
Abstract

The number of anterior cruciate ligament (ACL) injuries among young athletes has increased over the past 2 decades. It is currently estimated that 47 per 100,000 boys aged 10 to 19 years will require surgery for an ACL injury each year. 12 Apart from the immediate debilitating effects, there are serious long-term consequences of ACL injuries, including chronic knee instability, cartilage damage, and osteoarthritis—all leading to decreased activity levels. On average, 50% of individuals will develop radiographic signs of osteoarthritis, which is associated with pain and functional impairment, 10 to 20 years after diagnosis. 14 Thus, it is imperative to identify young athletes that may be susceptible to ACL injuries and implement preventative training measures in these individuals. The incidence rate of ACL injuries among young, male, American football players has been reported to be 0.58 ACL injuries per 10,000 athlete-exposures, with an athlete-exposure being defined as 1 athlete participating in either 1 game or 1 practice. 23
We report a case study of 4 consecutive brothers all requiring surgical treatment for football-related ACL injuries before the age of 22 years. The probability of such injuries occurring to the first 4 brothers in any given family by chance would be approximately 1 in 36 million given the reported incidence rate and an estimated 100 exposures per year for competitive players and 10 exposures per year for players playing leisurely. Given the uniqueness of such a case, we evaluated the brothers and the specifics to their injuries. We hypothesize that these brothers may have familial risk factors such as an increased posterior tibial slope, a narrow intercondylar notch width, or a high body mass index (BMI) underlying this apparent predisposition to ACL injury.
Case Report
Brother 1
The patient reported a knee injury after playing recreational football with his brother in December 2011. The patient was 21 years old when the injury occurred, and he reported experiencing a lateral blow or valgus force applied to his left knee, causing it to give way. After the injury and a period of activity, rest, and physical therapy, the patient continued to experience multiple episodes of instability despite bracing. At the time of orthopaedic consultation (approximately 1 year after initial injury), the patient had a height of 177.5 cm and a weight of 107.4 kg, with a resultant BMI of 34.1 kg/m2. On physical examination, the patient had full range of motion, no effusion, and a negative anterior drawer test but a positive Lachman test. The pivot shift was negative due to patient guarding, and no findings consistent with generalized ligament laxity were noted. Preoperative imaging revealed no significant anatomic abnormalities (Table 1). Magnetic resonance imaging (MRI) revealed a complete ACL tear with a concomitant medial meniscus tear. After the appropriate treatment options and their associated risks, benefits, and impact on future sports activities were communicated, the patient elected for ACL reconstruction using hamstring tendon autograft and had an uneventful postoperative recovery and rehabilitation was last assessed 3 months after the surgery.
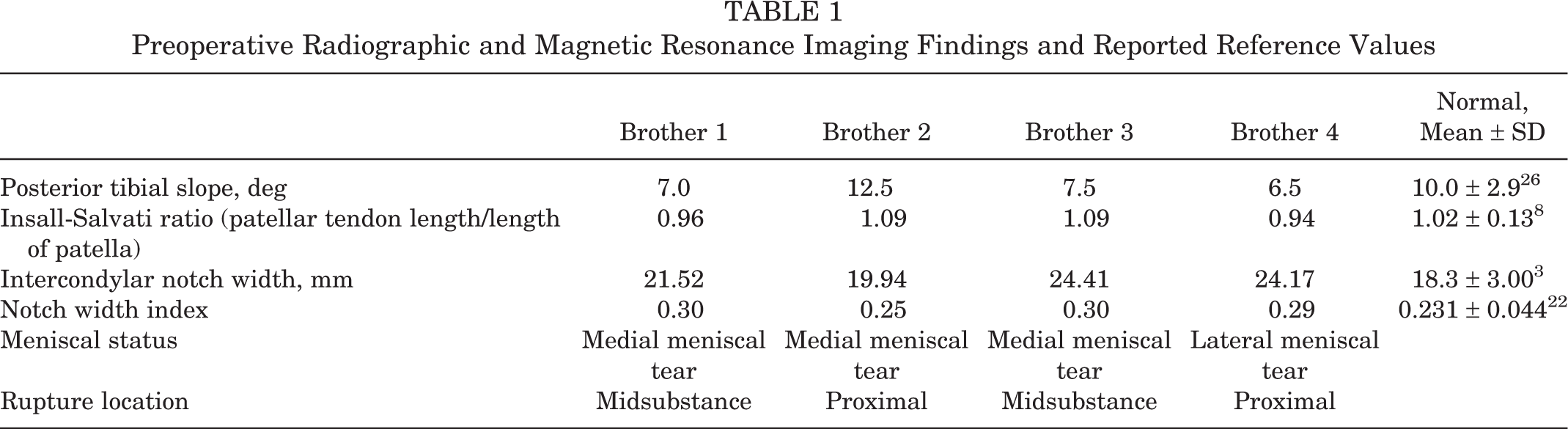
Preoperative Radiographic and Magnetic Resonance Imaging Findings and Reported Reference Values
Brother 2
The patient reported a right knee injury after pivoting and changing directions during football in July 2012. The patient was 18 years old at the time and was diagnosed with an ACL rupture. He was able to complete the remainder of his football season using an ACL-stabilizing brace. At orthopaedic consultation in November 2012, the patient’s height of 177.8 cm and weight of 103.6 kg yielded a BMI of 32.8 kg/m2. On physical examination, the patient had full range of motion and no effusion but medial joint line pain on palpation and a positive Lachman test. The patient deferred pivot testing due to apprehension, and all other tests were negative including no generalized ligament laxity. No obvious anatomic abnormalities were appreciable based on preoperative imaging results (Table 1). MRI demonstrated a full-thickness ACL rupture, a posterior horn medial meniscal tear, and a small focal medial femoral condyle cartilage defect. The patient opted for ACL reconstruction with hamstring autograft after the appropriate risks and benefits and expected return to play of the conservative and operative management pathways were discussed. Microfracture was performed on the medial femoral condyle, which had a 2 × 3–cm defect. A partial posterior horn medial meniscectomy was performed. Postoperative recovery was unremarkable, as was subsequent follow-up at 26 months after surgery.
Brother 3
The patient reported a right knee injury after pivoting while playing football during the summer of 2010. The patient was 15 years old when this initial injury occurred, and he reported an audible “pop” during the injury and almost immediate knee effusion. The patient experienced subsequent injuries to the knee and had been unable to play sports comfortably. He suspected an ACL tear and also used an ACL brace for activity and completed a trial of physical therapy. At orthopaedic consultation in March 2012, the patient’s height of 172 cm and weight of 91.5 kg yielded a BMI of 30.9 kg/m2. On physical examination, the patient had full range of motion and no effusion, but he had positive Lachman and pivot shift tests. There were no findings consistent with generalized ligament laxity. Preoperative imaging results, displayed in Table 1, indicated no obvious anatomic abnormalities and he was skeletally mature. The MRI identified a full-thickness ACL tear and a medial meniscus tear. Again, this patient opted for ACL reconstruction using hamstring autograft after the conservative and operative management pathways were discussed. Unlike the previous patient, his meniscal tear was amenable to repair with the all-inside suture technique. He completed rehabilitation uneventfully and returned to sport 1 year after index surgery. However, the patient experienced an injury to the same knee while playing football 14 months after index surgery. At 15 months postoperatively, an MRI scan revealed an intact ACL graft and degenerative tearing of the medial meniscus involving the body and posterior horn. This was addressed with arthroscopic partial meniscectomy 2 months later.
Brother 4
The patient reported a left knee injury after a hyperextension injury while playing football in November 2014. The patient was 15 years old when the injury occurred. He reported an audible “pop” during the injury, with a slowly developing, delayed effusion. There was some subjectively instability, but weightbearing was unaffected and he had progressed appropriately with physical therapy. At orthopaedic consultation 2 months later, the patient’s height of 186.4 cm and weight of 117 kg resulted in a BMI of 34.5 kg/m2. On physical examination, the patient lacked 5° of full extension in the knee and had full flexion, and he had a positive Lachman test and negative pivot-shift test. All other tests were normal, and there were no findings consistent with generalized ligament laxity. Preoperative imaging results indicated no substantial anatomic abnormalities and skeletal maturity (Table 1). MRI revealed an ACL tear with partial reattachment to the posterior cruciate ligament as well as a complex lateral meniscus tear (Figure 1). Bone contusions were noted on the lateral femoral condyle and lateral tibial plateau. Informed consent was obtained for ACL reconstruction using hamstring tendon autograft, as was the situation with his brothers. On follow-up 2 months postoperatively, recovery was unremarkable.

Sagittal magnetic resonance image of the knee for brother 4 indicating a complete anterior cruciate ligament rupture.
Discussion
Several studies have identified that males who have a first-degree relative with an ACL injury have a familial predisposition for an ACL injury themselves. 4,16 This report demonstrates a case of 4 brothers all requiring surgical intervention for complete ACL ruptures. Two of the brothers had midsubstance ruptures of their ACL while the other 2 brothers had proximal ruptures. The specific mechanism of each injury may have contributed to the particular locations of the tears. Brothers 1 (valgus force) and 3 (pivoting) likely experienced a transection of the ACL by the lateral femoral condyle causing a midsubstance tear. On the other hand, brother 4 was injured with an alternate mechanism of hyperextension, which may have resulted in a proximal ACL tear. 28 Although there was initially an episode of pivoting that lead to pain in brother 2, the exact mechanism of the proximal tear is not clear as the history suggests this patient likely experienced multiple injuries. An alphanumeric classification system for intra-articular ACL ruptures has been established by Zantop and Petersen 28 based on the specific bundle that is injured as well as the location and severity of the tear. Rupture of the anteromedial bundle is given a number from 1 to 5, while tears involving the posterolateral bundle are assigned a letter from A to E (1 and A, proximal rupture; 2 and B, midsubstance rupture; 3 and C, tibial rupture; 4 and D, insufficient or elongated bundle; and 5 and E, intact bundle). Because of the retrospective nature of this study, we were unable to delineate the individual bundle tear patterns for the brothers based on the MRIs available. 28 In addition to the ACL ruptures, each of the brothers had concomitant lateral or medial meniscal tears. Furthermore, all the injuries occurred while playing American football between the ages of 15 and 21 years, whether competitively or leisurely. While young American football players may play a variety of positions, all 4 brothers particularly played positions that require acceleration, deceleration, and pivoting during games, such as running back and full back. Bradley et al 2 found no significant association between the position played and the type or frequency of the injury in a study of 322 elite collegiate football players.
This case series is especially interesting considering that ACL injuries occur up to 4 times more often in 14- to 19-year-old female athletes than in male athletes of the same age participating in the same sport. 18 Individuals who have sustained ACL injuries have been shown to possess risk factors for the injury such as increased general joint laxity, increased patellar tendon length, increased knee abduction angles, and decreased knee flexion angles. 7 The results of the preoperative physical examinations and imaging reviewed in this study indicate that none of these factors were abnormal in all 4 brothers. Two specific anatomic risk factors that could have been likely to contribute to a familial predisposition to ACL injury in these brothers involve the intercondylar notch width (NW) and tibial slope. 5,11 The NW is determined using anteroposterior imaging and represents the width of the intercondylar fossa of the femur measured at the level of the popliteal groove. The notch width index (NWI) represents the ratio of the previously described NW to the entire femoral condyle, measured at the same level. 11 The posterior tibial slope is determined using lateral imaging and identifies the angle between a line tangential to the medial tibial plateau and the proximal anatomic axis of the tibia. 27 The depth of concavity of the medial tibial plateau (MTD) can be measured in the same plane as the tibial slope and indicates the distance between a line connecting the superior and inferior iliac crests and the lowest point of the concavity. 6 Siblings with a history of ACL injuries have been shown to have a narrow NW and NWI in addition to an increased tibial slope. 5,11 Males with increased tibial slopes in combination with a decreased MTD are at increased risk for an ACL injury. 6 However, 3 of the 4 brothers in this study had a decreased tibial slope, and all 4 brothers had a NW and NWI greater than the mean values identified in literature. Thus, according to the data available, anatomic risk factors did not contribute to the familial predisposition to ACL injury.
The height (cm) and weight (kg) of each brother was normalized by calculating their BMI using the following formula: BMI = weight (in kilograms)/height (in meters) squared. Using the Centers for Disease Control and Prevention growth charts and new BMI-for-age charts, the percentiles and z-scores (the number of standard deviations the value deviates from mean) were determined for each brother. Brother 1 had a BMI of 34.1 kg/m2 on consultation, corresponding to the 98th percentile with a z-score of 2.08. Brother 2 had a BMI of 32.8 kg/m2 on consultation, corresponding to the 98th percentile with a z-score of 2.14. Brother 3 had a BMI of 30.9 kg/m2 on consultation, corresponding to the 98th percentile with a z-score of 2.07. Brother 4 had a BMI of 34.5 kg/m2 at the time of injury, corresponding to the 99th percentile with a z-score of 2.35. Each of the brothers had a BMI more than 2 standard deviations (SDs) greater than the mean and all higher than the 98th percentile for their age and sex. 15,19
A literature search identified 2 studies that have evaluated the relationship between BMI and the occurrence of ACL injuries. Evans et al 3 reported that a high BMI may be an independent risk factor for noncontact ACL injuries in young male athletes in a study of 1434 male military subjects between the ages of 17 and 19 years. The article found that the relative risk of a noncontact ACL injury associated with a BMI of 1 SD or greater than the mean was 3.2. Having a high BMI was not reported to be an independent risk factor for noncontact ACL injuries in females among the 253 subjects studied. 3 On the other hand, Uhorchak et al 25 reported that a high BMI may be an independent risk factor for young female athletes. The relative risk ratio associated with having a BMI of 1 SD or greater than the mean was 3.5 among 118 young female cadets. No significant association was found among the 729 male subjects studied. 25
The present study suggests that a BMI 2 SD greater than the mean may be a risk factor for ACL injuries in young male athletes. This represents a very unique cohort of patients, as studies show that individuals with a very high BMI typically have a low fitness level. 10 However, the patients in the present study had a BMI higher than the 98th percentile for their age and sex, but they were athletes with a high level of activity. Furthermore, these brothers had played positions requiring cutting and pivoting such as running back which, coupled with a very high BMI, may have increased their risk for an ACL injury.
Although environmental factors play a major role in determining BMI, there is also a genetic component associated with BMI, and various loci affecting metabolic phenotypes have been identified. 13 Other genetic factors could be underlying the familial predisposition to ACL injuries by altering the composition of the ligament itself. The collagen type I alpha 1 (COL1A1), type V alpha 1 (COL5A1), and type XII alpha 1 (COL12A1) genes code for protein chains that are found in tendons and ligaments and regulate strength as well as fibril diameter. 21 Several genes responsible for producing molecular components of the ACL extracellular matrix include aggrecan (ACAN), fibromodulin (FMOD), and WNT1-inducible-signaling pathway protein 2 (WISP2). 9 Specific genotype variants in each of these genes have been associated with increased risk of ACL injuries. 9,21 Furthermore, 2 genotypes of the vascular endothelial growth factor A (VEGFA) and kinase insert domain receptor (KDR) genes, genes involved in angiogenesis-associated signaling cascade, have been associated with ACL injury. It is thought that, in response to loading, angiogenesis-associated signaling is a major component of extracellular matrix remodeling, which could affect the strength of the ACL. 17 Although, formal genetic testing was not conducted, the brothers belong to an Asian ethnic group and have no family history of ligamentous laxity, hypermobility syndromes, or connective tissue disorders.
Future research should evaluate a larger sample size for the risk of an ACL injury among young athletes with a BMI of 2 SD or more above the mean, particularly those participating in actions such as pivoting and cutting. Furthermore, these subjects should be evaluated for other genetic and anatomic risk factors that may, in combination with a very high BMI, increase the likelihood of an ACL injury. Identifying subjects with such risk factors could be very important for the cohort of athletic young males with a BMI greater than the 98th percentile playing sports such as American football. Susceptible athletes could participate in various prevention programs including education, training, and prophylactic bracing that may decrease the probability of ACL injuries in the future. 24 However, while some data exist demonstrating efficacy of prophylactic bracing in sports such as alpine skiing and motocross, prophylactic bracing has not yet demonstrated effectiveness in preventing ACL injuries in football players. 1,20
Conclusion
This case series of 4 consecutive brothers all with American football–related ACL injuries and concomitant meniscal tears requiring surgical intervention may contribute to evidence of a familial predisposition to ACL injuries. Common anatomic risk factors such as increased posterior tibial slope, narrow intercondylar notch width, and general ligament laxity were not appreciated on preoperative imaging and physical examinations of the brothers. However, all brothers had a BMI greater than the 98th percentile for their age and sex. Thus, having a BMI greater than 2 SD above the mean may be an independent risk factor for ACL injuries in young, male athletes, particularly those who play positions requiring pivoting and cutting motions such as running back, and should be investigated further.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.