
Abstract
Background:
Recent data suggest that inaccurate suture passage during remplissage may contribute to a loss of external rotation, with the potential to cause posterior shoulder pain because of the proximity to the musculotendinous junction.
Purpose:
To evaluate the accuracy of suture passage during remplissage and identify surface landmarks to improve accuracy.
Study Design:
Descriptive laboratory study.
Methods:
Arthroscopic remplissage was performed on 6 cadaveric shoulder specimens. Two single-loaded suture anchors were used for each remplissage. After suture passage, position was recorded in reference to the posterolateral acromion (PLA), with entry perpendicular to the humeral surface. After these measurements, the location of posterior cuff penetration was identified by careful surgical dissection.
Results:
Twenty-four sutures were passed in 6 specimens: 6 sutures (25.0%) were correctly passed through the infraspinatus tendon, 12 (50%) were through the infraspinatus muscle or musculotendinous junction (MTJ), and 6 (25%) were through the teres minor. Suture passage through the infraspinatus were on average 25 ± 5.4 mm inferior to the PLA, while sutures passing through the teres minor were on average 35.8 ± 5.7 mm inferior to the PLA. There was an odds ratio of 25 (95% CI, 2.1-298.3; P < .001) that the suture would be through the infraspinatus if the passes were less than 3 cm inferior to the PLA. Sutures passing through muscle and the MTJ were significantly more medial than those passing through tendon, measuring on average 8.1 ± 5.1 mm lateral to the PLA compared with 14.5 ± 5.5 mm (P < .02). If suture passes were greater than 1 cm lateral to the PLA, it was significantly more likely to be in tendon (P = .013).
Conclusion:
We found remplissage suture passage was inaccurate, with only 25% of sutures penetrating the infraspinatus tendon. Passing sutures 1 cm lateral and within 3 cm inferior of the PLA improves the odds of successful infraspinatus tenodesis. We recommend this “safe zone” to improve the odds of infraspinatus tenodesis during remplissage. These results may help improve remplissage techniques and prevent previously reported complications, including external rotation loss and pain from myodesis.
First described in 1940, 11 Hill-Sachs lesions have a reported prevalence of up to 70% in first-time dislocators 24 and up to 90% in recurrent instability. 2,26,28 These lesions frequently contribute to recurrent instability episodes requiring surgical management. Several techniques have been described for the management of Hill-Sachs lesions. 5,10,13,22 Of these options, the remplissage procedure has gained acceptance as a reliable surgical technique that is minimally invasive while providing improvement in clinical outcome scores. 3,20,29 Despite low recurrence rates after remplissage, concerns have existed for decreased external rotation. 6,14,17 In a recent cadaveric study, Elkinson et al 7 investigated the role that suture anchor location had on postoperative range of motion after arthroscopic remplissage. While they did not identify a difference in motion between specimens with anchor placement on the rim or “in the valley” of the Hill-Sachs lesion, they did identify that sutures passed 1 cm more medial than desired through the infraspinatus tendon significantly increased joint stiffness and limited external rotation. The authors cautioned us over the effects of suture medialization; however, no specific landmarks or surgical techniques were suggested to guide proper placement for posterior suture passage to prevent this complication.
Over the past 5 years, the clinical literature has assumed that the remplissage procedure functioned as a tenodesis of the infraspinatus into the Hill-Sachs lesion, as originally described. 20,21,29 However, limited evidence exists to support this, as most cadaveric studies have failed to evaluate the accuracy of arthroscopic suture passage as the procedure has been performed in an open fashion by direct visualization of the infraspinatus tendon and subsequent suture passage. 1,7,8,17 Recent work by Lädermann et al 12 demonstrated that even when arthroscopic remplissage is performed by fellowship-trained surgeons, sutures are frequently misdirected into the teres minor or even the infraspinatus muscle belly, resulting in a myodesis rather than tenodesis. Given these recent findings, further study is needed to quantify the malposition of sutures and investigate ways to improve the surgical technique of remplissage.
The primary purpose of this cadaveric study was to further evaluate the accuracy of suture passage and anchor placement during remplissage. The secondary goal was to identify extra-articular landmarks to improve placement of posterior anchors.
Methods
Six fresh-frozen cadaveric shoulders including the entire upper extremity were used for this study. The mean donor age was 66.4 years, with 4 females and 2 males. No significant shoulder pathology was found in the specimens. All shoulders were mounted to produce a simulated beach-chair position. The shoulder was secured in the desired position by use of a large metallic clamp placed along the medial scapular border. The scapula was mounted to ensure the glenoid was perpendicular to the floor and to simulate its anatomic position. For humeral rotation, we used the distal epicondyles to maintain neutral rotation and kept them parallel with the coronal plane of the upper extremity cadavers.
A fellowship-trained shoulder surgeon performed all procedures. The surgeon was blinded to measurements between each procedure, and a separate research staff performed all dissections. Creation of a Hill-Sachs lesion would have limited the ability to perform an arthroscopic procedure, similar to the concerns of Lädermann et al. 12 As a result, the location of anchor placement was based on the theoretical “off track” Hill-Sachs location previously described 23,25 (see Figure 1). Furthermore, each anchor was placed into the deepest part of the valley of the theoretical Hill-Sachs defect to minimize overmedialization, as described by Elkinson et al 7 .
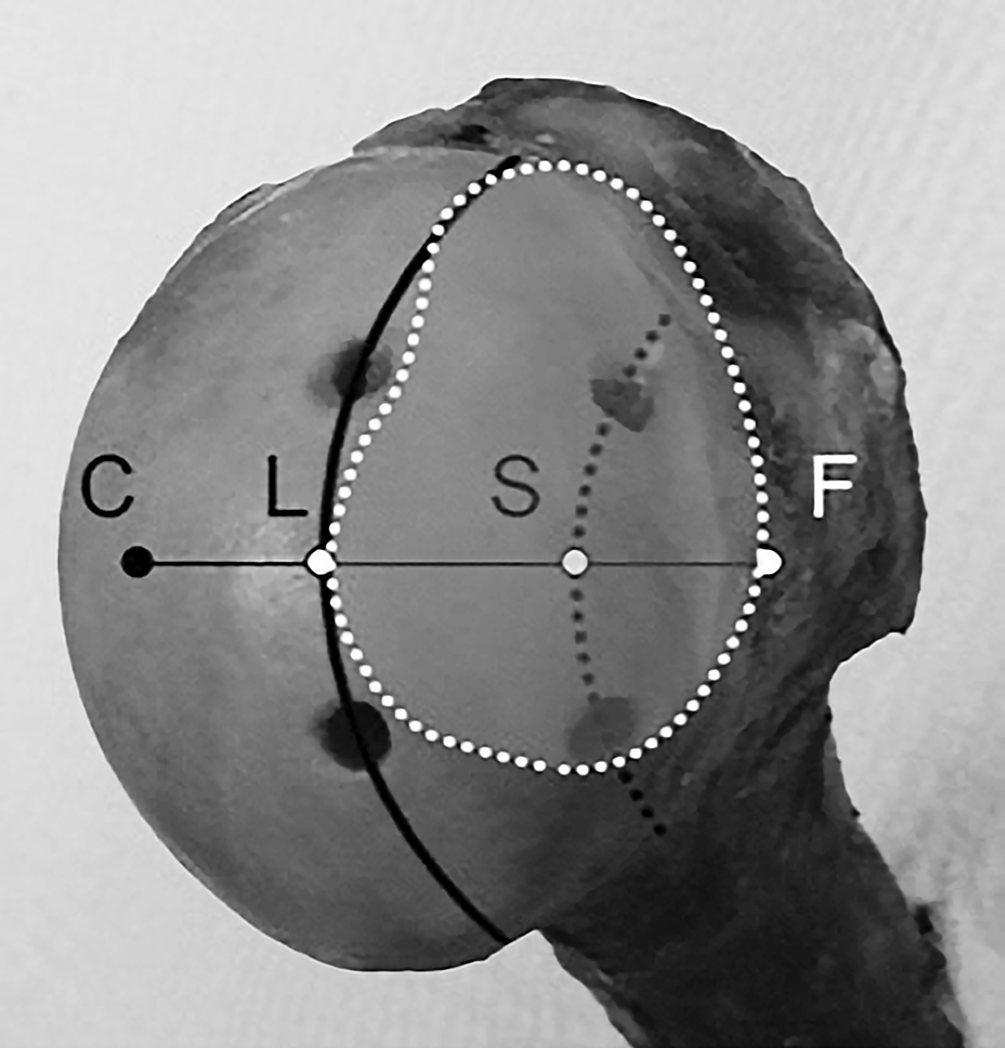
Appropriate anchor placement into a “theoretically” large Hill-Sachs lesion (L), as defined by Omi et al. 17 The dotted trajectory (S) defines the line for placement into the valley of a large Hill-Sachs lesion. Reprinted with permission from Omi et al. 17 C, center of the humeral head; F, bare spot.
An arthroscopic remplissage procedure was also performed similar to previous reports. 3,19,21 A standard posterior portal was used for initial diagnostic arthroscopy, which was roughly 1 cm medial and 2 cm inferior from the posterolateral acromion (PLA). After excluding any significant concomitant shoulder pathology, an anterior portal was established through the rotator interval. Using a switching stick, the camera was placed anteriorly to evaluate the posterior humeral surface. The arm remained in a position of neutral rotation and humeral adduction for anchor placement, as previously described. 19,20 Two 3-mm single-loaded anchors (SutureTak; Arthrex Inc) were used for each specimen. Through a percutaneous posterior portal similar to placement by Boileau et al, 3 a superior anchor was placed 5 mm inferior to the superior portion of the bare spot and 3 to 5 mm medial to it to simulate an “off-track” Hill-Sachs lesion. 12,18,25 All intraoperative measurements were made using a calibrated probe. The second anchor was placed 1 cm inferior to the first anchor, as it has been demonstrated that placement ≥2 cm apart increases the chance of teres minor penetration. 12
For each anchor, both suture limbs were passed in a horizontal mattress configuration. Initially, all 4 limbs were shuttled through the posterior portal cannula. With the use of a spinal needle and a 4-0 Prolene suture, all limbs were passed separately through the posterior capsule and rotator cuff. All spinal needle trajectories were similar for percutaneous passes, and care was taken to keep the needle perpendicular to the humeral head, similar to previous studies. 12 Corresponding pairs of sutures were then marked for easier identification during dissection and measurements. It should be noted that care was taken to avoid overmedialization during suture passage. 7
Once all suture limbs had been arthroscopically passed and marked, dissection of the shoulder was performed, removing all skin, subcutaneous tissue, deltoid, and bursa. All skin, deltoid, and subcutaneous fat was left preserved on the PLA for measurement purposes. Care was taken not to transect any of the passed sutures. The rotator cuff was preserved during dissection. The exit point of each suture limb was recorded with respect to the posterior lateral acromion (soft tissue was still attached to the PLA), with all limbs being held perpendicular to the humeral head to mimic similar entry and angle of the needles during the initial procedure. The arm was kept in neutral rotation with humeral adduction during all measurements. A superiorly directed force was manually applied at the elbow to prevent any inferior joint distraction. All measurements were done with a manual caliper and were confirmed by 2 other observers. These measurements were performed at the level of the remaining soft tissue PLA as to decrease any bias from variation between specimen size and habitus. Both the inferior and lateral distance from the posterior lateral acromion were recorded. In addition, the exit location through the rotator cuff was recorded (infraspinatus or teres minor), and the medial-lateral location was also recorded (muscle, musculotendinous junction [MTJ], or tendon) (Figure 2).

A posterior dissection with separation of all 4 suture limbs. The exiting posterior structure was recorded for each limb.
For further measurements, the axillary nerve was also dissected out as well. The footprints of the infraspinatus and supraspinatus insertion were defined during the dissection based on work by Mochizuki et al. 15 After all measurements were documented, the sutures were tied with a surgeon’s knot to each corresponding anchor. The distance from each knot to the middle of the infraspinatus footprint 15 and the superior distance from the axillary nerve were documented.
After extra-articular landmarks were assessed, the supraspinatus, infraspinatus, and teres minor were incised from their medial attachments to gain access to the glenohumeral joint. Additionally, sutures were excised, leaving only the anchors for final measurements. Distance from the posterior medial-most aspect of the footprint of supraspinatus insertion was recorded similar to that by Lädermann et al. 12
Statistical Analysis
Descriptive statistics were used to describe distances from the suture passes to the anatomic landmarks of interest. Student t tests were then used to compare continuous variables, and chi-square/Fischer exact tests were used to compare categorical variables. Tests were conducted using 2-sided hypothesis testing with statistical significance set at P ≤ .05 and conducted using SPSS (v 19.0; IBM Corp).
Results
Remplissage was performed in 6 cadaveric specimens with 12 anchors placed and 24 sutures passed. Six sutures (25%) were through the infraspinatus tendon and 12 (50%) were through the infraspinatus muscle (n = 4) or MTJ (n = 8). The remaining 6 sutures were in the teres minor (muscle) (n = 1) or MTJ (n = 5).
Extra-articular Measurements
The mean inferior distance from the PLA for the superior anchor limbs was 26.3 ± 8.5 and 25.2 ± 5.6 mm. The mean lateral distance for the superior anchor limbs was 7.5 ± 4.3 and 10.8 ± 9.3 mm. For the inferior suture limbs, the mean inferior distance was 31.2 ± 5.6 and 28.2 ± 8.7 mm, and the mean lateral distance was 10.5 ± 3.5 and 10.0 ± 5.4 mm (Table 1).
Suture Passage Measurements

a Negative value = medial. Infra, infraspinatus; MTJ, musculotendinous junction; PLA, posterolateral acromion.
The distance from the lateral insertion of the infraspinatus was on average 38.5 ± 3.2 mm for the inferior anchor and 35.2 ± 5.2 mm for the superior anchor. The mean distance from the axillary nerve was 45.7 ± 17 mm for the inferior anchors and 52.8 ± 15.9 mm for the superior anchor. The mean distance from the posterior supraspinatus insertion was 21.2 ± 7.2 mm for the inferior anchor and 16.7 ± 6.8 mm for the superior suture.
Comparative Analysis
For sutures passing through the infraspinatus, the mean inferior distance from the PLA was 25.0 ± 5.4 mm compared with sutures passing through the teres minor, which measured 35.8 ± 5.7 mm inferior to the PLA (P < .001). If sutures were passed within 3 cm inferior to the PLA, there was an odds ratio of 25 (95% CI, 2.1-298.3) that they were successfully passed through the infraspinatus (P = .006).
Suture passes in muscle and the MTJ were significantly more medial relative to the PLA, measuring on average 8.1 ± 5.1 mm lateral compared with sutures through tendon at 14.5 ± 5.5 mm (P < .02). If sutures were passed more than 1 cm lateral to the PLA, significantly more were in the tendon (6/6) compared with sutures passed less than 1 cm lateral to the PLA (6/12) (P = .013). As a result, passing 1 cm lateral to the PLA significantly increased the chances of tendon penetration (Figure 3).

The suggested safe zone is demonstrated. Staying 1 cm lateral and within 3 cm inferior of the posterolateral acromion significantly improves passage through the infraspinatus tendon.
Discussion
In this study, we found placement of anchors and suture passage through the posterior rotator cuff was completely variable. Only 25% of remplissage sutures were passed through the infraspinatus tendon. Referencing the posterolateral acromion, we demonstrated staying 1 cm lateral and within 3 cm inferior with each suture passage significantly improved the chances of passage through the infraspinatus tendon. Limited studies have evaluated the technical aspects of remplissage. 7,12 Despite attempts, a detailed evaluation of suture passage has not been performed. As remplissage continues to demonstrate clinical success, 3,20,29 further study is needed to identify landmarks to prevent posterior muscle damage and external rotation loss from inaccurate suture passage. 12 This study represents the first to our knowledge to provide surface landmarks to facilitate and improve the accuracy of suture passage during arthroscopic remplissage.
For the past decade, remplissage has been used for “off track” Hill-Sachs lesions and has been described as a tenodesis of the infraspinatus into the humeral head defect. 19,21,27 The results of this current study demonstrate that only 25% of sutures pass through the infraspinatus tendon during remplissage. This is consistent with previous studies that reported only 5% of remplissage sutures were located in the infraspinatus tendon. 12 These results suggest that rather than being a true capsulotenodesis of the infraspinatus, remplissage is more often a capsulomyodesis. One clinical concern is that this may be a reason for 30% of patients reporting posterior shoulder pain after remplissage. 16 Our study corroborates these findings, with only 25% of sutures passed in their desired location through the infraspinatus tendon and the remaining sutures all passing at or medial to the musculotendinous junction, potentially predisposing to pain if performed in this manner. Furthermore, myodesis versus tenodesis may decrease pullout strength and contribute to remplissage failure rates of up to 15%. 4,20,27 Biomechanical analysis is needed to evaluate whether muscle entrapment decreases stability, though a better option is to identify methods to decrease muscle penetration during remplissage.
Many studies have demonstrated insignificant range of motion deficits after remplissage, 3,4 though concerns still exist over reported external rotation deficits. 7,14,17 Even with small losses of only 2° to 8°, 3,4,19 the effects may have a greater impact in overhead athletes. 9 One explanation for external rotation loss may be due to overmedialization of suture placement. Elkinson et al 7 found placing anchors 1 cm more medial to the desired position in the posterior capsule significantly increased joint stiffness and reduced range of motion. The major limitation with this study was that the “desired position” for suture passage during the remplissage procedure was not reliably quantified or described, with no guidelines provided to prevent further suture medialization. Additionally, all procedures were done in an open manner, with direct visualization of the infraspinatus tendon, so the clinical application of these results to arthroscopic methodology is difficult. Despite being aware of the pitfalls of overmedialization, 54% of the sutures were still inadvertently passed through the MTJ and 20% in the muscle, similar to findings reported by Lädermann et al. 12 Given these results, this current study demonstrates a more quantifiable way to avoid overmedialization using external landmarks. We found staying 1 cm lateral to the posterior lateral acromion was the best predictor of appropriate passage through tendon. This clinical finding will aid in placement of posterior suture anchors and may be a more reliable marker to prevent overmedialization.
Biomechanically preventing medialization is necessary to limit external rotation loss, though superior-inferior placement of sutures has not been evaluated and may also be clinically relevant. In this study, we found anchoring of the teres minor occurred in 25% of suture passes. This is similar to previous reports. 12 Theoretically, anchoring of a more posteroinferior structure could lead to more global limitations in range of motion and may be another explanation for motion loss after remplissage. 8 Based on the results of this study, teres minor penetration can be minimized by passing sutures less than 3 cm inferior to the posterolateral acromion. We have demonstrated this safe zone for increasing probability of infraspinatus tendon penetration in Figure 2.
This study focused on reproducible extra-articular landmarks to improve accuracy of the remplissage. While we found the posterolateral acromion to be a good extra-articular landmark, intra-articular consideration of anchor separation is also important. Lädermann et al used a distance of 12 mm from the medial rotator cuff insertion as their reference guide for anchor placement 12 and reported they could consistently place anchors within 3 mm of this desired location. The issue with this landmark is it is only a medial reference point and does not a give superior-inferior reference. In evaluating the importance of referencing intra-articularly, medial references are less clinically important as it has been recommended that anchors be placed in the valley of the defect. 7 The medial-lateral location of the anchor will consequently be dictated by the size of each Hill-Sachs lesion rather than predefined distances. 7 If placing a second anchor during remplissage, we found placing the next anchor 1 cm inferiorly to be a good guideline. This smaller distance between anchors may have been the reason we had 15% less teres minor penetration than Lädermann et al, 12 who used 2 cm of inferior anchor separation. Overall, intra-articular distances of anchor separation should be taken into account and may aid in performing posterior capsulodesis of the remplissage procedure.
This study is not without limitations. As with many cadaveric studies, one of the limitations was the small sample size. Only 25% of sutures passed through the infraspinatus tendon; a larger sample of cadavers may have had less muscle penetration and improved accuracy. No biomechanical analysis was performed so the associations made with placement of sutures and clinical relevance is based on previous literature. Furthermore, the distance from the PLA may change with body habitus, needle trajectory, and soft tissue swelling, though our methods attempted to optimally control for this variation. This is the reason we have suggested a zone rather than exact location in anticipation of this variability. We also maintained similar trajectory throughout the protocol. Finally, we performed measurements at the level of the soft tissue of the PLA and recommend marking the “safe zone” before arthroscopy to limit variation with shoulder swelling. Also, measurements and the recommended “safe zone” are only reproducible for arms in neutral abduction and external rotation, which may not translate to patients operated on in the lateral decubitus position. Ideally, creation of an “off-track” Hill-Sachs lesion would have improved the study, though no current method allows for an arthroscopic procedure to be performed after lesion creation, and as a result, this was not feasible. 7,8 In addition, previous studies using arthroscopic methods have used a similar theoretical Hill-Sachs lesion. 12,17 Further biomechanical and clinical testing of these suggested landmarks is needed. Overall, this is the first study to demonstrate the inaccuracies of suture passage and suggest technical landmarks to improve remplissage.
Conclusion
Suture passage during remplissage is inaccurate using previously described techniques. Only 25% of sutures appropriately passed through the infraspinatus tendon, while the remaining 75% were in the muscle belly, musculotendinous junction, or teres minor. Passing sutures 1 cm lateral and within 3 cm inferior to the PLA significantly improved the chances of placing them in the infraspinatus tendon. Following these “safe zone” suggestions may reduce complaints of posterior shoulder pain associated with muscular damage from medial suture placement while also reducing the incidence of limited external rotation after remplissage.
Footnotes
Acknowledgment
The authors would like to thank Natasha Garcia for her assistance with the photography required for this manuscript.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.S.D. is a consultant for Arthrex.