
Abstract
Background:
Recurrent anterior shoulder instability after coracoid process transfers may be caused by trauma, sports injury, or technical failure of the index procedure. Surgical techniques vary with regard to graft orientation and positioning and number of screws utilized for fixation.
Purpose:
To identify surgical and patient-related factors associated with failure, defined as the need for revision surgery. We hypothesized that failures will occur more commonly with single-screw fixation and graft malposition.
Study Design:
Case series; Level of evidence, 4.
Methods:
Eighty-three patients (mean age, 24 years) who underwent an Eden-Hybinette operation as a revision procedure for recurrent anterior instability after primary coracoid process transfer between 1977 and 2010 were retrospectively reviewed. Preoperative medical records were queried for demographic data, failure event, and physical examination. Two fellowship-trained shoulder surgeons reviewed radiographs to identify for graft positioning, nonunion, and hardware failure. Descriptive analysis was used to assess reasons for failure.
Results:
Seventy-five percent of patients sustained a redislocation event after primary coracoid process transfer. Revisions were performed on average 50.3 months after the index procedure, most commonly on males, with two-thirds of recurrent instability occurring during sports. Among all patients, single-screw methods for fixation and inferior graft malposition during index bone block transfer were the most common. Hardware failure and graft nonunion were more frequent with the single-screw technique.
Conclusion:
In our series, recurrent anterior shoulder instability after primary coracoid process transfer was more likely to occur during sports in young, male patients. The most common technical errors leading to revision were placing the graft inferior to the 5-o’clock position on the glenoid face or relying on single-screw fixation.
Anterior shoulder instability is a common clinical problem that often requires surgical intervention. The incidence of shoulder instability is reported to be 0.08 and 0.24 per 1000 person-years in the United States and Europe, respectively. 23,26 Controversy remains, internationally, whether soft tissue or osseous procedures should be utilized as the index procedure for recurrent anterior shoulder instability without glenoid bone loss. Most large series report improvement in patient satisfaction after surgery; however, reported recurrence rates after successful Latarjet are around 3%, compared with 15% for Bankart procedures. 13,20,22 Glenoid deficiency of 20% to 25% has been shown to be a significant risk factor for recurrent instability after soft tissue procedures alone, such as arthroscopic labral repairs. 4,6,15,20 Biomechanical models show that 70% of stability restraint is lost at this critical point, and soft tissue procedures fail almost 67% of the time. 4,8 In this setting, it is generally accepted that reconstitution of the glenoid should be performed, usually with a bone-block transfer such as a Latarjet or Bristow procedure.
Latarjet 18 described the transfer of an osteotomized coracoid process oriented with its longitudinal axis parallel to the face of the glenoid. Four years later, Helfet 11 described a similar procedure, named after his mentor Bristow, with the exception that the osteotomized coracoid was transferred in an upright position using a single screw for fixation “down the pike” of the coracoid. 18,25 These procedures have evolved over time, and many variations now exist, including different graft orientation and positioning as well as type of fixation and number of screws utilized. 25,28,29 The total number of annual procedures worldwide has not been previously reported to our knowledge, but approximately 2000 of these procedures were performed at our institution from 1977 to 2000. Bone block transfers have been shown to be relatively successfully, but recurrent instability requiring revision surgery is reported at 1% to 7%. 1,10,13,14,29
The Eden-Hybinette procedure is commonly reserved for revision scenarios and has been shown to be successful after a failed Latarjet procedure. 19,26 It involves the harvest and placement of a tricortical iliac crest graft on the anterior glenoid to stabilize the shoulder. Previous studies have explored reasons for failed coracoid process transfers. 1 –3,21,27,30 Definitions for failure have varied and include recurrent instability, development of early glenohumeral arthritis and significant stiffness, hardware failure or complication, and graft nonunion or osteolysis. Preoperative joint laxity may lead to recurrent glenohumeral instability. 30 The use of bioabsorbable screws was recently identified in a small series as a technical factor leading to graft osteolysis. 2 Malposition of the coracoid graft along the glenoid rim has also been previously identified as a risk factor for development of glenohumeral arthritis, graft lysis, and nonunion. 1,3,21,27
The purpose of this study was to identify technical reasons and patient-related factors associated with failure after primary coracoid process transfer. We define failure as recurrent instability requiring revision with an Eden-Hybinette procedure. To date, no large series has focused specifically on the most frequent errors in surgical technique leading to failure. We hypothesize that single-screw fixation and graft malposition are most commonly associated with failure.
Methods
Failure after a primary coracoid process transfer in this descriptive study was defined as recurrent instability necessitating revision with an Eden-Hybinette operation. All patients who underwent an Eden-Hybinette operation by the senior author at 1 institution between 1977 and 2010 were retrospectively reviewed. Eighty-three patients (mean age, 24 years) meeting the study criteria were identified. Of these, 11 patients had incomplete data and were excluded, leaving 72 available for study (59 men, 13 women). Medical records were reviewed for demographic data, failure event, sporting activity, operative report (if available), and subscapularis integrity and presence of hyperlaxity defined by Beighton score greater than or equal to 5 on physical examination. Two fellowship-trained shoulder surgeons reviewed neutral anterior-posterior, internal rotation, external rotation, scapular-Y, and Stryker notch radiographs to identify surgical fixation technique, graft position, and presence of new fracture, nonunion, or hardware failure. These radiographic views are standardized at our institution, and repeat films are ordered if the images are not satisfactory. Ideal placement for a standard 2-cm graft was defined from the 3- to 5-o’clock position on the glenoid face and used as the reference point during analysis. 24 Superior malposition was defined from 3 o’clock superiorly, inferior malposition from 5 o’clock inferiorly, and medial malposition as greater than 2 mm medial to the glenoid rim. 27
The senior author (G.W.) performed the index Latarjet procedure in 17 of 72 patients meeting our inclusion criteria. These operations were done in a semi-inclined beach-chair position with a subscapularis split and fixation of the coracoid graft oriented with its longitudinal axis parallel to the face of the glenoid with two 4.5-mm malleolar screws. 28,29 Reattachment of the capsule to the stump of the coracoacromial ligament was also routine. 28,29 Among the other 55 patients who were tertiary referrals to the senior author after failure of their index procedure, 34 used similar graft orientation and there were 10 Bristow procedures. Because of removal of hardware or lack of records before evaluation, hardware analysis could only be performed in 61 of 72 patients by radiograph.
Results
Patient demographics are outlined in Table 1, highlighting that two-thirds of the failure events occurred during sporting activity, 38% of which were contact sports—most commonly rugby. Eighteen patients experienced symptomatic instability without frank dislocation, while the etiologies and mean time to failure for those suffering a redislocation event are shown in Table 2. Dislocation or symptomatic instability during sporting activity accounted for the majority of new fractures (75%), hardware failure (67%), graft migration (65%), and subscapularis rupture (65%) in the cohort.
Patient Demographics

Etiology and Mean Time to Failure Among Patients Suffering a Redislocation Event (n = 54; 75%) a

a MVA, motor vehicle accident.
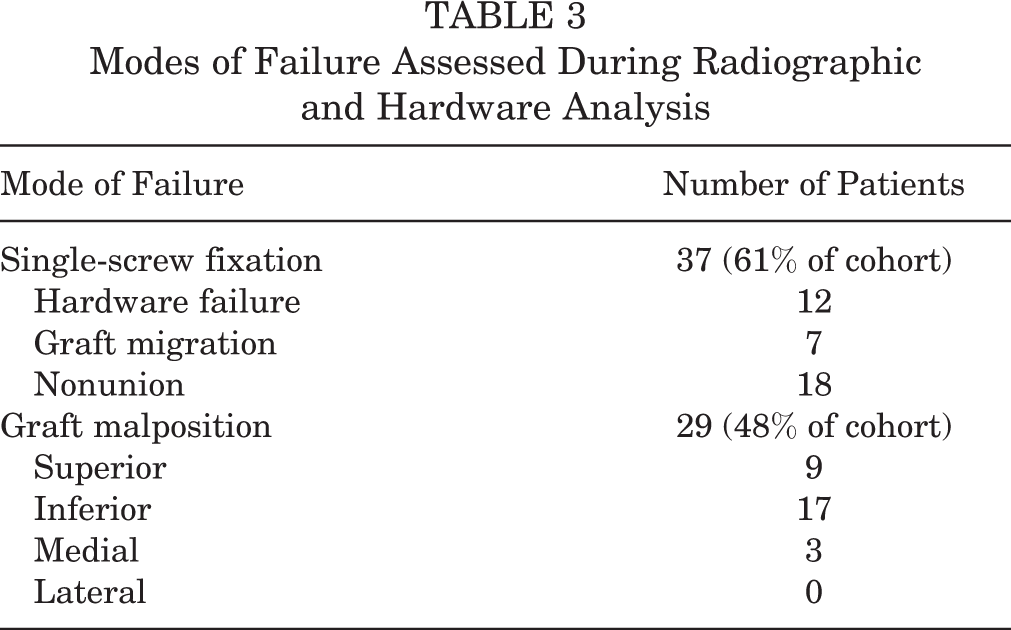
Among all patients in whom a failed index procedure could be identified by radiograph, 51 bone blocks were placed with their longitudinal axis parallel to the face of the glenoid (27 with single-screw fixation). Overall, single-screw methods for fixation were most common (Table 3). Hardware failure (57%) including bent, broken, and migrated screws (Figure 1) and graft nonunion (72%) was also seen more frequently with the single-screw technique. Among grafts judged to be malpositioned, inferior bone block placement (Figure 2) was more common than superior or medial malpositioning, with no cases of lateral overhang (Table 3).
Modes of Failure Assessed During Radiographic and Hardware Analysis
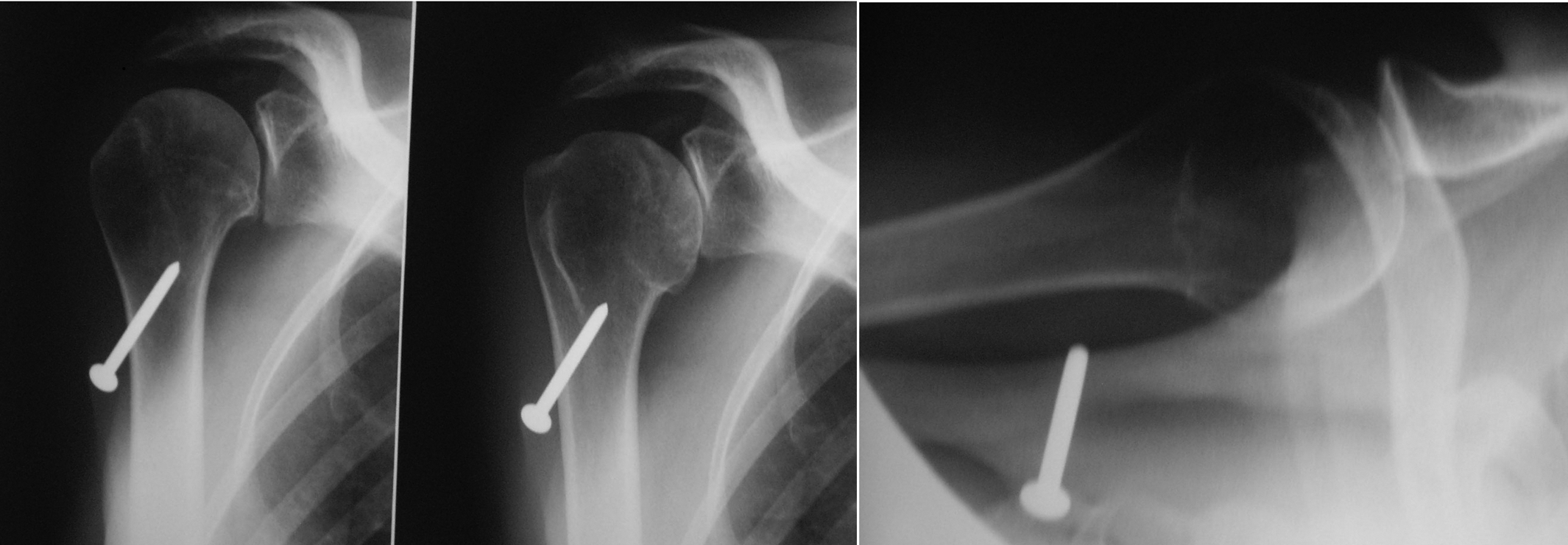
Pseudathrosis due to screw migration leading to biomechanic instability.
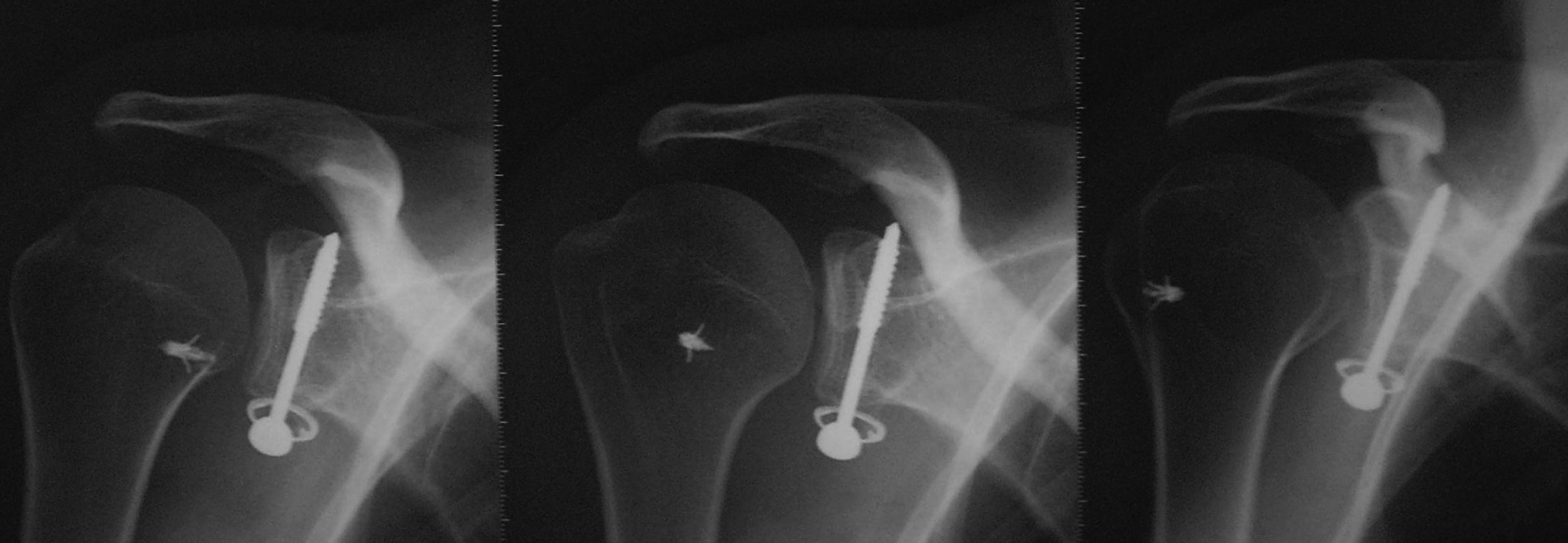
Example of inferior bone block malposition.
For the 17 patients who underwent the index Latarjet procedure by the revision surgeon, the most common reason for failure was new fracture (n = 8). The mechanism of injury in these cases was fall from height, participation in American football and rugby, and seizures. Symptomatic instability (n = 7) and hyperlaxity (n = 2) were also reported. Radiographs in these cases revealed 7 bent screws (5 due to new fracture) and 3 malpositioned grafts (2 inferior, 1 medial).
Discussion
Single-screw fixation and inferior graft malposition were most frequently associated with failure in our study, supporting our hypothesis. Sixty-one percent of patients were treated with single-screw fixation, accounting for 18 of 25 total cases in the series that went on to nonunion (see Table 3). A single screw may not confer enough rotational and compressive stability to allow for union, as evidenced by the number of hardware failures (57%) seen in this group. The addition of a second screw allows for greater compression and rotational control, which minimizes graft micromotion and theoretically decreases the chance for nonunion, graft migration, and failure. 17 Due to the inferior coracoid’s large contact area with the glenoid in the Latarjet technique, the placement of 2 screws is feasible. 18 The findings in our study may be consistent with greater risks of nonunion among tertiary referrals related to decreased surface area for bony healing in Bristow cases (n = 10) or technical error in the 27 cases (7 of 34 patients records or radiographs were not available) in which the surgeon used a Latarjet technique. Biomechanically, the Bristow technique has been shown to be less favorable than a Latarjet procedure, with less surface area for healing. 9,11
Malposition of the coracoid graft along the glenoid rim has been previously identified as a risk factor for development of glenohumeral arthritis, mostly in the setting of lateral overhang, graft lysis and nonunion, and recurrent instability. 1,7,27 Hovelius et al 12 reported an increased risk of recurrent instability with bone block placement in the upright position 1 cm or more medial to the glenoid rim, although placement >2 mm has been shown to be a risk factor for recurrent instability. 27 Ideal graft placement has been well discussed in the literature. 3,16,21,27 Nourissat et al 24 performed a biomechanical study demonstrating that the 4-o’clock position provided the best restraint to anterior displacement of the humeral head and inferior glenohumeral translation. In our study, 29 grafts were judged to be malpositioned during the index procedure, with 59% being placed inferior to the 5-o’clock position (see Table 3). Given the graft position in these patients, anterior translation likely occurs as a result of the humeral head jumping over the graft during shoulder abduction and external rotation. Superior (31%) and medial (10%) graft malpositioning was also identified but occurred much less commonly than inferior malpositioning. There were 9 patients (12.5%) with no identifiable technical reason for failure. Of these, new trauma was identified in the majority of cases.
Consistent with the literature, younger, male patients in their third decade of life were more likely to require revision in this series. 3,5,13 Mean time to failure was 50.3 months, and there were twice as many failures during sporting activity (see Table 1). This cohort represented a wide array of sports and including overhead activities, noncontact sports, and contact sports, most commonly rugby (see Table 2). Burkhart et al 5 described a series of 55 contact athletes who underwent a Latarjet procedure and found that 96% of these athletes were able to return to their sport for at least 1 season, but 5% of these patients had recurrent instability. Another large series found that 83% of athletes were able to return to sport at their preinjury level. 29 Our results show that patients participating in sports were more likely to need revision surgery, with 38% participating in contact sports (see Table 1) and 75% sustaining a redislocation event (see Table 2). Failures during sporting activity accounted for the majority of new fractures (75%), hardware failure (67%), graft migration (65%), and subscapularis rupture (65%) in the cohort. For this reason, we prefer subscapularis splitting approaches to avoid this potentially devastating complication.
Mean time to failure in those redislocating was 39 months versus only 13 months in patients with hyperlaxity on examination (see Table 2). In 1991, Young and Rockwood 30 explored reasons for failed coracoid process transfers. This retrospective review of 39 patients after a Bristow procedure found excessive laxity of the joint capsule as the primary etiology for failure in 80% of cases. 30 This finding is in stark contrast to our series of 72 patients, as only 7% were found to have hyperlaxity on physical examination before revision.
There are several limitations to our study. The retrospective and descriptive nature of this study permits only the observation of trends and calculation of the frequency of technical pitfalls rather than providing comparative analysis to establish relative risk. Although a single surgeon performed all Eden-Hybinette procedures, 55 index cases were performed by a number of surgeons in the surrounding community. Therefore, it is likely that there is more variability between procedures than accounted for in our analysis. Likewise, the number and type of surgical procedures for each patient between the index procedure and revision are unknown, as are the total number of index cases performed, which may influence the interpretation of our results. Similarly, the total number of coracoid process transfers performed annually has not been reported in the literature and can only be extrapolated from a single surgeon or group’s experience, in our case, 2000 procedures over 33 years. With regard to imaging, computed topography scans were not universally used for preoperative planning at the outset of the study period; therefore, radiographs were used for analysis in 72 patients, 61 of which did not have prior hardware removal. Last, our conclusions may be subject to selection bias, as failures during sporting activity were the largest cohort in this study. These patients may be more likely to seek treatment owing to their activity level and desire to return to participation.
Despite these limitations and given the experience at our institution with bone block transfers, we recommend placing the bone graft between the 3- and 5-o’clock position with its inferior surface flush with the anterior glenoid, as originally describe by Latarjet. The graft should be of sufficient size to allow fixation to the glenoid with 2 screws, especially in patients who participate in sports.
Conclusion
In our study, the most frequent technical errors during primary coracoid process transfer that led to recurrent instability were placement of the bone graft inferior to the 5-o’clock position on the glenoid face or relying on single-screw fixation. Recurrent instability was more likely to occur during sporting activity in male patients during their third decade of life. Further prospective trials are needed to determine the true relative risks of each particular surgical technique.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was waived by the University of Pittsburgh Medical Center Institutional Review Board (study #PRO15050410).