
Abstract
Background:
Meniscal allograft transplantation (MAT) is performed to improve symptoms and function in patients with a meniscal-deficient compartment of the knee. Numerous studies have shown a consistent improvement in patient-reported outcomes, but high failure rates have been reported by some studies. The typical patients undergoing MAT often have multiple other pathologies that require treatment at the time of surgery. The factors that predict failure of a meniscal allograft within this complex patient group are not clearly defined.
Purpose:
To determine predictors of MAT failure in a large series to refine the indications for surgery and better inform future patients.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients undergoing MAT at a single institution between May 2005 and May 2014 with a minimum of 1-year follow-up were prospectively evaluated and included in this study. Failure was defined as removal of the allograft, revision transplantation, or conversion to a joint replacement. Patients were grouped according to the articular cartilage status at the time of the index surgery: group 1, intact or partial-thickness chondral loss; group 2, full-thickness chondral loss 1 condyle; and group 3, full-thickness chondral loss both condyles. The Cox proportional hazards model was used to determine significant predictors of failure, independently of other factors. Kaplan-Meier survival curves were produced for overall survival and significant predictors of failure in the Cox proportional hazards model.
Results:
There were 125 consecutive MATs performed, with 1 patient lost to follow-up. The median follow-up was 3 years (range, 1-10 years). The 5-year graft survival for the entire cohort was 82% (group 1, 97%; group 2, 82%; group 3, 62%). The probability of failure in group 1 was 85% lower (95% CI, 13%-97%) than in group 3 at any time. The probability of failure with lateral allografts was 76% lower (95% CI, 16%-89%) than medial allografts at any time.
Conclusion:
This study showed that the presence of severe cartilage damage at the time of MAT and medial allografts were significantly predictive of failure. Surgeons and patients should use this information when considering the risks and benefits of surgery.
Meniscal allograft transplantation (MAT) has been performed for over 30 years and is now a well-established treatment option for relatively young patients with symptomatic meniscal deficiency. 16 MAT has traditionally been contraindicated in the presence of full-thickness articular cartilage loss as it is thought that the biomechanical environment would not be favorable, resulting in a high failure rate. 2,7,9,12 However, up to 50% of patients present with this level of advanced chondral damage and have very low functional scores. 14,22 These patients represent a treatment challenge, and some studies have looked to extend the indications of MAT by performing concomitant chondral repair procedures with promising clinical outcomes. 1,4,5,15,18 It is important to know whether the cartilage status or other factors at the time of surgery have a significant effect on failure rate to determine whether MAT is a viable surgical intervention for this challenging patient group.
Other factors may also influence the risk of failure. Additional procedures at the time of MAT are commonly reported in the literature. 16 Malalignment and ligament instability are considered contraindications to MAT unless corrected intraoperatively. These patients have been shown to have an up to 4 times greater complication rate and may have a greater failure rate. 3 Lateral MAT is performed proportionately more commonly than medial. It is thought the relative increased importance of the lateral meniscus makes lateral meniscectomy a more destructive procedure than medial meniscectomy. It is not clear whether this may be a risk factor for failure, but some studies have shown medial MAT to have greater failure rates. 20,21 Graft source may also alter the risk of failure. While allografts are no longer irradiated, there remains the potential to affect the structural integrity of the allograft in the preparation stage. Each tissue bank uses different proprietary cleansing methods; some preservation methods have historically increased failure rates. 3,10
The aim of this study was to determine the factors that predict failure of MAT in a large series to refine the indications for surgery and better inform future patients.
Methods
All patients undergoing MAT at the University Hospitals Coventry and Warwickshire (Coventry, United Kingdom [UK] ) between May 2005 and May 2014 were prospectively evaluated as part of an ongoing service evaluation. Data collection was undertaken in compliance with the UK Governance Arrangements for Research Ethics Committees policy. The study was registered with the local research, development, and innovation department of our hospital.
Patients were eligible for MAT if they were younger than 50 years and were experiencing pain with a history of total or subtotal meniscectomy in the same compartment of the knee. Each patient was assessed for suitability for MAT by combination of magnetic resonance imaging (MRI), plain radiographs, and arthroscopic images. Patients were considered not suitable if they had inflammatory arthritis or evidence of advanced joint arthrosis in compartments distinct from the recipient compartment.
Each patient was assessed and treated according to the joint restoration philosophy of the senior author (T.S. ), where the ideal compartmental environment is created for the MAT. 8,22 Limb alignment was assessed clinically and supplemented with weightbearing, long-leg alignment radiographs. Neutral alignment was defined on long-leg films as the hip to ankle weightbearing axis falling within 10% of the midplateau point. If malalignment was present, proximal tibial opening wedge or distal femoral closing wedge osteotomy was performed to correct the weightbearing mechanical axis. Knee stability was assessed clinically and radiologically, and when ligament insufficiency was present, a reconstructive procedure was performed. Chondral lesions were treated with debridement, microfracture, or autologous chondrocyte implantation (ACI) using the matrix-induced autologous chondrocyte implantation (MACI; Genzyme) technique, depending on the lesion size and location. Debridement was selected for small lesions (<10-mm diameter) on the tibial surface that would be covered by the new meniscal graft or for lesions that were not well shouldered by healthy articular cartilage to support new cell growth. Chondral defects <4 cm2 in size were generally treated with microfracture, and larger defects were treated with the MACI technique. The above procedures were performed simultaneously in addition to the MAT when indicated.
The cohort was divided into 3 groups according to the International Cartilage Repair Society (ICRS) chondral grade of the affected compartment
11
: Group 1: up to ICRS grade 3a (partial-thickness) chondral damage on 1 or both condylar surfaces. Group 2: ICRS grade 3b (full-thickness) ± associated subchondral bone loss on 1 condyle, with the opposite articular surface having intact articular cartilage up to ICRS grade 3a. Group 3: ICRS grade 3b (full-thickness) ± associated subchondral bone loss to both the femoral condyle and tibial plateau surfaces.
Surgical Technique
All procedures were performed utilizing a minimally invasive arthroscopic technique with soft tissue fixation through bone tunnels. The technique has previously been described in detail by Spalding et al. 17 Menisci were sized according to radiographic measurements, and nonirradiated fresh frozen allografts were obtained from 1 of 3 tissue banks: NHSBT UK, RTI, and JRF Ortho. After preparation of the meniscal rim, 4.2-mm drill holes were created from the anterolateral or anteromedial tibial surface, emerging in the anatomic insertion sites of the meniscal roots. Lead sutures were passed and the transplant graft fed into the knee, tying the posterior and anterior horn sutures over a bone bridge on the tibia. Peripheral meniscal fixation was achieved using a combination of fixation devices (FastFix; Smith & Nephew) and inside-out sutures (2-0 Ticron; Covidien) tied over the capsule.
Rehabilitation
Patients are treated with a personalized, goal-orientated physiotherapy program. The first 6 weeks of rehabilitation consisted of touch weightbearing to minimize the traction forces on the meniscal root anchor points. Early range of motion from 0° to 90° and active static quadriceps exercises were commenced with avoidance of open chain quadriceps exercises during this initial period. From 6 weeks, weightbearing, strengthening, and proprioceptive rehabilitation were progressed once the patient achieved the required goals. From 6 months, a functional and sport-specific rehabilitation program was undertaken, with a return to intended activities from approximately 9 months.
Outcomes
Failure was defined as complete removal of the allograft, revision, or conversion to joint replacement. Knee injury and Osteoarthritis Outcome Score 13 (KOOS) and International Knee Documentation Committee 6 (IKDC) scores were recorded at baseline and then on a yearly basis. The research team collected all the patient-reported outcome scores independently of the operating surgeon. Loss to follow-up was defined as failure to obtain scores despite repeated attempts and searching to make contact at any time point during the follow-up period.
Statistical Analysis
Analysis was performed using the SPSS statistical package (IBM Corp). Descriptive statistics were used to analyze the baselines demographics of the series. A Cox proportional hazards model was performed to analyze for the effect on outcome of each potential predictor variable independently of others. Potential predictor variables were chosen from data that had been prospectively recorded if it was considered scientifically plausible that it could affect failure rate or had previously been shown to affect failure rate in other studies; adding in too many variables with little chance of being predictive can dilute other potentially predictive variables. The variables included were the following: cartilage grade at the time of MAT, IKDC score, lateral or medial allografts, sex, additional procedures, and tissue bank source. The proportional hazards assumption was tested by examining log-log plots. Kaplan-Meier survival curves were used for whole group survival and also significant predictors of failure, as determined by the Cox proportional hazards model. The log-rank test was used to determine whether differences in Kaplan-Meier survival curves were statistically significant.
Results
There were 125 patients included in the study. One patient was lost to follow-up, leaving 124 patients available for survival analysis. The baseline demographics of the 3 groups according to cartilage grade are presented in Table 1 and associated cartilage procedures in Table 2. The median follow-up time was 3 years (range, 1-10 years). The mean age in this series was 31 years (range, 8-49 years). The mean age at the time of initial meniscal injury/meniscectomy was 23.6 years, and the mean time to MAT was 6 years (range, 6 months to 30 years).
Baseline Demographics Overall and for Each Group a
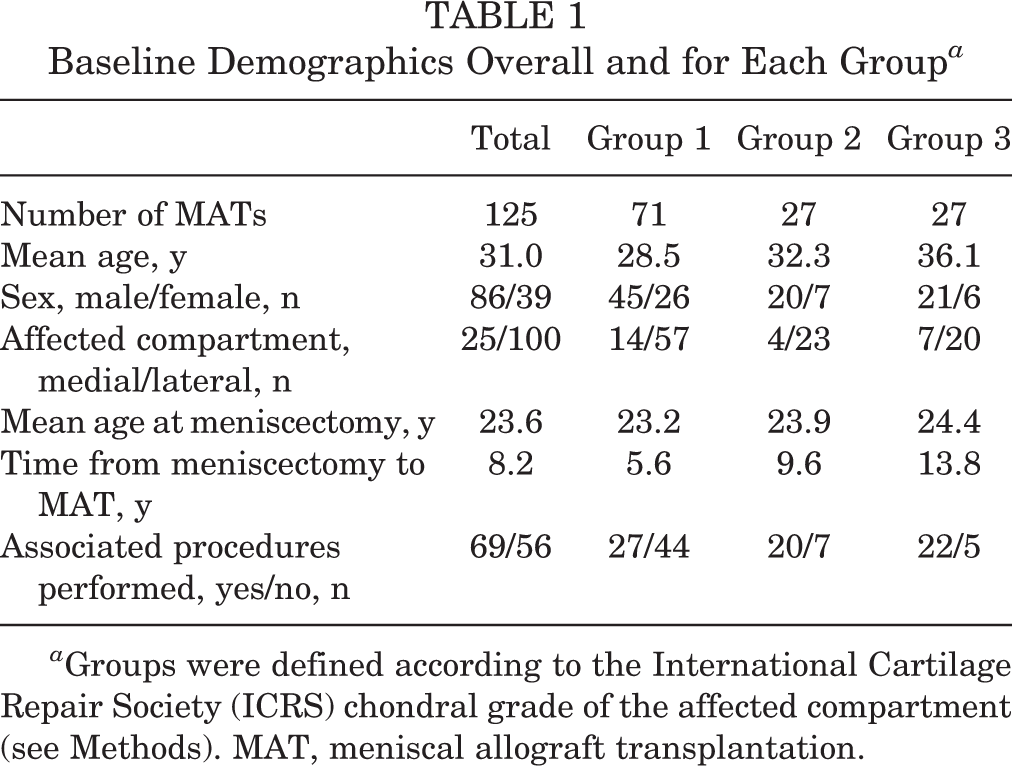
a Groups were defined according to the International Cartilage Repair Society (ICRS) chondral grade of the affected compartment (see Methods). MAT, meniscal allograft transplantation.
Cartilage Procedures Performed at the Time of MAT a
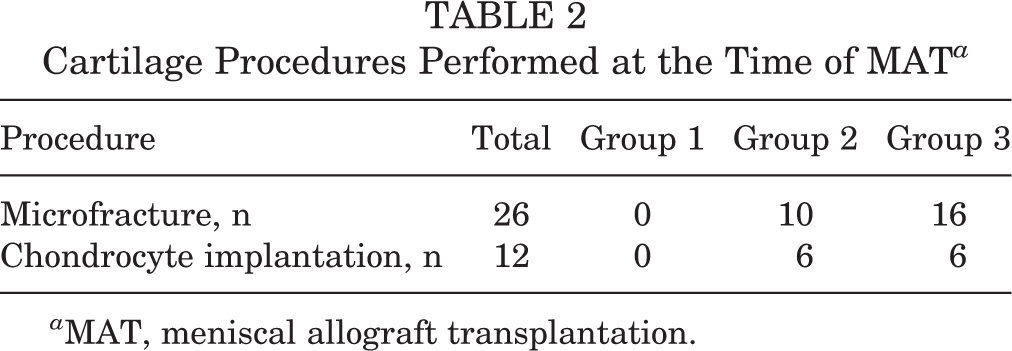
a MAT, meniscal allograft transplantation.
The results of the Cox regression model are shown in Table 3. After correcting for other predictor variables, cartilage grade and whether the allograft was medial or lateral were statistically significant predictors of survival. When comparing individual groups, the probability of failure in group 1 was 85% lower than for group 3 at any given time (95% CI, 13%-97%). There was a lower failure rate in patients that had lateral allografts, with a 76% lower probability of failure (95% CI, 16%-89%).
Cox Regression Analysis of Potential Predictor Variables a

a IKDC, International Knee Documentation Committee; MAT, meniscal allograft transplantation; NA, not applicable.
The Kaplan-Meier allograft survival curve of the whole cohort is shown in Figure 1, with a 5-year survival of 82%. The Kaplan-Meier allograft survival curve according to cartilage group is shown in Figure 2. Results show a 5-year survival of 97%, 82%, and 62% in groups 1, 2, and 3, respectively, with the survival rate for group 1 compared with groups 2 and 3 reaching statistical significance (P = .003, log-rank test). When comparing the overall number of failures between the groups, there were 2 of 70 (2.9%) in group 1, 3 of 27 (11.1%) in group 2, and 8 of 27 (29.6%) in group 3.

Overall cumulative meniscal allograft survival.

Kaplan-Meier curve according to group.
Figure 3 shows the Kaplan-Meier allograft survival curve grouped by medial or lateral allografts. The 5-year survival was 89% and 62% in the lateral and medial groups, respectively (P = .026, log-rank test). When comparing the overall number of failures between groups, there were 7 of 92 (7.6%) in the lateral and 6 of 19 (31.6%) in the medial group.

Kaplan-Meier curve according to medial or lateral allograft.
Discussion
This study has demonstrated that having a full-thickness cartilage lesion at the time of MAT is a significant predictor of failure, despite attempts to improve the biomechanical environment of the knee. Additionally, lateral allografts were found to have a significantly greater survival rate in comparison with medial allografts.
In this study, the overall survival was 82% at 5 years. However, this result hides the fact that there are significant differences according to the cartilage grouping. In our earlier study, 8 advanced cartilage damage appeared to be associated with failure. In this study with longer follow-up, more patients, and more events, cartilage group is shown to be a strong predictor of failure, even when balancing for potential confounders. Furthermore, the failure rate in patients with advanced cartilage damage is progressively higher once both condylar surfaces are involved.
In this study, 43% of patients had a full-thickness chondral defect at presentation and severe functional limitations as previously reported in the literature. 8,14,16 It has traditionally been considered that MAT is not suitable for patients with significant cartilage loss, leaving these patients with very few viable treatment options. With more recent studies showing improved results, MAT is being performed in patients with advanced disease at some centers. Farr et al 4 performed combined ACI in combination with MAT and had a 14% failure rate at a greater than 2-year follow-up. Stone et al 18 reported on a large series of patients undergoing MAT in the presence of severe articular damage and demonstrated a 25% failure rate of the primary meniscal graft at a mean follow-up of 5.1 years. They did not find an association between articular cartilage damage severity on Cox regression modeling, but all patients in the study already had severe articular cartilage damage. Other case series report lower failure rates, although patient numbers are small. 1,15 This study has compared the results of MAT in this challenging patient group to the traditional “ideal” patient group with intact articular cartilage and found that the articular cartilage status was a significant predictor of failure. In the “ideal” group with intact/partial-thickness articular cartilage loss, the 5-year survival rate was 97%. Once there was full-thickness cartilage loss, the 5-year survival rate was significantly lower (82% 1 condyle involved, 62% both condyles involved). This finding is important as it will enable surgeons preoperatively to inform and carefully counsel patients of their individual risk of graft failure. Despite the greater failure rate, many of these patients with full-thickness chondral loss are accepting of this risk, given the lack of viable alternatives to relieve pain and restore function in their knee.
A greater failure rate among medial allografts has previously been reported but has not been shown to be an independent predictor of failure before. In a series of patients undergoing MAT by van Arkel and de Boer, 20 7 of 17 medial allografts failed compared with 5 of 34 lateral allografts. These authors also reported that the mean survival time for medial allografts was 69 months and lateral allografts was 111 months. In another study, 8 of 46 medial allografts failed compared with 1 of 22 lateral allografts. 19 A further study performed a survival analysis of 100 MAT procedures, finding that the 14.5-year survival for medial allografts was 53% compared with lateral allograft survival of 70%. 21 When looking at isolated MAT procedures, the difference in survival was even greater, with a 27% survival at 13.4 years for medial allografts compared with 67% survival at 14 years for lateral allografts. 21 Additionally, Cole et al 2 were able to demonstrate a trend toward greater functional improvements in nearly all outcome scores with lateral meniscal grafts. It is not clear why medial allografts have poorer outcomes, but the differences in anatomy between the medial and lateral side have been proposed as a possible cause. 20 Further investigation would be warranted to determine whether the failure rate in medial allografts could be reduced.
Limitations
One of the difficulties in comparing failure rates across studies is that failure is variably defined in the literature. 14,22 While complete allograft removal or conversion to joint replacement is a clear and hard failure definition, it does not directly take the patient’s symptoms into account. Some authors suggest defining failure if patient-reported outcomes fall below a certain level. This would be likely to increase the reported failure rate of a series, but would have difficulties: which measure would be used, would it take the patients preoperative state into account, would an equal preoperative and 10-year postoperative score be considered a failure given the likelihood of some osteoarthritis progression in between? Cox regression balances for known (and measured) confounders; however, it cannot balance for unknown confounders, which may have had an influence on the results. Only a randomized controlled trial can balance such unknown confounders.
This study was designed to determine factors predictive of failure. It did not address functional or radiographic outcomes, which are important from the patient’s perspective. Therefore, while certain factors are shown to predict failure, it does not necessarily follow that patients in these groups have poor functional outcomes.
Conclusion
This study has demonstrated that the presence of severe articular cartilage damage at the time of MAT and medial allografts were significantly predictive of failure. Surgeons and patients should use this information when considering the risks and benefits of surgery.
Footnotes
The authors reported no conflicts of interest in the authorship and publication of this contribution.