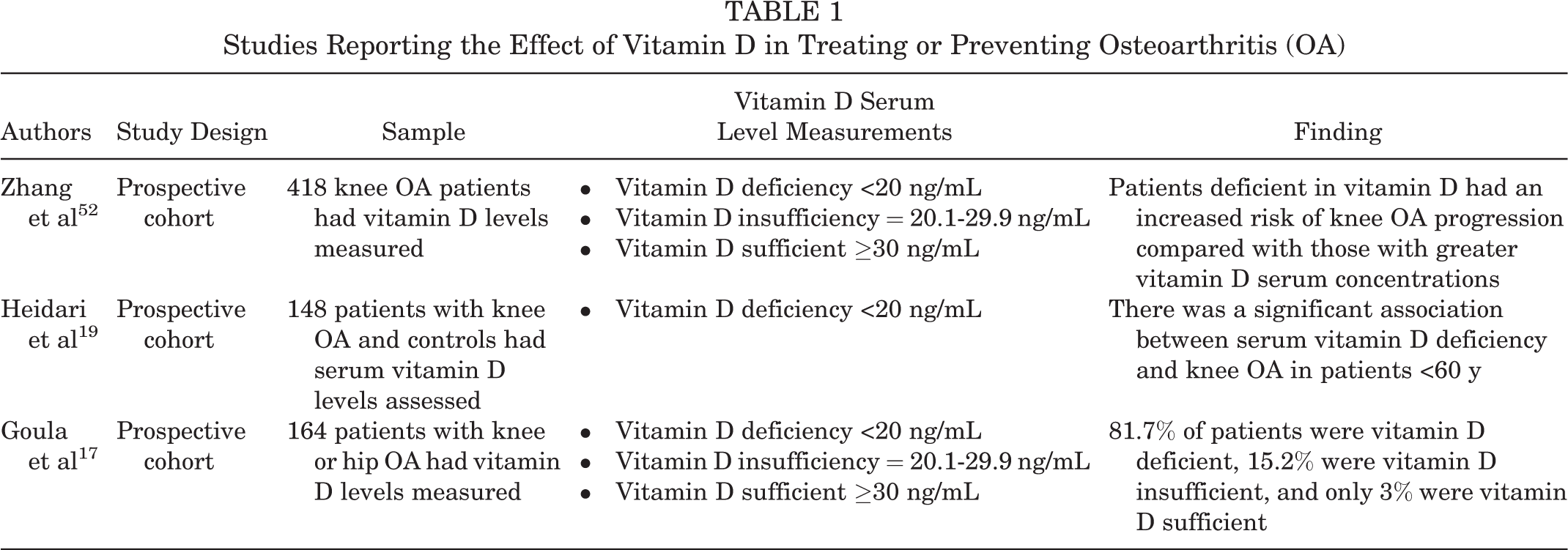
The efficacy of vitamin D in treating or preventing OA is controversial (Table 1). Some authors have found that vitamin D deficiency increases the risk of patients’ developing OA. In a prospective study, Zhang et al 52 found that individuals with similar characteristics who were deficient in vitamin D and who were assessed radiographically for OA had an increased risk for OA of the knee, as assessed by radiologists blinded to the study. In a cross-sectional study with age-matched controls, Heidari et al 19 found a similar result; however, this applied only to patients younger than 60 years. In an uncontrolled cohort study, Goula et al 17 found that a significant percentage of men and women who were vitamin D deficient had an increased prevalence of hip and knee arthritis based on radiologic assessment.
Studies Reporting the Effect of Vitamin D in Treating or Preventing Osteoarthritis (OA)
It has been shown that patients with OA have decreased vitamin D serum levels (Table 2). Bassiouni et al 9 and Veronese et al 49 both found that serum 25(OH)D levels were significantly decreased in the patients with knee OA and noted that medial meniscal deterioration was seen in patients with low vitamin D levels. In a cross-sectional study, Jansen and Haddad 24 showed that in elderly patients with advanced knee OA, there was a high prevalence of vitamin D deficiency. Interestingly, Konstari et al 27 found in a longitudinal cohort study that low serum 25(OH)D concentration did not predict increased incidence of knee and hip OA when looking at 5274 Finnish patients; however, their results can be questioned since patients who were considered to be vitamin D deficient were included with patients with normal vitamin D levels in the results.
Studies Investigating an Association Between Decreased Vitamin D Levels and Osteoarthritis (OA)

In several imaging studies, vitamin D deficiency is associated with decreased cartilage thickness (Table 3). In an ultrasonographic study, Malas et al 31 found that vitamin D deficiency significantly decreased femoral cartilage thickness in women between 20 and 45 years of age. In another longitudinal cohort study performed in the United States, men with vitamin D deficiency had a 2-fold increased likelihood of radiographic hip OA compared with men showing normal levels of vitamin D. 11
Studies Investigating an Association Between Vitamin D Deficiency and Decreased Cartilage Thickness

While these studies seem promising, imaging studies looking at increased vitamin D serum levels as a way to decrease the risk for OA have been inconclusive (Table 4). Hussain et al 23 showed that increased vitamin D serum concentrations were associated with an increased risk of hip arthroplasty for men with OA; however, this was not demonstrated in women. A 2-year randomized controlled trial in which 413 participants were given monthly treatments with oral vitamin D showed that oral supplementation did not produce significant clinical or cartilage volume structural differences in patients who were previously vitamin D deficient. 25 In a double-blind, randomized placebo-controlled trial, Arden et al 4 also showed that there was no significant difference in the rate of joint space narrowing in the medial compartment of knees due to vitamin D supplementation.
Studies Investigating Increased Vitamin D Serum Levels as a Way to Decrease the Risk for Osteoarthritis (OA)

Studies have shown conflicting results as to whether low vitamin D levels are correlated with OA-related pain in patients (Table 5). In a prospective study with 3874 Korean patients aged 65 years and older in whom serum 25-hydroxyvitamin D levels were measured and compared with knee radiographic OA and knee pain, serum vitamin D did not have a significant effect on pain in older adults. 28 In a cross-sectional study of 2756 patients with OA, only women with low vitamin D levels seemed to experience OA-related pain. 49 The Hertfordshire Cohort Study found that there was a significant association between vitamin D and knee pain. 36
Studies Investigating the Association Between Low Vitamin D Levels and Osteoarthritis (OA)–Related Pain

Furthermore, there are conflicting reports as to whether vitamin D supplementation decreases pain in OA (Table 6). In a 2-year randomized controlled study in which symptomatic knee OA patients were given oral doses of cholecaliciferol to raise serum levels of vitamin D, there was no reduction in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) knee pain scores. 34 In a double-blind study with 103 knee OA patients, patients receiving vitamin D oral supplements had slightly less pain compared with those receiving placebos after 1-year follow-up 45 ; however, these patients were not as physically capable as their placebo counterparts.
Studies Investigating the Clinical Effects of Vitamin D Supplementation to Decrease Osteoarthritis (OA) Pain

Conclusion
Much research has been conducted concerning the effects of vitamin D on OA, but few studies have been done to investigate the effects of vitamin D on articular cartilage degeneration and regeneration specifically. Vitamin D–sufficient patients have a lower risk of developing OA, and vitamin D sufficiency and supplementation decrease articular cartilage degeneration radiographically. Some studies have investigated the effect of vitamin D on OA progression and pain management; however, while there is no general consensus on the effects of vitamin D on OA, some results seem promising. Vitamin D supplementation may be a safe method to treat and prevent OA, but future research is required to define the specific pathway and ultimate efficacy.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by research grants R01 HL116042, R01 HL112597, and R01 HL120659 from the National Heart, Lung, and Blood Institute, National Institutes of Health to D.K.A. and the Haddix Grant to M.F.D.