
Abstract
Background:
Cartilage injury associated with anterior cruciate ligament (ACL) ruptures is common; however, relatively few reports exist on concurrent cartilage repair with ACL reconstruction. Autologous chondrocyte implantation (ACI) has been utilized successfully for treatment of moderate to large chondral defects.
Hypothesis:
ACL insufficiency with relatively large chondral defects may be effectively managed with concurrent ACL reconstruction and ACI.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients undergoing concurrent ACL primary or revision reconstruction with ACI of single or multiple cartilage defects were prospectively evaluated for a minimum 2 years. Pre- and postoperative outcome measures included the modified Cincinnati Rating Scale (MCRS), Western Ontario and McMaster Universities Osteoarthritis Index, visual analog pain scales, and postsurgery satisfaction surveys. ACI graft failure or persistent pain without functional improvement were considered treatment failures.
Results:
Twenty-six patients were included, with 13 primary and 13 revision ACL reconstructions performed. Mean defect total surface area was 8.4 cm2, with a mean follow-up of 95 months (range, 24-240 months). MCRS improved from 3.62 ± 1.42 to 5.54 ± 2.32, Western Ontario and McMaster Universities Osteoarthritis Index from 45.31 ± 17.27 to 26.54 ± 17.71, and visual analog pain scale from 6.19 ± 1.27 to 3.65 ± 1.77 (all Ps <.001). Eight patients were clinical failures, 69% of patients were improved at final follow-up, and 92% stated they would likely undergo the procedure again. No outcome correlation was found with regard to age, body mass index, sex, defect size/number, follow-up time, or primary versus revision ACL reconstruction. In subanalysis, revision ACL reconstructions had worse preoperative MCRS scores and greater defect surface areas. However, revision MCRS score improvements were greater, resulting in similar final functional scores when compared with primary reconstructions.
Conclusion:
Challenging cases of ACL tears with large chondral defects treated with concurrent ACL reconstruction and ACI can lead to moderately improved pain and function at long-term follow-up. Factors associated with clinical failure are not clear. When combined with ACI, patients undergoing revision ACL reconstructions have worse function preoperatively compared with those undergoing primary reconstructions but have similar final outcomes.
Keywords
Anterior cruciate ligament (ACL) tears are common injuries in young, active patients and often result in significant functional impairment. Pathology involving the menisci and/or articular surface is also common, with chondral defects reported in 16% to 46% of acute ACL tears. 9,19,53 Untreated ACL tears result in increased rates of chondral injury over time and are associated with multiple factors, including recurrent instability, meniscal insufficiency, individual activity level, and increased age. 11,23,26,39,53,56 Articular cartilage injury visualized at the time of ACL reconstruction has also been demonstrated to negatively affect long-term outcomes. 50
While early ligament reconstruction is often recommended to potentially prevent cartilage injury, the optimum treatment of existing chondral pathology in the setting of ACL insufficiency is unclear. 15,19,21,55 Potential treatment options include abrasion chondroplasty, microfracture, osteochondral autograft/allograft, or autologous chondrocyte implantation (ACI). The size and location of the defect, surgeon experience/preference, and other patient-specific factors potentially affect the treatment decision-making process. With relatively large defects, the options for surgical treatment become more limited.
ACI has been demonstrated to improve long-term subjective and objective outcomes in patients with intermediate to large chondral defects. § While this technique has evolved over 2 decades, there are little published data on its utilization concurrently with ligament reconstruction. In this series, we present intermediate to long-term results of combined ACI with ACL reconstruction in patients with relatively large chondral defects (mean, 8.4 cm2).
Methods
Patient Population
A search was performed from a single institution’s preexisting institutional review board (IRB)–approved database to retrospectively identify patients having undergone concurrent ACL reconstruction with ACI. This institution includes a high-volume cartilage repair center having performed more than 800 ACI procedures to date with prospective accumulation of measured outcomes in all patients. A minimum 2-year follow-up was required. Patients were included regardless of defect location and whether they underwent an associated procedure such as an osteotomy.
Indications
All patients were assessed as having functionally limiting pain and instability in the knee as well as having failed conservative management, and in most cases, prior surgery. Patients who smoked, required daily narcotics, or were unwilling to comply with postoperative rehabilitation and restrictions were not candidates for surgical treatment.
A standard physical examination was performed to assess laxity with Lachman and pivot shift maneuvers consistent with ACL insufficiency. All patients underwent magnetic resonance imaging that demonstrated the presence of at least 1 cartilage defect with size, location, and subchondral bone quality evaluated. Associated ligamentous pathology was also assessed. Standard weightbearing radiographs were performed in all patients, including anteroposterior (AP), lateral, 45° posteroanterior (PA; Rosenberg views), skyline, as well as full-length AP mechanical axis views. Patients with advanced unicompartmental or moderate to severe tricompartmental changes were excluded. Kellgren-Lawrence grading was performed retrospectively. In ACL revision cases, computed tomography scans were performed to assess tunnel expansion and/or malpositioning.
As part of a standard treatment algorithm, all patients assessed as being candidates for ACI underwent an examination under anesthesia and diagnostic arthroscopy to evaluate the chondral surface more clearly, and if indicated, a cartilage biopsy. During this diagnostic arthroscopy, a thorough evaluation of ACL/graft integrity was determined. In revision cases with tunnel malposition/dilatation, arthroscopic allograft bone grafting was performed in preparation for revision ACL reconstruction. Patients were then scheduled for a combined ACI with ACL reconstruction with additional procedures as indicated.
Surgical Technique
Autologous Chondrocyte Implantation
The ACI technique has been described previously. 33,36 Cartilage specimens harvested arthroscopically were placed into culture medium. Cells were expanded in vitro over 3 to 5 weeks prior to the scheduled surgical date (Vericel, formerly Sanofi-Genzyme BioSurgery). Implantation was performed initially with local harvesting of periosteum and, in later cases, with use of a resorbable bilayer collagen membrane (Bio-gide; Geistilch-Pharma North America). All membranes were secured with 6-0 Vicryl absorbable suture in a simple, interrupted pattern followed by injection of cultured cells within the contained defect and sealed with fibrin glue (Tisseel-Baxter). In cases of failed microfracture resulting in intralesional osteophytes, a “sandwich” technique was utilized with burring to normal bone, obtaining hemostasis, securing a base membrane with fibrin glue, and followed by the aforementioned technique with a second membrane. 31 The surgical procedure was performed under tourniquet control using an anterior longitudinal incision. Typically, a medial parapatellar arthrotomy was performed to expose the joint surface and intercondylar notch contents.
Anterior Cruciate Ligament Reconstruction
Because all ACI procedures in this series were performed using a standard open technique, the ACL reconstructions were also performed in an open manner. In cases of autograft reconstruction, a central-third bone–patellar tendon–bone graft (BPTB) was harvested during the initial approach and prepared for later reconstruction. Tunnel locations were determined based on visual confirmation of native footprint anatomy. The open approach allowed for relative ease in accurately visualizing and executing anatomic tunnels. In the case of the femoral tunnel, these were ensured to be at the anatomic footprint on the medial wall of the lateral femoral condyle. As mentioned previously, revision cases were often performed after staged bone grafting of nonanatomic tunnels. Grafts were initially secured with femoral tunnel interference screw placement. Final graft tensioning and tibial fixation were obtained with an interference screw after completion of the ACI.
Concurrent Procedures
All patients were assessed for malalignment as a contributing factor in their chondral injuries. Valgus-producing high tibial osteotomies were performed utilizing preoperative templating to transfer the mechanical axis through the center of the knee in cases of normal medial joint spaces or overcorrecting by 2° to the lateral tibial spine in cases with medial joint space narrowing. In earlier cases, a lateral closing wedge technique was used with later transition to a medial opening wedge technique. In 2 cases necessitating both staged bone grafting with high tibial osteotomy (HTO), the osteotomy was performed in the first stage. When performing a combined ACL reconstruction with HTO, the osteotomy was performed first, as low as possible in the metaphysis, with posterior plate fixation allowing for adequate positioning of the tibial tunnel proximal and anterior to the osteotomy and hardware, respectively. Tibial tubercle anteromedialization osteotomies were considered in patients with patellofemoral defects/maltracking.
Postoperative Rehabilitation and Follow-up
All patients underwent a supervised postoperative course of rehabilitation. 31 Continuous passive motion was utilized immediately postoperative, and patients remained touchdown weightbearing for 6 weeks with a hinged brace locked in extension. Initial outpatient physical therapy focused on range of motion, isometrics, and patellar mobilization for the first 6 weeks. Weightbearing and active range of motion were then advanced along with discontinuation of bracing from weeks 7 to 12. Beyond week 12, patients returned to daily activities as tolerated and progressed with strengthening and low-impact exercise with avoidance of any high-impact or pivoting activity for at least 12 months. A follow-up magnetic resonance image was obtained at 1 year to evaluate graft incorporation.
Treatment Failures
Failure was defined as any patient with 1 or more of the following results: (1) failed ACI resulting in defect rerepair, (2) complete ACI graft delamination or >25% ACI graft failure to incorporate regardless of additional treatment, (3) conversion or plan for conversion to prosthetic arthroplasty, or (4) no clinical improvement based on postoperative outcomes measures. Cases were not considered treatment failures if follow-up operations were performed to address ACI graft hypertrophy/mild fraying or arthrofibrosis. Additionally, diffuse progression of degeneration in clinically improved patients was not considered grounds for failure.
Functional Outcomes
Patient-specific data were collected in the institution’s IRB preapproved databank preoperatively and then continued prospectively at regular intervals postoperatively. Patients completed questionnaires including an activity-based questionnaire, the modified Cincinnati Rating Scale (MCRS, description in Appendix 1), and an osteoarthritis-focused questionnaire, the Western Ontario and McMasters Universities Osteoarthritis Index (WOMAC, 0- to 96-point scale; lower values indicated improved function). Additional outcomes measures such as the International Knee Documentation Committee (IKDC), though part of the standard database, were not available for the earliest patients in the study and were therefore not included in the analysis. Patients were also questioned on general satisfaction with the procedure and completed visual analog pain scales (VAS).
Statistical Analysis
Preoperative outcomes measures were compared with final follow-up data utilizing paired and independent variable t tests. Level of significance was set at P < .05. In cases assessed as clinical failures, follow-up time was finalized at that point to avoid inaccurate overestimation of time to failure. In addition, further comparisons were made with both patient-specific (age, body mass index [BMI], and sex) as well as pathology-specific variables (defect size, type, and location; primary vs revision ACL; and prior and concurrent procedures).
Results
Demographics
Twenty-seven patients were identified who met inclusion criteria. One patient was lost to follow-up, leaving 26 patients who completed final evaluation, with a mean follow-up of 95 months (range, 24-240 months). Mean age at time of the index procedure was 36 years (SD, 10.6 years; range, 18-56 years). Seventeen males and 9 females participated, with 11 right and 15 left knees included (none bilateral). Mean BMI was 27.2 kg/m2 (SD, 4.2 kg/m2). One patient’s injury was the result of a workers’ compensation claim. Eighteen patients had undergone at least 1 prior surgery on the affected knee (mean, 1.8; SD, 2.3; range, 0-10), including 13 prior ACL reconstructions, 9 patients with a previous microfracture, and 8 patients undergoing prior partial medial or lateral meniscectomy.
Procedures
Thirteen primary and 13 revision ACL reconstructions were performed. BPTB allograft was used in all revision reconstructions, and BPTB autograft was utilized in the first 8 primary reconstructions, with transition to allograft for the last 5 reconstructions. The first 19 consecutive patients in the series underwent ACI with periosteal membrane (ACI-P), and the remaining 7 patients with collagen bilayer membrane (ACI-C; non–Food and Drug Administration approved). Six patients had varus malalignment and underwent a concurrent valgus-producing HTO (3 closing and 3 open wedge). One patient underwent a tibial tubercle osteotomy. One patient had a concurrent meniscal repair, 2 patients had partial meniscectomies, and no patients required meniscal allograft transplantation.
Defect Description
Defects were classified using a previously described system as simple, complex, or salvage. 31,32 Because each knee included associated pathology (ACL insufficiency), there were by definition no simple defects. Eleven patients were classified as having complex and 15 as having salvage-type defects, as noted by presence of early osteoarthritic changes. Thirteen patients had single chondral defects, and 13 patients had 2 or more defects, of which 5 were bipolar. Mean total surface area was 8.4 cm2 (SD, 4.3 cm2; range, 3.3-16.75 cm2). Defect locations included 21 medial femoral condyle (MFC), 8 lateral femoral condyle (LFC), 2 medial tibial plateau, 9 trochlea, and 4 patella. Individual defect mean sizes were: MFC, 5.4 cm2; LFC, 5.8 cm2; trochlea, 4.9 cm2; and patella, 2.4 cm2. In terms of Kellgren-Lawrence grading, 6 patients were grade 1, 15 grade 2, and 5 grade 3.
Failures
Eight of 26 patients (31%) were assessed as clinical failures. Five patients had isolated ACI graft failure, 1 had combined graft failure with disease progression, and 2 had disease progression away from the healed defect. One ACI failure also included an associated ACL graft failure. Mean time to failure was 52 months (range, 6-132 months). The only patient in the series with injury resulting from workers’ compensation clinically failed. Two patients were early failures, both at 6 months, and no other patients failed earlier than 36 months. Of the failures, 5 eventually were converted to arthroplasty and 3 underwent revision ACI. One additional patient sustained reinjury resulting in ACL graft rupture but was not considered a clinical failure for the purposes of this study due to a well-maintained ACI graft and good final outcome scores/satisfaction after revision ACL reconstruction.
Outcome Measurements and Statistical Analysis
Sixty-nine percent of patients were improved and rated their knee as good or excellent at final follow-up. Ninety-two percent of patients (24/26) stated they would definitely or probably undergo the procedure again. All measured outcome scores significantly improved from pre- to postoperative (Table 1). In comparing the clinical failure group with the nonfailure group, there were no statistically significant differences in patient demographics including age, sex, or BMI (see Appendix 2). Furthermore, there were no statistically significant differences between groups in defect number/type/location, total surface area, bipolar defects, preoperative Kellgren-Lawrence grade, prior microfracture, number of prior surgeries, revision versus primary ACL reconstruction, ACL graft type, membrane type, or concurrent osteotomy. Of the 5 patients with preoperative Kellgren-Lawrence grade 3, only 1 clinically failed. There was an insignificant statistical trend of increased follow-up time associated with failure; however, after excluding the 2 acute failures as potential outliers, there was still no significant difference in follow-up. Not all patients had final radiographs available for review; therefore, an assessment of progression of radiographic osteoarthritis was not possible. However, there was a significant difference in preoperative Kellgren-Lawrence grades between revision and primary ACL reconstruction cases (2.31 ± 0.63 vs 1.62 ± 0.51, P < .003). When excluding the 8 patients considered failures, the outcome measures of the 18 clinically successful patients were: MCRS, 6.39 ± 2.12; WOMAC, 20.83 ± 13.88; and VAS, 2.72 ± 1.58 (see Appendix 2).
Outcome Scores a

a MCRS, modified Cincinnati Rating Scale; VAS, visual analog scale for pain; WOMAC, Western Ontario and McMaster Universities Ostoearthritis Index.
A subanalysis was performed comparing patients with single versus multiple defects and primary versus revision reconstruction (Table 2). Though patients with multiple defects had significantly greater surface area involvement, there were no statistically significant differences in final outcomes compared with patients with single defects. When comparing primary versus revision ACL reconstruction, revision patients had significantly greater defect numbers and total surface areas and lower preoperative MCRS scores. WOMAC and VAS scores did not differ between groups pre- or postoperatively. However, MCRS improvements were significantly greater in revision reconstruction patients when compared with primary reconstructions such that final MCRS scores did not differ between the 2 groups.
Subanalysis a

a Boldfaced values indicate statistically significant differences. BMI, body mass index; MCRS, modified Cincinnati Rating Scale; n/a, not applicable; TSA, defect total surface area.
Complications and Reoperations
One major complication occurred: an early postoperative infection treated with arthroscopic irrigation and debridement, resulting in a viable graft and successful final outcome. Graft hypertrophy (n = 8), graft failure (n = 6), and arthrofibrosis (n = 6) were the most common indications for reoperation. The mean number of reoperations in the failure group was 4.0 (range, 1-9) compared with 1.2 (range, 0-2) in the nonfailure group. The most common procedure was arthroscopic debridement for either periosteal hypertrophy (1 failure and 7 nonfailure patients, all with ACI-P) or chondroplasty of graft failure/progression of disease (8 failure patients). Six patients underwent arthroscopic lysis of adhesions for arthrofibrosis (1 failure, 5 nonfailures). After modification of technique from ACI-P to ACI-C, reoperations in clinically successful patients averaged 0.4 per patient.
Discussion
We present a series of 26 patients having undergone combined ACL reconstruction and ACI for relatively large chondral defects (mean total surface area, 8.4 cm2). The patients were evaluated with prospective clinical outcome measures for pain and function, with intermediate to long-term follow-up averaging over 8 years. Sixty-nine percent of patients were improved at final follow-up. Despite 8 failures, only 2 patients stated they would not choose to undergo the procedure again.
ACL reconstructions are among the most commonly performed procedures in the United States, and surgical rates are increasing. 27 Though the association of ACL tears with chondral injuries is well established, there are relatively little published data on concurrent cartilage repair with ACL reconstruction. 9 This may be related to defect heterogeneity, diverse treatment options, and individual surgeon experience. Procedures such as abrasion chondroplasty and microfracture in association with an ACL reconstruction may be underreported. Furthermore, some authors have suggested that nontreatment of chondral defects at the time of ACL reconstruction may lead to similar long-term clinical outcomes as in patients without chondral injuries. 51,57 However, in those reports, the mean defect sizes were significantly smaller than in our series (range, 1.7-2.1 cm2). Cox et al 13 conversely found that grade III and IV defects observed during ACL reconstructions resulted in significantly worse outcomes compared with matched controls at 6 years.
Concurrent ACL reconstruction with osteochondral autograft transplantation has been reported to be effective in cases of relatively small defects. 7,22,28 A single high-level study randomized 102 patients undergoing ACL reconstruction with medial femoral condyle defects (range, 2-4 cm2) to arthroscopic debridement, microfracture, or osteochondral autograft transplantation. At 3 years, nondefect controls had superior outcomes; however, patients undergoing osteochondral autograft were still significantly better than those undergoing debridement or microfracture regarding IKDC scores. 17 There are published reports on microfracture in the setting of ACL reconstruction. Osti et al 44 reported on 25 patients undergoing microfracture for grade III to IV defects with ACL reconstruction. At 5 years, these patients had greater rates of radiographic osteoarthritis and worse WOMAC scores when compared with a matched group of patients with grade I to II defects treated with radiofrequency. 44 In a review of the English literature, no reports on combined osteochondral allograft transplantation with ACL reconstruction were found. The presumed rarity of this combined procedure may be secondary to the logistical challenges of obtaining allograft in the setting of patients who desire definitive ligamentous stabilization in a timely fashion.
The concurrent use of ACI for chondral defects in the setting of ACL reconstruction is also not widely reported. One small series of 7 patients treated with ACI-P for defects averaging 7.3 cm2 had improved functional outcomes at a mean of 31 months postoperative. 4 Another study reported good to excellent results in 8 of 9 patients undergoing concurrent ACI/ACL after 23 months and noted overall superior results when compared with a matched group that underwent ACI subsequent to ACL reconstruction. 2 Dhinsa et al 14 also compared patients undergoing combined ACI/ACL with those having staged ACI after ACL reconstruction and compared these patients with an isolated ACI cohort. At 5-year follow-up, the best outcomes were with patients requiring only ACI without ligament reconstruction, followed by combined ACI/ACL, and with the staged group having the worst functional outcome. 14 They also found a significant negative association in outcome with larger defects. In a series of patients undergoing ACI with mean follow-up of over 12.8 years, the authors reported on a subset of 42 patients having undergone a concurrent ACL reconstruction. 47 MFC defects were the most common, and mean defect sizes were 4.5 and 4.6 cm2 for the MFC and LFC, respectively. Thirty-four of 42 patients (81%) stated they were improved or the same at final follow-up, with 91% stating they would undergo the procedure again. 47
There are several factors in the current series that are similar to previously published reports on chondral defects associated with ACL tears. The most common location was the MFC, which is consistent with prior series, 26,46 though others have reported the LFC to be most frequently involved in acute injuries. 54 Patellofemoral defects have been reported as a late finding after ACL reconstruction, 43 which was consistent with our results as only 2 of 13 patellofemoral defects occurred in primary reconstruction cases. Patellofemoral defects were not found to have worse outcomes in our population, which is also consistent with other reports demonstrating favorable outcomes in treating these defects with ACI. 16,34 In terms of defect size, this series includes a larger mean surface area of both single and combined defects. Despite this fact, the outcomes were not significantly worse in patients with larger surface areas involved or with multiple defects.
A notable finding in this study was that outcomes of cases involving revision ACL reconstructions were equivalent to primary reconstructions. The observation that initial MCRS scores in failed reconstructions were significantly worse than in primary reconstructions is also consistent with prior reports. 12 Outcomes of revision ACL reconstruction are typically inferior to primary cases. 3 However, in our series, while revision reconstructions had worse function preoperatively, the degree of improvement was greater, and overall final outcomes were equivalent to primary cases. As revision cases in this series had larger defect sizes, the ability of ACI to effectively treat large surface areas may potentially explain this outcome. However, as there were also no significant differences between revision and primary reconstructions with regard to WOMAC and VAS scores, a conclusive validation of this finding would require further study with larger patient numbers. An additional advantage of ACI with revision ACL reconstruction is the potential need for staged bone grafting of expanded or malpositioned tunnels. With ACI, an initial diagnostic arthroscopy is performed, enabling a thorough evaluation of chondral pathology, obtaining a cartilage biopsy, and also allowing for treatment of abnormal tunnels in this index procedure.
An additional factor that further complicates the ability to predict late outcomes after cartilage repair with ACL reconstruction is the known progression of osteoarthritis that often occurs after ACL tears. 1,5,38,42,48 Predisposing factors for the progression of cartilage injury are multifactorial and potentially include advancing age, BMI, associated meniscal pathology, activity level, recurrent instability, abnormal range of motion, poor strength, and progression of time. ǁ Microscopic damage to the joint surface along with an inflammatory cascade beginning at the time of injury may result in some patients progressing to degeneration despite surgical reconstruction. 15,18 This natural course of posttraumatic degenerative joint disease along with the complex multifactorial nature of symptomatology may further contribute to the lack of conclusiveness in predictive factors for failure in this series. Interestingly, patients undergoing revision reconstruction did have significantly higher Kellgren-Lawrence grades preoperatively; however, at final follow-up, these patients did not have worse functional outcomes despite the more advanced preoperative arthritic changes.
There are several limitations of this study. These include the relatively small number of patients as well as the heterogeneity of defect characteristics and concurrent procedures. However, it is important to note that this combined procedure is much less commonly performed than either procedure alone. Of more than 800 ACIs performed at the reporting institution, less than 30 of those were associated with a concurrent ACL reconstruction. Because of the relative rarity and inherent complexity of these cases, heterogeneity is to be expected with regard to patient, defect, and surgical variables. Regardless, these factors do weaken our statistical analysis and may hide factors that contribute to long-term failure. While our series found no patient- or defect-specific characteristic associated with failure, other series have demonstrated factors such as prior microfracture, concurrent osteotomies, or salvage-type lesions as being predictive of worse outcomes with ACI. 25,31,35,37,58 Another limitation is that follow-up time varied greatly, though this is also inherent with the relative infrequency of the procedure performed. This does contribute to further variability, with an expected evolution of surgical technique over time as membrane type, graft selection, and osteotomy type all evolved. Finally, a complete radiographic evaluation for progression of osteoarthritis could not be performed, as final films were not available for all patients given that outcomes were assessed clinically and not radiographically.
An important consideration in any analysis of treating knee pathology in relatively young, active patients is the ability to return to preinjury levels of activity, including sports. A recent systematic review found both ACI and osteochondral autograft transplantations to have rates of return to sport exceeding 80%, both superior to microfracture. 10 Factors associated with increased sports participation included smaller defect size, younger age, shorter duration of symptoms, and no prior surgeries. While ACI has been demonstrated to consistently improve pain and functionality with daily activities and recreational sports, some studies have reported that return to high-level sports is unlikely. 45 Our series had similar findings, with successfully treated patients having significant functional improvement (MCRS >6). However, this level of function is most consistent with an ability to return to some sports activity but not unrestricted participation (Appendix 1).
Conclusion
ACL insufficiency with intermediate to large chondral defects treated with concurrent ACI and ACL reconstruction can lead to improved pain and function in patients for many years. However, it is important to counsel patients that progression to degenerative changes resulting in persistent pain and dysfunction is not uncommon, and return to high-level sports may be unrealistic. Improvement in technique appears to have resulted in lower reoperation rates; however, it is important to counsel patients that even in successful cases, undergoing a follow-up arthroscopic procedure is not uncommon. Cases of failed ACL reconstructions with large or multiple chondral defects may have similar outcomes when ACI is performed with revision ACL reconstruction compared with primary cases.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: T.M. is a paid consultant for Vericel.
Ethical approval for this study was obtained from the Partners Human Research Committee, Boston, MA (Protocol #: 2007P000470/BWH).
Notes
Appendix 1
Modified Cincinnati Rating Scale 32
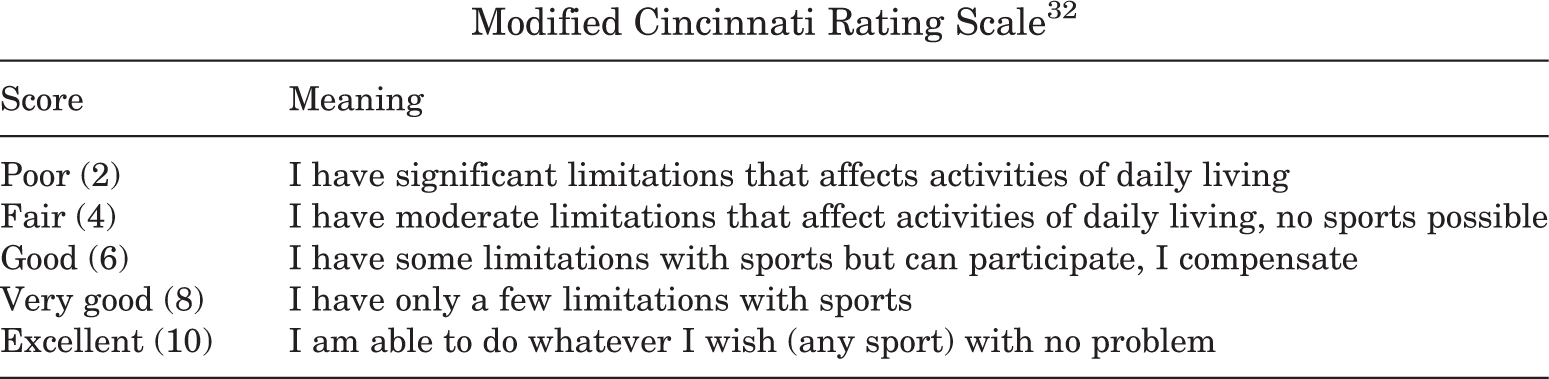
| Score | Meaning |
|---|---|
| Poor (2) | I have significant limitations that affects activities of daily living |
| Fair (4) | I have moderate limitations that affect activities of daily living, no sports possible |
| Good (6) | I have some limitations with sports but can participate, I compensate |
| Very good (8) | I have only a few limitations with sports |
| Excellent (10) | I am able to do whatever I wish (any sport) with no problem |
Appendix 2
Success Versus Failure Analysis a

| Final Outcome | Clinical Success | Clinical Failure | P Value |
|---|---|---|---|
| Patients, n | 18 | 8 | |
| Age, y | 36.6 ± 10.7 | 36.5 ± 11.9 | .981 |
| BMI, kg/m2 | 26.5 ± 3.5 | 28.8 ± 5.7 | .221 |
| TSA, cm2 | 9.15 ± 4.09 | 6.78 ± 5.06 | .216 |
| Defects, n | 1.8 ± 0.9 | 1.3 ± 0.5 | .085 |
| Follow-up, mo | 113 ± 68 | 67 ± 47 | .09 |
| Reoperation, n, mean | 1.2 ± 0.9 | 4.0 ± 2.6 |
|
| Kellgren-Lawrence grade | 2.05 ± 0.62 | 1.75 ± 0.66 | .32 |
| MCRS preoperative | 3.67 ± 1.50 | 3.50 ± 1.31 | .79 |
| MCRS postoperative | 6.39 ± 2.12 | 3.62 ± 1.51 |
|
| WOMAC preoperative | 48.78 ± 17.24 | 37.50 ± 15.60 | .127 |
| WOMAC postoperative | 20.83 ± 13.88 | 39.38 ± 19.52 |
|
| VAS preoperative | 6.00 ± 1.33 | 6.63 ± 1.06 | .25 |
| VAS postoperative | 2.72 ± 1.58 | 5.75 ± 1.28 |
|
a Boldfaced P values indicate statistically significant differences. BMI, body mass index; MCRS, modified Cincinnati Rating Scale; TSA, defect total surface area; VAS, visual analog scale for pain; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.