
Abstract
Background
Resorbable anchors are widely used in arthroscopic stabilization of the shoulder as a means of soft tissue fixation to bone. Their function is to ensure repair stability until they are replaced by host tissue. Complications include inflammatory soft tissue reactions, cyst formation, screw fragmentation in the joint, osteolytic reactions, and enhanced glenoid rim susceptibility to fracture.
Purpose
To evaluate resorption of biodegradable screws and determine whether they induce formation of areas with poor bone strength that may lead to glenoid rim fracture even with minor trauma.
Study Design
Case series; Level of evidence, 4.
Methods
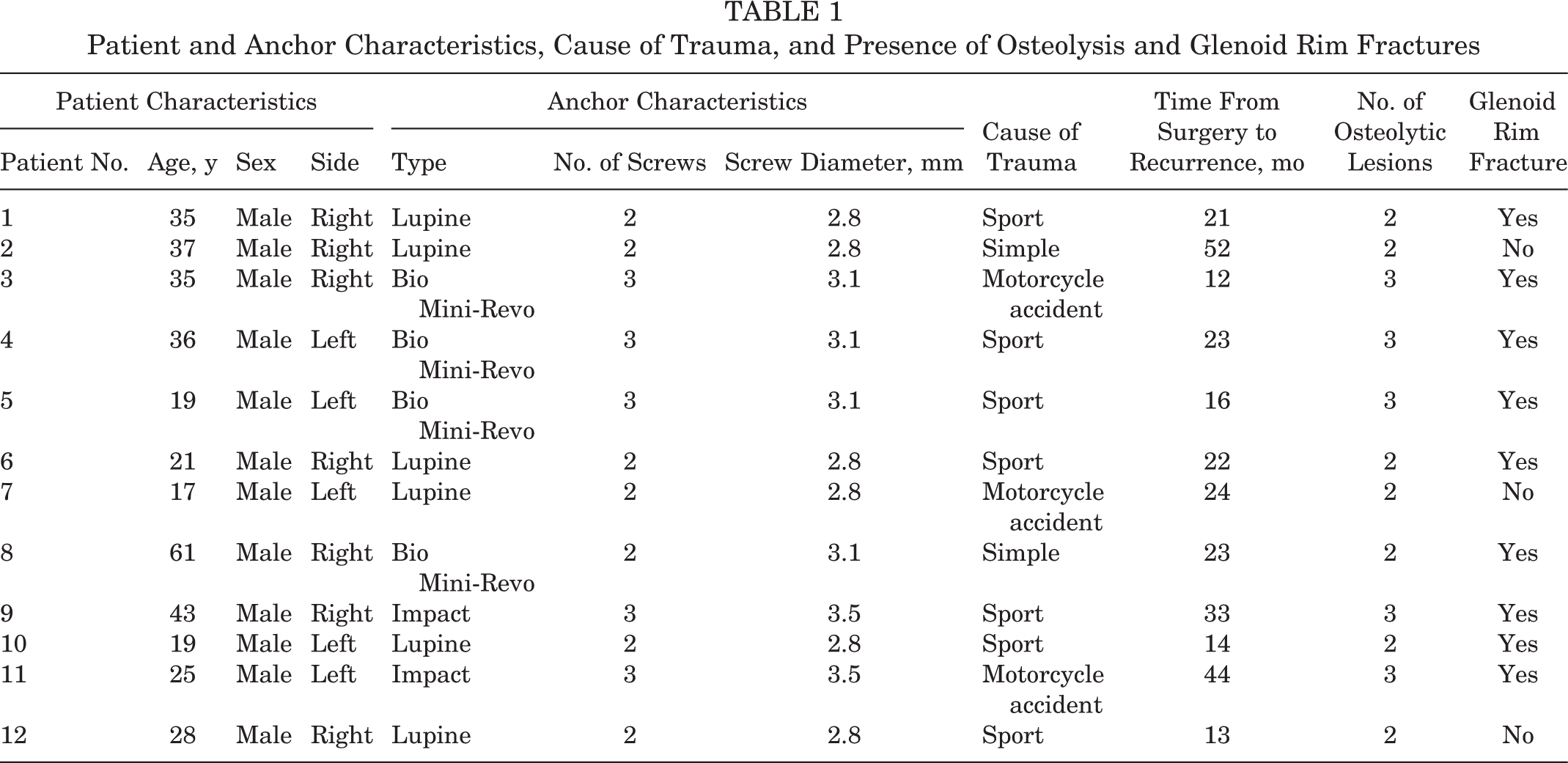
This study evaluated 12 patients with anterior shoulder instability who had undergone arthroscopic stabilization with the Bankart technique and various resorbable anchors and subsequently experienced redislocation. The maximum interval between arthroscopic stabilization and the new dislocation was 52 months (mean, 22.16 months; range, 12-52 months). The mean patient age was 31.6 years (range, 17-61 years). The persistence or resorption of anchor holes; the number, area, and volume of osteolytic lesions; and glenoid erosion/fracture were assessed using computed tomography scans taken after redislocation occurred.
Results
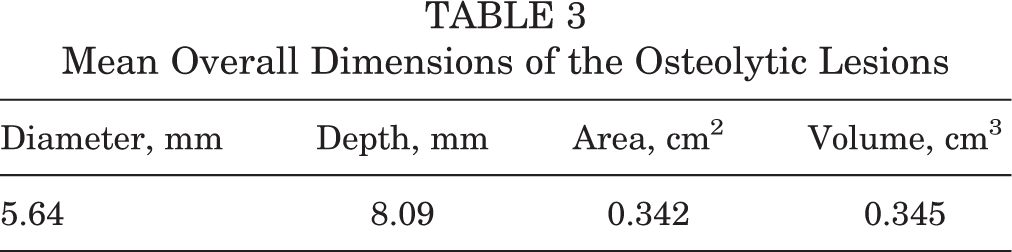
Complete screw resorption was never documented. Osteolytic lesions were found at all sites (mean diameter, 5.64 mm; mean depth, 8.09 mm; mean area, 0.342 cm2; mean volume, 0.345 cm3), and all exceeded anchor size. Anterior glenoid rim fracture was seen in 9 patients, even without high-energy traumas (75% of all recurrences).
Conclusion
Arthroscopic stabilization with resorbable devices is a highly reliable procedure that is, however, not devoid of complications. In all 12 patients, none of the different implanted anchors had degraded completely, even in patients with longer follow-up, and all induced formation of osteolytic areas. Such reaction may lead to anterior glenoid rim fracture according to the literature and as found in 75% of the study patients with local osteolysis (9/12). Reducing anchor number and/or size may reduce the risk of osteolytic areas and anterior glenoid rim fracture.
For decades, open Bankart repair and capsular shift have been the gold standard surgical treatments for anterior shoulder instability. Advances in arthroscopic techniques have involved a steady shift toward arthroscopic procedures. 17,24 Further technical progress has vastly improved arthroscopy, so much so that recent studies comparing current arthroscopic techniques with open procedures report similar rates of recurrence. 4,5,7,12 Advances in biomedical materials have led to the introduction of a succession of new, effective devices to achieve fixation of the capsulolabral complex to the scapular glenoid. 10 The main disadvantages of metal implants include magnetic resonance imaging (MRI) artifacts, the release of metal ions in tissue, the need for a surgical procedure in case of device removal, and increased complexity of revision surgery. For these reasons, biodegradable anchors are commonly preferred in arthroscopic stabilization procedures. Resorbable anchors are compatible with MRI and computed tomography (CT), and they provide options for easier revision surgery 9 while ensuring primary stability equivalent to that obtained with nonresorbable devices. 15 A major characteristic of biodegradable materials is that they are eventually replaced by host tissue. Although the early stages of degradation involve formation of fibrous tissue, 19,27,28 little is known about actual anchor resorption and replacement with host tissue. Complete device replacement by bone has not been demonstrated either experimentally or clinically in most patients. 29 Complications associated with biodegradable devices include cyst formation, inflammatory reactions, fragment dispersion in the joint, and local osteolysis. 6,18,30 Although several investigators have reported osteolytic lesions at the site of the bioresorbable implants, § an association between osteolysis and poor clinical outcomes has never been documented. The study’s purpose was to evaluate the consistent finding of osteolysis about bioresorbable suture anchors in 12 cases of redislocation after arthroscopic repair and its potential role as a predisposing factor to glenoid fracture. Our hypothesis was that in the presence of osteolytic lesions, the anterior glenoid rim is less resistant to trauma, and therefore the use of bioresorbable suture anchors should not be recommended in contact sport athletes.
Methods
This study was conducted at the Department of Shoulder Surgery at Cervesi Hospital (Cattolica, Italy), directed by the senior author (G.P.). It involved 12 male patients, all of whom had undergone arthroscopic stabilization of the shoulder by the Bankart technique and subsequently experienced a redislocation. The original operation had been performed by the same surgeon (G.P.). Redislocation was treated by open stabilization with Bristow-Latarjet coracoid transfer. We analyzed the epidemiological and CT findings of patients who experienced recurrence. There were 9 left (75%) and 3 (25%) right shoulders. Different types of anchors, with different diameters, had been implanted in the 12 patients: Lupine Loop Plus suture anchor with No. 2 Panacryl, polylactic acid (PLA; DePuy Mitek) (6 patients [50%]; anchor diameter, 2.8 mm), Bio Mini-Revo Anchor Self-Reinforced 96L/4D PLA with No. 2 Hi-Fi high-strength suture (ConMed Linvatec) (4 patients [33.3%]; anchor diameter, 3.1 mm), and Impact Suture Anchor Self-Reinforced 96L/4D PLA Copolymer with 2 strands of braided polyester (ConMed Linvatec) (2 patients [16.6%]; anchor diameter, 3.5 mm). Labrum repair was performed with different numbers of anchors: 7 patients had received 2 anchors (58.3%), and 5 patients had received 3 anchors (41.6%) (Table 1). The mean patient age was 31.6 years (range, 17-61 years). The maximum interval between arthroscopic stabilization and the new dislocation was 52 months (mean, 22.16 months; range, 12-52 months). The cause of recurrence was a sport injury in 7 patients (58.3%; all professional athletes), and simple trauma with the shoulder in abduction and external rotation was observed in 2 patients (16.6%). Three patients experienced recurrence after a motorcycle accident (25%). The reports and videos of the earlier procedures were reviewed by a blinded, unbiased surgeon for technical errors such as incorrect topographic positioning of the anchor. None of the patients had had glenoid erosion before arthroscopic stabilization, and none had associated lesions detected intraoperatively; all patients reported good shoulder stability without instability symptoms prior to the new dislocation. The persistence or enlargement of anchor holes; the number, area, and volume of osteolytic lesions; and glenoid erosion/fracture were assessed on CT scan (32-detector CT scanner; General Electric) performed at our hospital after injury.
Patient and Anchor Characteristics, Cause of Trauma, and Presence of Osteolysis and Glenoid Rim Fractures
Data Processing, Radiographic Evaluation Criteria, and Statistical Analysis
The CT scan evaluation and all measurements were performed using the image processing software OsiriX (v 3.7.1; Pixmeo). Osteolytic lesions were defined as areas (zones) of bone resorption having a diameter and volume exceeding those of the anchor. The volume of each lesion (in cm3) was calculated by measuring its area on the sagittal plane and its depth on the axial and coronal planes (Figure 1). The mean dimensions of osteolytic lesions were obtained from measurements performed by 3 independent raters (orthopaedic surgeons with 20 years of experience in shoulder surgery) at 3 different points of time. The Pearson correlation coefficient was applied to test interobserver reliability.

Measurement of the osteolytic lesion dimensions.
Results
We found no statistically significant association between glenoid rim fracture and anchor number, anchor type, or volume of osteolytic lesion. We also did not find any correlation between patient age and the incidence of osteolytic lesions or glenoid rim fracture.
Among the 12 patients with recurrence of shoulder dislocation, we observed that all were characterized by the presence of osteolysis around the anchors. In these patients, none of the anchors implanted showed signs of resorption. Seven patients presented 2 osteolytic lesions, and 5 presented 3 osteolytic lesions. We observed 9 patients with anterior glenoid rim fracture (75%).
Patients’ epidemiological data, anchor number and characteristics, type of trauma, presence of osteolysis, and glenoid rim fractures are listed in Table 1.
The mean (±SD) diameter of the osteolytic lesions detected was 5.64 ± 3.48 mm (range, 2.85-14.5 mm). The mean depth of the osteolytic lesions was 8.09 ± 3.37 mm (range, 3.2-15.4 mm). The mean osteolytic area was 0.342 ± 0.43 cm2 (range, 0.06-1.87 cm2), and the mean volume of the lesions was 0.345 ± 0.52 cm3 (range, 0.2-2.14 cm3).
The mean diameter of the osteolytic lesions (measured on the sagittal plane) and their maximum depth (measured on the axial and coronal planes) are reported in Table 2. The mean dimensions of the osteolytic lesions are reported in Table 3. The Pearson correlation coefficient was 0.86 (nearly perfect agreement) for all measurements (P < .05).
Mean Diameter and Maximum Depth of the Osteolytic Lesions a

a Lesion diameter was measured on the sagittal plane and lesion depth was measured on the axial and coronal planes of computed tomography scans.
Mean Overall Dimensions of the Osteolytic Lesions
Discussion
Implanting metal fixation anchors in the joint space involves more complications than using resorbable implants, but the latter devices may also entail some complications. Among these, formation of osteolytic lesions at the anchor site has attracted the interest of the orthopaedic community because it might closely correlate with the clinical outcomes of patients treated for shoulder instability. Bioresorbable devices can induce formation of large osteolytic defects, since they often fail to be replaced with bone tissue, but the cause is still unclear. Previous clinical studies found considerable drill hole enlargement after bioresorbable anchor use. Ejerhed et al
11
found visible or cystic drill holes on plain radiographs 33 months after surgery; moreover, visible drill holes or drill holes with cystic changes did not appear to heal during the follow-up period. A recent clinical radiographic study of the drill holes in patients subjected to arthroscopic capsulolabral repair
25
found that drill holes tended to enlarge over time, negatively affecting clinical outcomes. As defect enlargement was not found in equal measure at all implant sites, local factors besides the presence of the anchor itself may be involved. To the best of our knowledge, no studies have attempted to correlate these osteolytic reactions with clinical data after shoulder instability surgery. In a recent study, Kim et al
16
reported the presence of different grades of osteolytic lesions after the use of biodegradable suture anchors (poly(

Resorbable devices (2 Bio Mini-Revo anchors) recovered from a patient who experienced redislocation (patient 8) after 23 months of follow-up. A large glenoid rim fracture was found along the anchor holes.
Limitations
This study has some limitations. The devices implanted in our 12 patients were different in size, number, and material, preventing correlation of osteolytic lesions to anchor type. Second, although all 12 patients experienced a redislocation, the presence of osteolysis cannot be generalized to all patients with recurrent dislocation because of the lack of a control group. Moreover, the absence of a control group means that it cannot be demonstrated whether these lesions are also found in asymptomatic patients. The advantages of our study include the fact that all patients were operated on with the same technique by the surgeon who had previously performed the arthroscopic stabilization procedures. Moreover, none of the 12 patients had a glenoid fracture at the time of the stabilization procedure, indicating an intact anterior glenoid rim. Finally, the osteolytic lesions were measured 3 times by 3 different orthopaedic surgeons to maximize accuracy.
Conclusion
Arthroscopic stabilization of the shoulder using resorbable fixation devices is a highly reliable surgical procedure that is, however, not devoid of complications. One of the most insidious problems is formation of osteolytic lesions at the anchor site. Our study showed that most of the anchors had not completely degraded and had induced osteolysis at the screw site. These lesions may weaken the anterior glenoid rim, increasing the risk of a glenoid rim fracture. The use of bioresorbable devices should thus be carefully evaluated, especially in young, active patients like contact sport athletes. New, smaller devices made from osteoinductive materials could help reduce the incidence and/or size of osteolytic lesions.