
Abstract
Background:
The Chinese unique inlay Bristow (Cuistow) procedure is a modified Bristow surgery in which an inlay (mortise-and-tenon) structure is added to the contact surface between the coracoid tip and the glenoid. Patients who have undergone the Cuistow procedure have had satisfying clinical performance and excellent postoperative bone healing rates (96.1%).
Purpose:
To compare the clinical and radiographic outcomes after the arthroscopic Cuistow procedure and the arthroscopic Bristow procedure.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 91 patients who underwent either the Cuistow or Bristow procedure between January 2017 and March 2018 were selected, and 69 patients (70 shoulders; 35 in the Cuistow group and 35 in the Bristow group) were included. Clinical assessment at minimum 24 months postoperatively, including the visual analog scale for pain and instability, American Shoulder and Elbow Surgeons score, Rowe score, subjective shoulder value score, and active range of motion, was completed by independent observers and compared with values collected preoperatively. Assessment with 3-dimensional computed tomography scans was performed preoperatively; immediately after the operation; at 3, 6, and 12 months postoperatively; and at the final follow-up.
Results:
A total of 69 patients (70 shoulders) were included, with a mean follow-up duration of 34.41 ± 5.99 months (range, 24-50 months). Both groups saw significant improvement in visual analog scale for pain and instability, American Shoulder and Elbow Surgeons, Rowe, and subjective shoulder value scores at the final follow-up compared with the preoperative values (P < .001 for all), with no significant between-group differences on any clinical outcomes at the final follow-up. The 3-month postoperative graft union rate on computed tomography was significantly higher in the Cuistow group compared with the Bristow group (82.9% vs 51.4%, respectively, P = .003), although the graft union rate at the final follow-up was not significantly different (94.3% vs 85.7%, respectively; P = .449).
Conclusion:
Patients receiving the Cuistow procedure had equivalent clinical outcomes and a significantly higher bone union rate at 3 months postoperatively than those in the Bristow group. The inlay structure used in the Cuistow procedure was found to be associated with accelerated bone union.
Anterior shoulder dislocation is the most common type of joint dislocation. 21 It will significantly affect the patient's activities of daily life and sports performance if not treated properly. In the treatment of traumatic anterior shoulder instability, patients with a large glenoid defect or younger age are at higher risk for recurrent instability after arthroscopic Bankart repair.1,12,28,29,37 Under these circumstances, bone grafting procedures are usually recommended.
Currently, the coracoid process transfer (Bristow or Latarjet procedure) is the bone grafting procedure most commonly used. The traditional Bristow or Latarjet procedure can reconstruct the shape of the glenoid and joint stability by the combination of the sling effect and bone-grafting effect, 39 but problems such as poor healing of the bone block5,13 and long rehabilitation period remain a concern.11,36 Moreover, the Bristow procedure was reported to have a lower bone union rate and an inferior biomechanical stabilizing effect than the Latarjet procedure,5,16 which may undermine postoperative recovery and lead to a premature end of a professional athlete's career; thus, it has lost popularity for a period of time. However, a recent comparative systematic review has shown that the Bristow procedure has equivalent clinical outcomes and has advantages in postoperative pain and osteoarthritis when compared with the Latarjet procedure, 13 which may lead to faster postoperative recovery and gain advantage in long-term performance. In addition, the bone union rate and stabilizing effect might be enhanced by using a more biomechanically effective structure or extra fixation. Therefore, the Bristow procedure has a theoretical and clinical basis to gain popularity once again.
On the basis of current Bristow procedure, our author group24,31 developed a procedure using an original inlay structure, called the Chinese unique inlay Bristow (Cuistow) procedure. The Cuistow procedure was inspired by the mortise-and-tenon structure in traditional Chinese architecture; this structure is added to the contact surface between the coracoid tip and the glenoid. In previous retrospective studies, it was found that patients who received the Cuistow procedure had an excellent postoperative bone healing rate (96.1%) and satisfying clinical performance through a 3-year follow-up.24,31,33
The purpose of the current study was to compare the clinical and radiological outcomes after the arthroscopic Cuistow procedure and the arthroscopic Bristow procedure. Our hypothesis was that patients receiving the Cuistow procedure would have a higher bone union rate and equivalent clinical outcomes compared with those undergoing the Bristow procedure.
Methods
Study Design and Participants
This was a retrospective comparative cohort study conducted at a single institution. Approval for this study was obtained from the medical science research ethics committee at our institution. All operations were performed in our department between January 2017 and March 2018 by the same senior surgeon (G.C.). All relevant data were gathered from existing medical records and radiographic images. The inclusion criteria were traumatic recurrent anterior shoulder instability treated by the Cuistow procedure or the Bristow procedure with (1) a glenoid defect ≥10% but <25%, (2) participation in high-demand (collision and overhead) sports combined with the presence of a glenoid defect <25% of the glenoid or without defect, or (3) failure after Bankart repair. The exclusion criteria included (1) multidirectional shoulder instability, (2) uncontrolled epilepsy, (3) pathological involvement of other soft tissue such as the long head of the biceps or a rotator cuff tear, (4) previous shoulder surgery other than Bankart repair, and (5) follow-up of <2 years or incomplete follow-up data.
A total of 91 patients who underwent either the Cuistow procedure or the Bristow procedure between January 2017 and March 2018 were selected, and 69 patients (70 shoulders) meeting the inclusion and exclusion criteria were included in this study. All patients provided informed consent. The patients were divided into 2 groups depending on the surgical procedure: the Cuistow group (n = 35 shoulders) and the Bristow group (n = 35 shoulders).
Surgical Technique
Patients in the Cuistow group received an arthroscopic Cuistow procedure according to the technique described by Lin et al, 24 in which we produced a mortise-and-tenon structure in the contact surface between the coracoid block and glenoid, making a bone groove on the glenoid neck at the 4-o’clock position and trimming the coracoid graft to fit the groove (Figure 1). Patients in the Bristow group received a modified arthroscopic Bristow procedure based on the technique described by Boileau et al, 4 and we freshened the cortex of the glenoid for the contact area during the glenoid preparation. All coracoid grafts in 2 groups were fixed by screws.

Schematic diagrams illustrating the Cuistow procedure.
Rehabilitation
Patients in both groups used the same set of training programs for postoperative rehabilitation under the guidance of a physical therapist. The sling was worn for 6 to 8 weeks, and no active movement was permitted within this period. After 8 weeks, the sling could be removed. Patients could start active training, resume normal gait, and gradually try to wash their faces and practice other daily activities with light pain or no pain. No active biceps contraction, such as pulling things, was permitted until 3 months postoperatively to reduce the risk of bone absorption and ensure solid bony union. Return to contact sports, throwing, or heavy labor activities were allowed 6 months after surgery with our assessment and permission. In our practice, we assess patients’ readiness to return to sport (RTS) with the following criteria: (1) bone union; (2) no pain or swelling around the operated shoulder; (3) approachable range of motion compared with the opposite side; (4) muscle strength or endurance recovery; and (5) negative release or relocation sign. Generally, if the patients meet more than 2 requirements, we allow them to attend leisure or noncontact sports. Return to contact sports, throwing, or heavy labor activities were generally allowed 6 months after surgery when the bone achieved solid union, full range of motion was restored, and no apprehension was demonstrated.
Clinical Outcome Assessment
The age at first injury and surgery, number of shoulder dislocations before surgery, occupation, competition level, and glenoid bone defect sizes were obtained from preoperative medical records. In addition, the visual analog scale for pain and instability, American Shoulder and Elbow Surgeons score, 26 Rowe score, 22 subjective shoulder value score, 15 and range of motion in different directions were recorded preoperatively. All of these measurements were also taken when patients were routinely seen postoperatively at 3, 6, and 12 months and then annually. Patients also completed the University of California, Los Angeles, shoulder score postoperatively. 22 Any complications that occurred intraoperatively or postoperatively were recorded.
The assessment of RTS status and time to RTS was included in the clinical assessment at the final follow-up. RTS status was determined by a 3-level classification method 27 : level 1, unable to RTS (the operative shoulder was unable to RTS); level 2, change in the type of sport or participation in competition at a lower level (the operative shoulder can participate only in exercises that are different from those before surgery or participate in sports at lower level); or level 3 (the operative shoulder is completely able to return at the same or higher level as before injury).
Computed Tomography Assessment
All patients underwent computed tomography (CT) scan evaluation with 3-dimensional reconstruction (3D-CT) preoperatively; immediately after the operation; at 3 months, 6 months, and 1 year postoperatively; and at the final follow-up (minimum of 2 years postoperatively). All CT scans were performed with the same protocol in our hospital.
The radiological measurements were evaluated by 2 independent examiners (H.W. and H.L.), who were blinded to the clinical outcomes. Both examiners were medical students (sixth year of an 8-year medical program) with expertise in sports medicine and radiology. Before beginning the measurements, both observers participated in training sessions using CT scans from an independent collective of patients managed before the study. Both examiners conducted 2 separate measurements for all CT scans in this study, with a 3-month interval between each measurement session.
Bone healing was observed on axial and sagittal 2-dimensional CT views, and it was defined as trabeculation or ossified density crossing the glenoid and bone block space in any slice of the CT images.7,19 The glenoid bone defect (Pico method), 2 Hill-Sachs lesion, and size of the coracoid were measured in preoperative 3D-CT according to validated methods in the literature.2,10,34 Bone graft positioning was validated in 2-dimensional and 3D-CT scans immediately after the surgery (within 2 days). The ideal position of the bone block was defined as 4-o’clock (for the right shoulder) on the en face view and flush to the anterior glenoid rim on the axial view.5,19,23 The bone block was considered too lateral if it went beyond the glenoid rim by more than 5 mm, and it was judged to be too medial if it was medial to the rim by more than 5 mm. 3 The alpha angle was defined as the angle between the axis of the screw (or the bone tunnel) and the glenoid rim. Bone absorption as shown on the latest CT scan was evaluated by a simplified validated classification method,24,40 in which the severity of the absorption was graded as 0 (no resorption), 1 (minor resorption), 2 (major resorption), or 3 (total resorption). All measurements on CT scans were performed via RadiAnt DICOM Viewer software (Version 2020.2.3; Medixant).
Statistical Analysis
The quantitative data were expressed as the mean and standard deviation, and qualitative data were described as sample sizes and/or percentages. Quantitative variables were compared using paired-samples t tests or nonparametric tests, depending on whether the data were distributed normally. Qualitative variables were compared using the chi-square test or Fisher exact test. The grade of graft resorption was compared using the Mann-Whitney-Wilcoxon test.
The interobserver and intraobserver reliability of the glenoid defect and graft position were assessed using the intraclass correlation coefficient (ICC). Interobserver reliability for bone union and the grade of graft absorption were evaluated using Cohen's kappa, while intraobserver reliability was determined using weighted kappa.
All data analysis was performed using the SPSS Statistics software (Version 26.0; IBM); P < .05 was considered statistically significant.
Results
The mean follow-up duration was 34.41 ± 5.99 months (range, 24-50 months). The mean age of the included study patients was 26.1 years (range, 13-60 years). The mean number of dislocations before surgery was 10.23, and the mean time between first dislocation and surgery was 5.8 years. The mean glenoid defect size measured on preoperative 3D-CT was 13.72% ± 6.31%. There were no significant differences with regard to the characteristics of the shoulders in the Cuistow and Bristow groups (Table 1).
Characteristics of the Study Groups (N = 70 Shoulders) a

Data are reported as mean ± SD or number of shoulders (%) unless otherwise indicated. BMI, body mass index.
Clinical and Functional Outcomes
In both groups, there were no significant differences in range of motion at the final follow-up compared with preoperative values except for external rotation at the side (51.9°± 10.7° vs 48.1°± 9.4° at final follow-up; P = .039). The final visual analog scale for pain, American Shoulder and Elbow Surgeons, Rowe, and subjective shoulder value scores were all improved significantly when compared with preoperative scores (P < .001 for all) (Table 2). When comparing functional outcomes between the Cuistow and Bristow groups, there were no significant differences on any measures at the latest follow-up (Table 3).
Clinical and Functional Scores Before Surgery and at Final Follow-up a

Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; ER, external rotation; IR, internal rotation; SSV, subjective shoulder value; VAS, visual analog scale.
Clinical and Functional Scores Between the Study Groups at Final Follow-up a

Data are reported as mean ± SD. ASES, American Shoulder and Elbow Surgeons; ER, external rotation; IR, internal rotation; SSV, subjective shoulder value; UCLA, University of California, Los Angeles; VAS, visual analog scale.
RTS and Professional Activities
At the time of the latest follow-up, all patients were able to RTS without redislocation. Of 35 shoulders in patients of competitive sports, 23 (66%) were able to resume at the same or a greater level. The status of patients’ RTS level and the percentages in each level were similar in both groups (P = .623) (Table 4). The time of RTS in the 2 groups was significantly different (P = .026). There were 15 shoulders (42.9%) in the Cuistow group that achieved RTS within the first 6 months postoperatively compared with 9 (25.7%) in the Bristow group that fulfilled this standard within the same period of time (Table 4).
Level and Time of RTS and Activities in Study Groups a

Data are reported as n (%). Boldface P value indicates statistically significant difference between groups (P < .05). RTS, return to sports.
CT-Based Outcomes
For interobserver reliability, the ICC of the CT measurements ranged from 0.855 to 0.975 for all of the evaluations, indicating excellent reliability. For intraobserver reliability, the ICC of repeated CT measurements (after a 3-month interval) ranged from 0.870 to 0.985 for all of the evaluations, also indicating excellent reliability.
Graft Position
Postoperative CT scanning showed that the median position of the transferred bone block was at the 4:30-o’clock position (from 4-o’clock to 5-o’clock) on the sagittal view (right shoulder). The mean alpha angle was 18.5°± 5.2°, with 7 (10.0%) of 70 screws being overangulated (alpha angle >25°). On the axial view, the graft position was considered to be flush in 64 shoulders (91.4%), medial in 4 (5.7%), lateral in 2 (2.9%), and too medial or too lateral in none.
Graft Healing and Absorption
The graft healing rate was significantly higher in the Cuistow group at the 3-month follow-up (82.9% vs 51.4% for the Bristow group; P = .003); however, the difference was not significant at the final follow-up (P = .449) (Table 5). Overall, 8 patients had grade 0 bone absorption, 34 had grade 1 bone resorption, 22 had grade 2 bone resorption, and 6 patients had grade 3 bone resorption at the latest follow-up. No significant differences between the Cuistow and Bristow groups were detected regarding degree of bone resorption (P = .282) (Table 6). No arthropathy was observed in any patient. Representative images of bone union and osteolysis of coracoid grafts are shown in Figure 2.
Graft Healing Rate at the 3-Month and Final Follow-ups in the Study Groups a
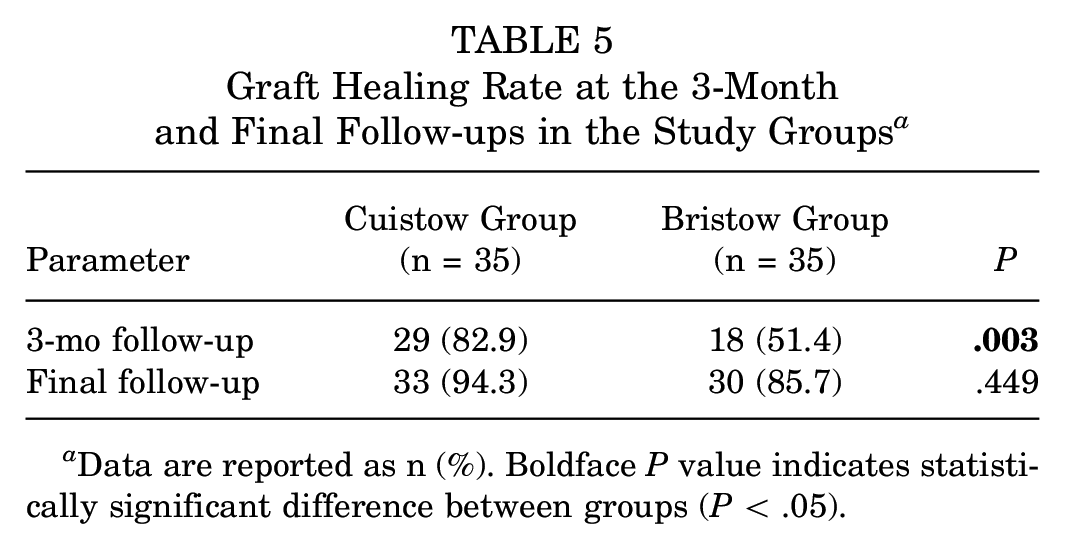
Data are reported as n (%). Boldface P value indicates statistically significant difference between groups (P < .05).
Graft Resorption at the Final Follow-up in the Study Groups a

Data are reported as n (%).

Graft positioning and remodeling on computed tomography of a right-handed male patient who underwent the Cuistow procedure in his left shoulder in 2018 (age, 24 years) and the Bristow procedure in his right shoulder in 2017 (age, 23 years). (A) Illustration of the Cuistow procedure. (B-E) Postoperative bone graft healing on 2-dimensional axial view immediately after the Cuistow procedure and at 3 months, 6 months, and final follow-up, respectively. (F) Illustration of the Bristow procedure. (G-J) Postoperative bone graft healing on 2-dimensional axial view immediately after the Bristow procedure and at 3 months, 6 months, and final follow-up, respectively.
Complications
At a mean follow-up of 34.4 months, no major complications (eg, redislocation, hematoma, infection, glenohumeral joint arthropathy, or stiffness of the shoulder joint) were recorded after either type of surgery; 1 patient in the Cuistow group and 1 patient in the Bristow group had intraoperative coracoid graft fracture. The screw could not be tightened during the operation in 2 patients in the Cuistow group. The conjoint tendon was scalded in 1 patient in the Cuistow group. Two patients in the Bristow group had transient nerve palsy - 1 for the musculocutaneous nerve and 1 for the axillary nerve; both of them recovered within 12 weeks postoperatively. Two patients in the Cuistow group and 5 patients in the Bristow group failed to achieve bone union at the latest follow-up. One patient in the Cuistow group reported a subjective feeling of unstable but not subluxation or dislocation 2 years postoperatively. One patient in the Bristow group underwent another rotator cuff repair surgery 8 months postoperatively because of the tear and clicking caused by a type 2 acromion.
Discussion
In the current study, 82.9% of shoulders in the Cuistow group achieved bone union 3 months after surgery, compared with 51.4% of shoulders in the Bristow group during the same period (P = .003). In other words, patients who received the Cuistow procedure required less time to achieve bone union than those in the Bristow group; thus, it appears that the inlay structure used in the Cuistow procedure accelerated bone union.
When considering the bone-block procedure for shoulder instability, the relatively low bone union rate (73%-85%) of the Bristow procedure remains a major concern.5,6,19,25 An increasing number of researchers have argued recently that postoperative bone healing is a key factor affecting postoperative functional recovery.25,38 Makihara et al 25 performed a clinical evaluation and imaging analysis of 23 patients who underwent the Bristow procedure, and found that the Rowe score and Walch-Duplay score of nonhealing patients were significantly lower compared to those of patients who achieved bone healing. They concluded that bone healing between the bone block and glenoid was a key factor affecting postoperative bone resorption and clinical outcomes. Willemot et al 38 included patients who had undergone revision surgery for postoperative redislocation after the Bristow or Latarjet procedure, and they found that nonhealing was the most crucial trigger for revision after the Bristow or Latarjet process, followed by bone resorption, bone block fracture, and malposition of the bone block. Tasaki et al 35 also reported that nonunion of the transferred coracoid was associated with significantly lower Rowe scores in collision athletes.
When compared with recent works in the literature reporting the clinical and radiographic outcomes of the modified Bristow procedure, the occurrence rate of nonunion of the transferred coracoid in this study was relatively low in both groups. In studies conducted by Boileau et al 5 and Gendre et al, 14 the coracoid union rate for arthroscopic Bristow surgery with suture-button fixation was only 74%, and the union rate with screw fixation was 73%. Regarding open Bristow surgery, a retrospective study conducted by Hovelius et al 19 reported bony healing in 83% with at least 5 years of follow-up. Therefore, we improved coracoid healing by incorporating a mortise-and-tenon structure, and we believe this structure is an ideal way to solve the lower bone healing rate of Bristow surgery. In addition to the high healing rate, patients in the Cuistow group showed excellent clinical results as indicated by functional scores at the final follow-up, and the RTS and redislocation rates achieved were quite competitive when compared with those of other studies (Appendix Table A1).
Why did the patients who underwent the Cuistow procedure have such an advantage in bone healing rate and speed of bone healing compared with those who underwent the Bristow procedure? We speculate that this may be related to biomechanical and biological factors. Biomechanically, the mortise-and-tenon structure itself has a better ability to resist shear and torque. The mortise-and-tenon structure also increases the contact area between the bone block and the glenoid, thus increasing friction and making it possible to resist pull from the conjoint tendon during biceps contraction, improving the stability of the bone block fixation system in the early postoperative period, thereby accelerating bone healing and increasing the long-term bone healing rate. By performing finite element simulations, Sano et al 30 found that the medial proximal bone block experienced the most evident stress shielding after the Latarjet procedure. Their results are consistent with previous clinical reports,9,17,40 demonstrating that the most significant bone resorption was located in the proximal part of the bone block. Therefore, we hypothesized that the mortise-and-tenon structure can moderate the postoperative stress shielding experienced by the transferred bone block and avoid the occurrence of bone resorption, thus contributing to the healing of the coracoid with the glenoid.
With regard to the biological aspect, the mortise-and-tenon structure allows for adequate blood supply provided by cancellous-to-cancellous bone contact, thus allowing the transferred bone block to receive more blood flow and factors that may promote bone healing from the glenoid. Since it has been shown that the blood supply to the bone block is cut off after the Latarjet procedure, 18 and that there is no vascularity in the conjoint tendon, 8 it seems that the blood flow from the glenoid side is of vital importance. In this regard, Kawasaki et al 20 and Shibuya et al 32 added a 3- to 8-mm socket to the anterior aspect of the glenoid during a modified Bristow procedure, which is similar to our idea of mortise-and-tenon construction. The socket also increases the contact between the bone block and the glenoid, thus potentially improving material exchange between these 2 parts. They also reported a significant increase in both short- and long-term postoperative bone healing rates, thus confirming our belief that increased contact between the 2 could improve bone healing rates. More basic experiments are needed to confirm the blood flow status between the articular glenoid and the transferred bone block.
Limitations and Strengths
There are several limitations to this study. First, the procedures were performed at a single institution by an experienced surgeon, and we performed a training session of CT measurement for observers before the study. Therefore, the results may not be generalizable. Second, longer follow-up and further study are needed to definitively confirm the reliability and effectiveness of the procedure. Finally, biomechanical and biological studies should be performed to investigate the mechanism by which the inlay structure accelerates bone union.
On the other hand, our study has several strengths. Preoperative and postoperative standardized CT imaging was performed for all patients to assess the bone graft union and positioning accuracy. Moreover, the groups were homogenous, with no significant difference in terms of sex, occupation, level of sports, or glenoid bone defect, making the comparison of 2 groups convincible.
Conclusion
The findings of the current study indicated that patients receiving the Cuistow procedure had equivalent clinical outcomes and a significantly higher bone union rate at 3 months postoperatively than those in the Bristow group. The inlay structure used in the Cuistow procedure was found to be associated with accelerated bone union.
Footnotes
Appendix
Comparison of Current Study Results With Previous Reports a

| Authors (year) | Type of Surgery | Other Surgery Techniques | Mean Follow-up, mo | No. of Shoulders Involved | Redislocation Rate | Bone Union Rate | RTS Rate | |
|---|---|---|---|---|---|---|---|---|
| 3 mo Postop | Latest Follow-up | |||||||
| Hovelius et al (2012) 19 | Bristow-Latarjet procedure | Coracoid placed in “standing” position. Capsulopexy | >60 | 319 | 1% | - | 83% | - |
| Boileau et al (2014) 5 | 2B3 procedure | Arthroscopic Bristow-Latarjet combined with Bankart repair | 35 | 70 | 2% | - | 73% | 83% (n = 58) at preinjury level |
| Kawasaki et al (2018) 20 | Bristow procedure with Bankart repair | The anteroinferior cortex of the glenoid was deepened by approximately 5-8 mm to provide an indented bed of cancellous bone (rectangular and approximately 12 mm long) adjacent to the glenoid rim for placement of the coracoid graft | 51.5 | 176 (152 competitive rugby players) | 3.4% | - | 89.2% | 93.2% of shoulders returned to preinjury level at a mean of 6.3 mo postop |
| Makihara et al (2019) 25 | Modified Bankart and Bristow procedure | - | 19.2 | 23 | - | - | 78.3% | - |
| Shao et al (2020) 31 | Inlay Bristow procedure | - | 36.1 | 56 | 0 | - | 96.4% | 98% (55 of 56) returned to preinjury level or higher |
| Lin et al (2021) 24 | Chinese unique inlay Bristow procedure | Mortise-and-tenon structure added to the contact face | 41.5 | 63 | 0 | - | 96.1% | 87.0% at latest follow-up |
| Clowez et al (2021) 6 | Bristow-Latarjet procedure | - | 89 | 59 | 7% | - | 85% (53 patients with postop CT) | Overall: 91% (53/58); 70% (37/53) returned to their previous discipline, 46% (17/37) returned at the same level; 35% (11/31) practicing their sport in competition resume at a high level |
| Shibuya et al (2021) 32 | Bristow and Latarjet procedures | Bristow and Latarjet procedures with Bankart repair and an indented 3- to 5-mm bed created in the anteroinferior cortex of the glenoid | 32.7 | 169 (154 competitive rugby players) (Bristow: 92; Latarjet: 77) | 1.2% (both of them underwent Bristow procedure) | • Bristow: 89.1% • Latarjet: 92.2% |
- | 92.3% returned to their preinjury level at a mean of 5.9 mo postop; 9.8% in Bristow group and 5.2% in Latarjet group returned at a lower level |
| Present study | Cuistow procedure and modified Bristow procedure | • Cuistow: Mortise-and-tenon structure added to the contact face • Bristow: Bristow procedure with Bankart repair and fully freshened glenoid cortex |
34.4 | 70 (of 69 patients) (Cuistow: 35; Bristow:35) | 0 | • Cuistow: 82.9% • Bristow: 51.4% |
• Cuistow: 94.3% • Bristow: 85.7% |
34% (12/35) in Cuistow group returned at a lower level; 66% (23/35) of competitive players resume at the same or higher level. RTS rate and level were identical in both groups |
Postop, postoperative; RTS, return to sport.
Final revision submitted October 29, 2023; accepted November 15, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: this study was supported by the National Natural Science Foundation of China (82172423, 81871770, 81802161), Beijing Natural Science Foundation (7222209), and Capital's Funds for Health Improvement and Research (Z171100001017092). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital (ref No. M2021039).