
Abstract
Anatomic reconstruction of the anterior cruciate ligament (ACL) has been shown to improve stability of the knee, particularly rotational stability, potentially leading to superior clinical outcomes and a shorter return to sport. Nonanatomic ACL reconstruction has been linked to graft failure and abnormal cartilage loading thought to contribute to progression of degenerative joint disease. Use of the far anteromedial portal (FAMP) to uncouple the tibial and femoral tunnels has led to improved reproduction of the femoral footprint and facilitates drilling of the femoral tunnel in an anatomic position. The use of the FAMP and straight reamer systems introduces its own set of potential complications, including short femoral tunnels and peroneal nerve injury. These potential complications have been addressed by drilling the femoral tunnel in a hyperflexed position, which can lead to difficulty with positioning the operative extremity, visualization, and identification of anatomic landmarks. The purpose of this case report was to review the advantages and technical aspects of using a flexible reamer system and the FAMP to achieve an anatomic ACL reconstruction while avoiding potential complications and pitfalls. Flexible reamer systems allow an additional way of uncoupling the tibial and femoral tunnels to clearly visualize and establish an anatomic starting point within the femoral footprint of the native ACL while avoiding the complications associated with knee hyperflexion and straight reamers with the far anteromedial portal. In the authors’ experience, an anatomic reconstruction of the ACL can be achieved safely using flexible reamers while avoiding some of the difficulties seen with straight reamers used in conjunction with an uncoupled, far anteromedial approach.
Increasing evidence suggests that anatomic reconstruction of the anterior cruciate ligament (ACL) leads to improved knee stability, particularly anterior translation of the tibia and rotational stability (pivot shift). 1,4,5,13,18 The thought that improvement in knee kinematics directly leads to improved clinical outcomes remains controversial, as several reports comparing anatomic ACL reconstructions to nonanatomic ACL reconstructions have found no significant difference in outcome measures, 2,9,10 while other comparative studies have demonstrated earlier return to activity and sport as well as superior subjective outcome scores. 2,6,12,16 It has also been reported that nonanatomic ACL reconstructions may fail to restore normal knee kinematics, leading to increased forces on the articular cartilage and contributing to accelerated progression of degenerative joint disease and graft failure. 3,5,12,17,20 Much of this information has been gained from decades-long study of femoral tunnel placement of the ACL beginning with outside-in, transtibial endoscopic, and double-bundle femoral tunnel placement and combined with outcome data showing functional stability is considered critical for a successful reconstruction of the ACL. The anatomic understanding of the origin of the ACL on the lateral wall of the femoral notch is critical to be relatively lower than what was traditionally accepted in early reconstructions, especially those seen when using a transtibial approach and more “vertical” appearing ACL graft placement. Last, the understanding of the ACL femoral anatomic footprint below the intracondylar ridge and with the bifurcate ridge splitting the anteromedial (AM) and posterolateral (PL) femoral bundles is an important landmark. In contrast to previous notchplasties used to increase visualization of the femoral origin of the ACL, the bifurcate ridge is now preserved for a more accurate placement of the single-bundle femoral tunnel.
Given the importance of anatomic tunnel position on ACL outcomes, the available intraoperative landmarks used to guide correct femoral tunnel placement have been discussed extensively in recent literature. 7,8 Advancements in arthroscopic instrumentation and use of the far anteromedial portal (FAMP) to uncouple the tibial and femoral tunnels has led to an improved ability to drill the ACL femoral tunnel within the native ACL footprint, providing an anatomic reconstruction. 14 However, drilling the ACL femoral tunnel through the FAMP with a straight reamer and the knee in 90° of flexion can result in complications, such as posterior condylar blowout, a short femoral tunnel length, and injury to the peroneal nerve if the guide wire happens to exit below the long head of the biceps femoris. When using a straight guide wire and reamers from the FAMP position, the surgeon must hyperflex the knee to avoid the above complications. Hyperflexion of the knee often decreases flow significantly (even with the use of a pump) at this critical juncture in the procedure, and visualization in the notch is often compromised. 11 Finally, viewing the lateral wall of the notch with the knee in hyperflexion results in a change in the appearance and location of the ACL femoral attachment site compared with the appearance obtained when the knee is positioned at 90° of flexion. This can result in spatial disorientation, which may lead to malposition of the ACL femoral tunnel.
In this case report, we discuss the use of the FAMP, a 30° arthroscope, and flexible guide wire/reamer systems (Clancy Anatomic Cruciate Guide Flexible Drill System; Smith & Nephew or VersiTomic Flexible Reaming System; Stryker). We discuss the advantages of a flexible reaming system and recommendations to help avoid the potential complications seen in recent reports of flexible guide wire and reamer breakage. In our experience, anatomic reconstruction of the ACL can be achieved safely using flexible reamers while avoiding some of the difficulties seen with straight reamers used in conjunction with an uncoupled, FAMP approach.
Surgical Technique
The patient undergoes induction of general anesthesia, and prophylactic antibiotics are administered. An examination under anesthesia is performed. A clean/sterile tourniquet is then placed proximally on the thigh. The patient is positioned in the supine position with a lateral thigh post or isolated leg holder to achieve valgus stress as needed. Standard institution-based time-out is taken verifying patient identification, laterality, and appropriate equipment/indicators with the entire surgical team present. The extremity is prepped and draped in a sterile routine fashion. The lower extremity is exsanguinated with an Esmarch bandage and the tourniquet inflated to an appropriate level with the knee flexed to 120°. Examination under anesthesia is performed; if this examination correlates with preoperative imaging, the autograft is harvested prior to diagnostic arthroscopy. Both bone–patellar tendon–bone and hamstring grafts can be utilized with a flexible reamer technique without difficulty. After harvest, the autograft is prepared on the back table in standard fashion. For bone–patellar tendon–bone autografts, a shorter femoral bone block is created to ensure that there is room for the bone block to rotate in the notch and pass into the ACL femoral tunnel. We recommend a bone plug no longer than 23 mm and prefer a 20-mm bone plug, which allows for unrestricted graft passage while providing sufficient bone for secure fixation with an interference screw.
Femoral Tunnel Changes and Graft Demands With an FAMP Approach
We first establish a superomedial outflow portal in the suprapatellar pouch. Next, a standard anterolateral portal is established and the arthroscope is inserted. A diagnostic arthroscopy of the knee joint is performed using a 30° arthroscope. A standard medial parapatellar portal is created under direct visualization using a spinal needle. Instrumentation is introduced through this portal for addressing associated intra-articular pathology, and this portal is also used to view the lateral wall of the intercondylar notch during preparation and drilling of the ACL femoral tunnel. This procedure can easily be performed using a 30° arthroscope viewing from a tight anteromedial portal but has also been described using a 70° arthroscope viewing from the anterolateral portal to avoid the “sword fighting phenomenon” described by Rasmussen et al 15 as a result of 2 medial portals. Once meniscal and chondral pathologies have been treated, attention is turned to the technical aspects of the ACL reconstruction.
The remnant of the ACL is debrided using a straight arthroscopic basket punch and motorized shaver blade, separating the scarred ACL from the intact posterior cruciate ligament (PCL). Care is taken to adequately debride soft tissue from the lateral wall of the notch for clear visualization of the anatomic landmarks while not disrupting or altering the bony anatomy of the lateral femoral condyle. The motorized shaver blade is then used through the anteromedial and anterolateral portals to debride the tibial footprint, leaving minimal residual ACL tissue. If the tibial remnant is not sufficiently debrided, it may deflect the curved endoscopic passing guide, thus altering the 45° angle uniquely achieved by using a flexible guide pin without hyperflexing the knee. This 45° angle relative to the tibial plateau is essential in avoiding a short femoral tunnel and potential injury to the common peroneal nerve and lateral supporting structures. The anterior and posterior boundaries of the tibial footprint are identified, and the center is marked with electrocautery. The center point is marked just lateral to the medial tibial eminence. A spinal needle is then used to establish the far anteromedial portal, placed just superior to the anterior horn of the medial meniscus with the needle hugging the medial femoral condyle and PCL. The needle should safely skirt the medial femoral condyle and PCL on route to the anatomic footprint of the ACL on the medial aspect of the lateral femoral condyle (Figure 1).

Position of the far anteromedial portal. Spinal needle entering just superior to the anterior horn of the medial meniscus and passing just anterior to the medial femoral condyle.
With the knee in 90° of flexion and viewing with a 30° arthroscope via the tight anteromedial portal, the ACL footprint is examined and the posterior wall is clearly identified by placing a probe in the over-the-top position. Next, a point within the anteromedial bundle footprint, inferior to the lateral intercondylar ridge and slightly deep to the bifurcate ridge, is identified and clearly marked with electrocautery, microfracture awl, or a curved curette (Figure 2). The knee is then flexed to 110°, and the curved endoscopic offset guide (Figure 3) is passed through the FAMP to the previously chosen entry point (Figure 4). The nitinol guide wire is positioned at the previously marked ACL femoral tunnel location (Figure 5) and drilled through the skin of the lateral thigh. The guide wire should exit at an anterolateral position, well anterior to the common peroneal nerve, as demonstrated in Figure 6. A straight lateral exit point indicates a horizontal and possibly short tunnel, and a straight anterior exit point indicates a vertical tunnel position. The guide wire tip should stop approximately 2 to 3 cm from the lateral skin exit point; this leaves approximately 8 cm of guide wire out the FAMP (Figure 6). This positioning keeps adequate nitinol wire medially to avoid kinking and breakage of the flexible reamers, especially the smaller 4.5-mm flexible reamer. At this point, the knee must be held in this 110° flexed position to avoid nitinol guide wire kinking. It is important to understand knee flexion of 110° maximizes femoral tunnel length and minimizes risk of posterior wall blowout as well as injury to the common peroneal nerve. A lesser degree of flexion may result in an angle less than 45°, which creates a shorter and more horizontal tunnel, placing the posterior wall and peroneal nerve at greater risk. A greater degree of knee flexion is unnecessary and may lead to increased bend in the flexible guide wire, causing increased stress on the flexible reamer and possible breakage. Changing the degree of flexion from placement of the flexible guide wire to reaming may result in an acute bend in the guide wire, also causing increased resistance on the reamer leading to possible breakage.
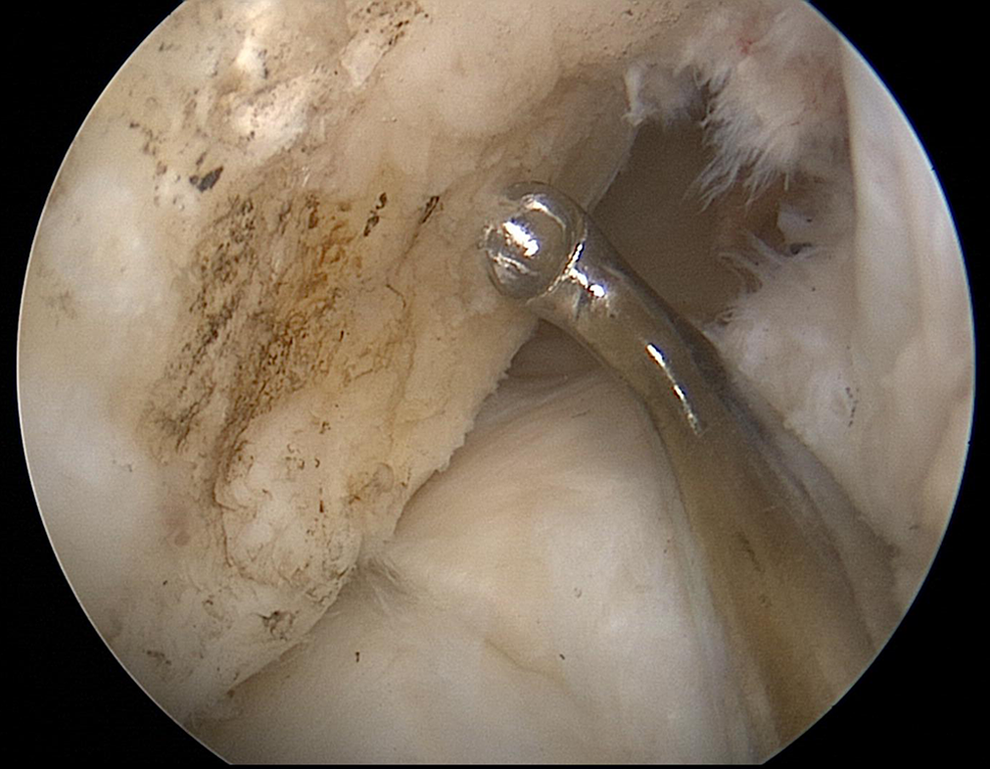
Bony anatomy of the lateral femoral condyle and anterior cruciate ligament femoral footprint demonstrated with a curved curette positioned within the anteromedial bundle footprint, just inferior to the lateral intercondylar ridge and slightly deep to the bifurcate ridge.

Offset guide, nitinol wire, and flexible reamer with eccentric cutting flutes (VersiTomic Flexible Reaming System; Stryker).

View obtained from the tight anteromedial parapatellar portal using a 30° arthroscope with knee flexed to 110°. The offset flexible reamer guide is passed safely by the medial femoral condyle under direct visualization.
The offset flexible reamer guide used to place the flexible guide wire at the chosen anatomic location of the femoral tunnel.

Knee flexed to 110° for the placement of the flexible guide wire and reaming of the femoral tunnel demonstrating the correct anterolateral exit trajectory of the flexible guide wire with the knee flexed to 110°. Approximately 2 to 3 cm of guide wire exiting the lateral thigh keeps adequate nitinol wire medially out the far anteromedial portal (FAMP) to avoid kinking and breakage of the flexible reamers.
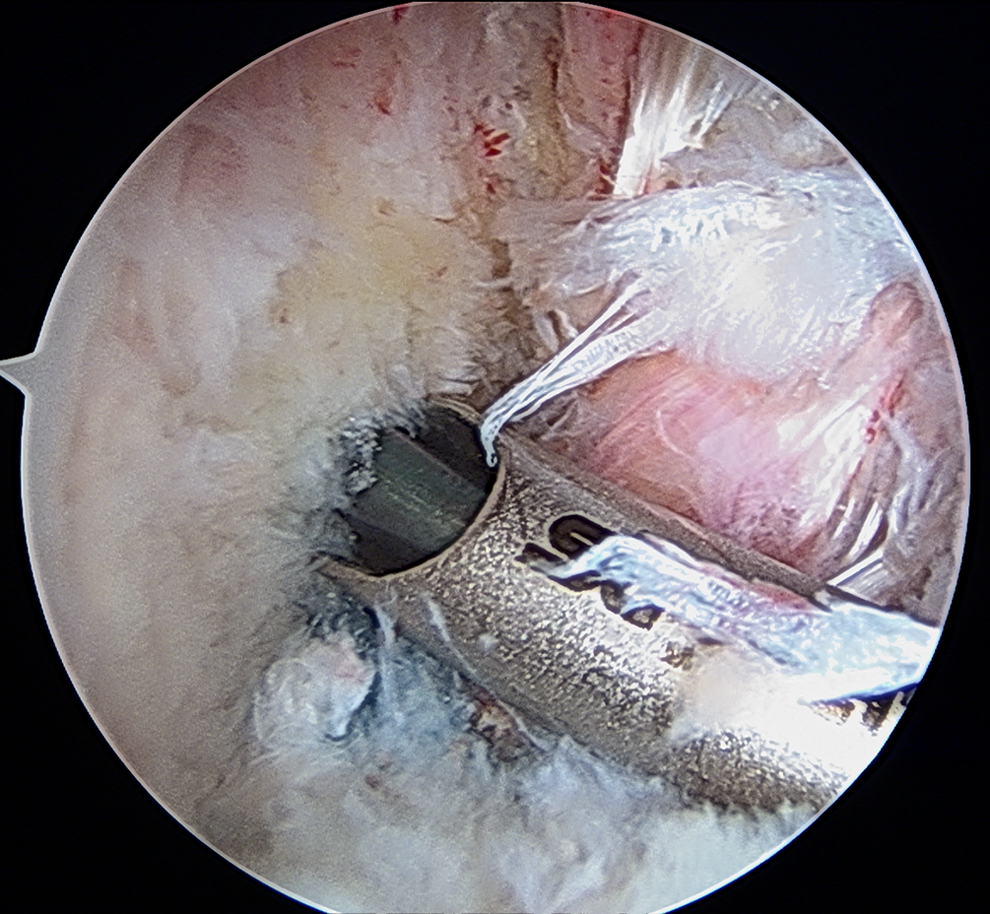
Based on the type of graft being utilized and the planned method of femoral-sided fixation, the appropriate size flexible reamer is then introduced over the flexible guide wire, taking care to avoid damage to the medial femoral condyle and advance to the desired tunnel depth. The surgeon must be aware of the guide wire’s proximity to the medial femoral condyle and take care to avoid damage to the articular cartilage when passing reamers over the guide wire from the far anteromedial portal. We prefer to use a reamer with eccentric flute heads; this allows for rotation of the cutting flutes away from the articular cartilage while passing the articular surface on way to the native ACL footprint. Reamer passage should be done with great care and under direct visualization to avoid iatrogenic damage to the articular surface (Figure 7). Using an initial 4.5-mm reamer is often advantageous as it allows for button fixation passage out over the lateral wall of the femur and for accurately measuring the femoral tunnel length. Using a 4.5-mm reamer also allows mobility of the nitinol guide wire and can position the final reamer slightly superior or more toward the PL bundle footprint; this is useful if the nitinol guide wire is initially positioned slightly inferior or too close to the AM bundle footprint. Flexible reamers are safe and straightforward to use and can accurately determine the depth of the ACL femoral socket. The femoral aperture is debrided of peripheral soft tissue, and the tunnel edges are smoothened with the shaver while the nitinol guide wire is still in place. The shaver is best placed through the FAMP when cleaning out the tunnel edges to allow for ease of access. The arthroscope can also be shifted to the far anteromedial portal to allow a clear look into the tunnel, evaluating the integrity of the posterior wall and far cortex (Figure 8). A passing suture is then passed via the flexible guide wire and the loop is parked behind the lateral femoral condyle to avoid damage during tibial tunnel preparation.

Arthroscopic view from the tight anteromedial parapatellar portal demonstrating passage of the eccentrically fluted (cutting flutes directed away from the articular surface) flexible reamer under direct visualization, taking care to avoid iatrogenic damage to the medial femoral condyle.

View down the femoral tunnel from the far anteromedial portal with a 30° arthroscope demonstrating an intact posterior wall and far cortex.
A rigid tibial guide pin is passed using the 55° tibial guide and reamed to the same diameter as the graft utilizing a soft tissue protector and a large curette to protect the lateral femoral condyle. The passing suture is then retrieved from behind the LFC via the FAMP and delivered to the mouth of the tibial tunnel and then retrieved out the tibial tunnel. The graft is then pulled into the notch through the tibial tunnel. With the sharper turning angle into the less vertical femoral tunnel using the FAMP approach, the graft can be difficult to pass into a lower wall tunnel. Using a probe in the notch just above the tibial tunnel, the passing suture can be lifted while pulling laterally to help the graft (especially when using a bone–patellar tendon–bone graft) turn and pass into the low femoral tunnel. The graft is secured with the surgeon’s choice of femoral fixation with either a lateral button or interference screw fixation. The graft is cycled, tensioned near full extension, and secured on the tibial side with the surgeon’s preferred method of fixation. The graft is probed and final images are obtained. The arthroscopic instrumentation is removed from the knee, and the incisions are closed in standard fashion.
Discussion
Flexible reamer systems allow for anatomic re-creation of the ACL femoral insertion without compromising optimal tunnel trajectory and avoiding the need for hyperflexion of the knee. We prefer to avoid hyperflexion for 2 key reasons. First, positioning the patient in a way that allows for hyperflexion becomes somewhat cumbersome, especially if their body mass index is higher and limbs are shorter. Second, hyperflexion past 110° when using straight reamers through the FAMP can create low arthroscopic flow and in turn significant obstruction of the visual field while drilling the femoral tunnel. With low flow, the surgeon is sometimes left guessing the depth of the ACL femoral socket and integrity of the back wall. Flexible reamer systems used through an FAMP can be used with the knee in 110° of flexion, allowing better visualization during drilling of the ACL femoral tunnel. It is critical to highlight that by keeping the knee flexion constant at 110° from placement of the flexible guide wire through the reaming process, we avoid introducing an acute bend in the guide wire and minimize the resistance on the flexible reamers, thus preventing reamer breakage. Knee flexion of 110° also allows for unrestricted placement of the curved endoscopic femoral guide in the center of the femoral foot print while maintaining a 45° superolateral trajectory, thus maximizing tunnel length, protecting the posterior wall, and minimizing risk to the common peroneal nerve. Recent studies have suggested that flexible guide wires used with the knee in 110° to 120° of flexion provide longer femoral tunnels with less risk of posterior cortex blowout and peroneal nerve injury when compared with rigid guide wires. In a series of 10 cadaveric knees position in 120° of flexion, Silver et al 19 reported longer and more consistent femoral tunnel lengths with flexible guide pins and reamers when compared with standard ridged reamer systems with an average tunnel length of 43.5 and 37.1 mm, respectively (P = .01). In terms of tunnel consistency, they reported 8 of 10 intraosseous distances were less than 40 mm with straight guide pins, and all but 1 distance was at least 40 mm long with flexible guide pins. With regard to peroneal nerve injury, they reported a trend toward a further exit point from the peroneal nerve with flexible guide pins compared with rigid guide pins (37.8 and 42.3 mm, respectively). 19 This difference was not significant (P = .33). They did, however, show an increased exit distance from the origin of the lateral collateral ligament: 13.4 mm with rigid guide pins and 26.1 mm with flexible guide pins. This difference was significant (P = .003). 19 In a series of 6 matched pairs of cadaveric knees, Steiner and Smart 21 reported flexible guide pins placed by anteromedial drilling compared with rigid guide pins placed by anteromedial drilling had a longer intraosseous length (42.0 vs 32.5 mm), were farther from the posterior border of the femur (15.0 vs 3.5 mm), and exited further from the peroneal nerve (45.2 vs 37.2 mm). However, none of these differences were statistically significant. They also felt tunnels drilled with flexible reamers demonstrated more consistent lengths and position, reporting the tunnel lengths in 3 knees using rigid guide wires were less than 30 mm (25, 27, and 28 mm), and only 1 knee using a flexible guide pin had a tunnel length less than 35 mm (33 mm). Three knees with rigid guide pins placed the exit point at the posterior border of the femur. The closest distance to the posterior femur for a flexible guide pin was 6 mm, and the next closest knee was 9 mm. 21
As with all implants and instrument systems, there are potential disadvantages to using a flexible reamer system. Along with the potential complication we have addressed in this article, flexible reamer systems are more expensive than traditional rigid reamer systems, and one must decide if the advantages offset the increased cost. We feel the advantages gained by ease of positioning, avoiding hyperflexion of the knee, and a safe and predictable anatomic femoral tunnel justify the additional cost.
In summary, flexible reamer systems allow an additional way of uncoupling of the tibial and femoral tunnels to clearly visualize and establish an anatomic starting point within the femoral footprint of the native ACL while avoiding the complications associated with knee hyperflexion and straight reamers with the FAMP: namely, short femoral tunnels, possible posterior wall blowout, low arthroscopic flow and poor visualization, and iatrogenic damage to the medial femoral condyle.
Footnotes
Declaration of Conflicting Interests
The authors declared that they have no potential conflicts of interest in the authorship and publication of this contribution.