
Abstract
Background:
Superior labrum anterior posterior (SLAP) lesions often cause shoulder pain, dysfunction, and instability. Professional athletes require a high level of shoulder function for competition and overhead activities.
Purpose:
To evaluate elite athletes who had arthroscopic surgery for common shoulder pathologies and SLAP lesions with a follow-up of more than 3 years. The associated intra-articular pathologies and return to play were documented.
Study Design:
Case series; Level of evidence, 4.
Methods:
Thirty-five shoulders in 34 elite athletes (4 women and 30 men; mean age, 25 years [range, 18-32 years]) had arthroscopic repair of SLAP lesions and accompanying Bankart or rotator cuff tears between January 2008 and November 2011. The documentation included patient symptoms, physical examination, radiological analysis with radiographs, and magnetic resonance imaging. Shoulder function was evaluated preoperatively and at follow-up using American Shoulder and Elbow Surgeons (ASES) and Kerlan Jobe Orthopaedic Clinic (KJOC) scores. The mean follow-up was 52 months.
Results:
Isolated SLAP lesions were seen in 17.1% of patients, SLAP lesions and partial cuff tear occurred in 25.7%, associated Bankart lesions in 37.1%, full-thickness rotator cuff tears in 8.6%, Bankart and posterior labrum lesions in 8.6%, and Bankart and full-thickness rotator cuff tears in 2.9%. Return to play was a mean 6.4 ± 1.5 months. The mean postoperative ASES and KJOC scores were 89.6 ± 4.6 and 80.9 ± 6.8, respectively, compared with preoperative scores of 64.0 ± 7.2 and 50.5 ± 10.3 (t test, P < .01).
Conclusion:
The majority (88.2%) of professional athletes returned to their preinjury levels. SLAP lesions may frequently occur with Bankart lesions and rotator cuff tears. A high rate of return to sport at the same level of athletic performance can be achieved by anatomic repair and effective rehabilitation.
Keywords
Lesions of the superior labrum anterior posterior (SLAP) to the biceps tendon were first described in 1985 by Andrews et al. 2 In athletes, tensile overload during throwing with eccentric biceps contraction lifts the biceps tendon off its glenoid insertion leading to labral injuries. Snyder et al 23 classified detachment of the labrum biceps complex from the superior glenoid rim into 4 types and reported type II as the most prevalent. Maffet et al 13 found an incidence of 11.8% for labral lesions in their series of 712 consecutive shoulder arthroscopies. SLAP lesions are frequently associated with other intra-articular pathologies, including Bankart lesions and posterior labrum and rotator cuff tears 12,23 that cause shoulder pain, dysfunction, and instability. 10 Athletes require a high level of shoulder function for competition and overhead activities.
In this retrospective study, we evaluated 34 elite athletes who had arthroscopic surgery for common shoulder pathologies along with SLAP lesions with a follow-up of more than 3 years. The associated intra-articular pathologies and return to play were documented.
Methods
This study was approved by our institutional review board. We retrospectively reviewed 355 shoulder arthroscopies performed between January 2008 and November 2011. Among those injuries, we documented 35 (9.9%) shoulders with SLAP lesions in 34 patients who were elite professional athletes. Patients who had previous shoulder surgery, less than 3 years of follow-up, or who were participating in sports at the recreational level were not included. There were 4 women and 30 men, with a mean age of 25 years (range, 18-32 years). All surgeries were performed by the senior surgeon (T.B.). There were 27 right and 8 left shoulders (30 dominant and 5 nondominant). All elite athletes except 2 (soccer, arm wrestling) were overhead sports professionals at a national and international level (8 volleyball, 8 American football, 7 basketball, 4 tennis, 2 handball, 2 weight lifting, 1 swimming). Demographic data of the athletes are summarized in Table 1.
Demographic Data of Athletes

The patients’ symptoms, physical examinations, and radiological analyses were documented. Comprehensive shoulder examinations were performed. Most patients had tenderness at the rotator interval. Patients were evaluated with a provocation test for pain and apprehension with the shoulder at 90° of abduction and maximal external rotation, 15 standard apprehension test for anterior instability, Speed and O’Brien tests for anterior SLAP lesions, and Jobe relocation test for posterior labrum lesions. 7
All patients underwent anteroposterior, axillary, and scapular Y radiographs and 3.0-T magnetic resonance imaging (MRI). Anatomic changes occurring within the shoulders of throwing athletes were documented with MRI. The changes included paralabral cyst formation, posterior superior humeral head cystic changes and/or bone bruise, articular side partial rotator cuff tear, and irregularity of the labrum. 9 These MRI findings suggested internal impingement in the throwing athletes. 24
After clinical and imaging examinations, labral lesions were confirmed using arthroscopy. All shoulder arthroscopies were performed under general anesthesia in the beach-chair position. After standard arthroscopic evaluation and confirmation of diagnosis (Figure 1), labrum stabilizations were performed with PushLock (Arthrex Inc) knotless suture anchors.

Arthroscopic view of a type II superior labrum anterior posterior (SLAP) lesion in an elite athlete.
All the associated pathologies were also repaired along with the SLAP tear. A double-row repair technique was used for full-thickness rotator cuff tears. Partial-thickness articular-sided rotator cuff tears (depth less than 50% of the tendon) were debrided using a shaver and radiofrequency device (ArthroCare Corp).
All patients had rehabilitation at the same center with similar physiotherapy programs depending on the repaired pathologies. All shoulders were positioned in a sling, and pendulum exercises were immediately begun. Posterior capsular and scapulothoracic stretching and strengthening were the most important part of the early rehabilitation. Daily activities of overhead elevation and external rotation were allowed immediately. Patients were expected to regain full range of motion by 6 to 8 weeks, followed by rotator cuff strengthening without any resisted biceps work until 10 weeks. Throwing programs were initiated after 12 to 14 weeks.
Shoulder function was evaluated preoperatively and at follow-up with American Shoulder and Elbow Surgeons (ASES) and Kerlan Jobe Orthopaedic Clinic (KJOC) scores. Statistical analysis was conducted to determine the differences between the preoperative and postoperative scores using the Student t test and SPSS version 20.0 (IBM Corp). Statistical significance was accepted as P < .01 for all analyses.
Results
In this study, isolated SLAP lesions were seen in 17.1% of patients, SLAP lesions with partial cuff tears occurred in 25.7%, with associated lesions consisting of Bankart in 37.1%, full-thickness rotator cuff tears in 8.6%, Bankart and posterior labral lesions in 8.6%, and Bankart lesion and full-thickness rotator cuff tear in 2.9% (Table 2). Full-thickness rotator cuff tears of the supraspinatus tendon were less than 2 cm in length. Partial-thickness rotator cuff tears occurred at the articular side of the cuff localized between the supraspinatus and infraspinatus tendons and were less than 50% of the tendon thickness.
Associated Pathologies of SLAP Lesion a
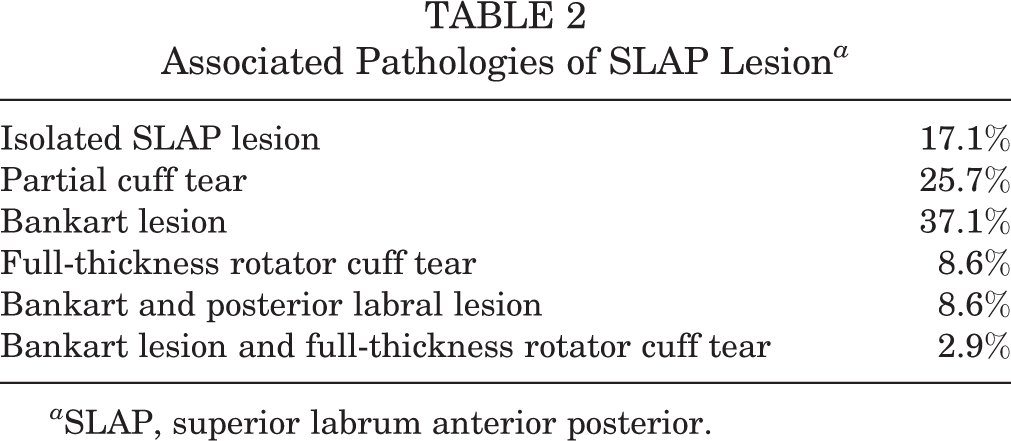
a SLAP, superior labrum anterior posterior.
All labral tears were repaired using a mean 3.6 ± 1.8 (range, 2-7) knotless suture anchors. a mean return to play time was 6.4 ± 1.5 months (range, 4-13 months). Mean preoperative ASES score was 64.0 ± 7.2 (range, 45-72), and mean KJOC score was 50.5 ± 10.3 (range, 35-65). Postoperative last follow-up ASES scores had a mean of 89.6 ± 4.6 (range, 86-100), and KJOC scores had a mean of 80.9 ± 6.8 (range, 69-92). Regarding KJOC scores, all patients were graded fair before surgical treatment. The KJOC scores after surgical treatment revealed 2 excellent (5.7%), 17 good (48.6%), 15 fair (42.9%), and 1 poor (2.9%). Differences between pre- and postoperative scores were statistically significant (t test, P < .01). Follow-up results are summarized in Table 3.
Follow-up Results of Athletes a
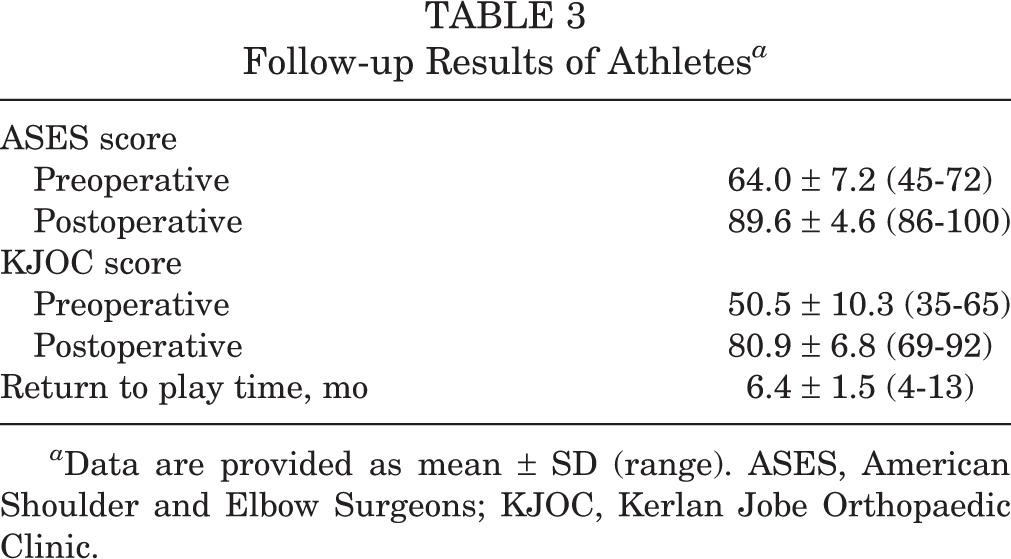
a Data are provided as mean ± SD (range). ASES, American Shoulder and Elbow Surgeons; KJOC, Kerlan Jobe Orthopaedic Clinic.
The mean follow-up was 52 months (range, 36-82 months). There were 2 complications requiring revision surgery. One of the female handball players had a recurrent labral tear due to cutting of the repaired labrum by suture, probably caused by insufficient healing of the labrum to the glenoid. After arthroscopic labral re-repair, she was able to return to sports. A male weight lifter had reinjury due to a shoulder dislocation with a bony Bankart lesion, and revision surgery was performed by open bony-bloc technique. He was not able to return to professional sports. Eighty-eight percent of professional athletes (30 athletes) returned to sports at preinjury levels. Four patients were not able to return to play at the same level.
Discussion
There have been numerous studies documenting satisfactory outcomes of arthroscopic SLAP repair. 3,5,6,27 Clinical studies revealed that elite athletes had greater challenges in returning to their preinjury levels of play in spite of successful postoperative outcome scores. Ide et al 8 found that 90% returned to normal function; however, only 75% of athletes were able to return the same level of competition. Neri et al 17 reported that 57% of athletes returned to their preinjury levels of sports, 26% returned to sports but were limited by pain, and the remaining 17% were unable to return to sports. Neuman et al 18 retrospectively reviewed the outcomes of SLAP repair in 30 athletes. The average ASES and KJOS scores were 87.9 and 73.6, respectively. Eighty-four percent of athletes returned to play. 18 Park et al 20 reported 75% of overhead athletes were able to return to play, whereas only 38% of baseball players were able to return to play. In this study, 88.2% of professional athletes were able to return to preinjury levels of competitive sports activities.
Several scores that focus on activities of daily living have been used to evaluate shoulder function. The KJOC shoulder and elbow score was designed for performance evaluation of elite athletes. This score could be used to distinguish minor changes in endurance, velocity, power, or control. 17 We reported mean postoperative ASES and KJOC scores of 89.6 and 80.9, respectively. We believe the ASES score is more suitable for evaluation of activities of daily living, and the KJOS score is more detailed, allowing for evaluation of high-demand elite athletes. The ASES score is not adequate to evaluate return to competition. A higher ASES score may only represent satisfaction in activities of daily living, such as dressing, bathing, and toileting. 18 The KJOS score provides a more comprehensive measure of athletic activity to assess changes in warm-up time, pain with competition, weakness, feeling instability, difficulties with management or coaches, throwing mechanism, changes in power or velocity, endurance limitation in competition, control of the affected arm, and desired level of competition. 1
SLAP tears are commonly found with coexisting shoulder pathology, including Bankart tears and undersurface partial or complete rotator cuff tears. In a report of 129 cases with SLAP tears, Kim et al 12 found that 88% of patients had concomitant pathology. Snyder et al 23 reported arthroscopic repair of 140 SLAP lesions; they found only 28% had isolated SLAP tears, 29% had a partial rotator cuff tear, 11% had a full-thickness rotator cuff tear, and 22% had a Bankart lesion. Similar to previous reports, in the present study, 82.9% of the athletes with SLAP lesions had additional pathology. We observed that SLAP tears were commonly associated with labral lesions. SLAP lesions with concomitant Bankart tears are difficult to treat. Four patients in this series who were unable to return to play had SLAP tears with associated Bankart lesions.
Magnetic resonance imaging of the shoulder has been found to be a suitable method for the detection of labral tears, but some series have found that a number of pathologies may be missed. 4 Distinguishing between normal and pathologic anatomy is important. 4 The use of gadolinium-enhanced MRI may improve diagnostic accuracy of labral lesions and partial rotator cuff tears. 24 Magee and Williams 14 reported that MRI of the shoulder at 3.0 T is very sensitive, specific, and accurate in the diagnosis of labral tears compared with arthroscopy. We did not use gadolinium-enhanced MRI. A good history and physical examination is still most important in the diagnosis of shoulder pathology in athletes. Because shoulder complaints are frequently combined, examination under anesthesia, MRI, and arthroscopy can be helpful in accurate clinical diagnosis.
The injury mechanism of posterior labrum tears may be a direct force, repetitive microtrauma, or internal impingement. 21 In our experience, SLAP lesions and posterior labral tears are frequently observed in basketball players. While playing defense, basketball players elevate their hands overhead at a 45° angle. A front-to-back force on the arm in this position is the most common cause of posterior labral tears.
Chronic microtrauma to the inferior glenohumeral ligament results in insidious anterior and inferior instability in the athletes. Glenohumeral joint external rotation results in tension upon the rotator cuff and internal impingement of the tuberosity upon the posterior and superior glenoid that produces articular surface rotator cuff tears. 22 Morgan et al 16 postulated that SLAP lesions occurred because posterior superior instability by a secondary anterior inferior pseudolaxity caused chronic superior instability that leads to secondary partial-thickness articular rotator cuff tear. Consequently, labral pathologies should be suspected in overhead athletes with partial articular rotator cuff tears. Van Kleunen et al 25 found that the success rate of SLAP repairs was lower when there was a concomitant rotator cuff defect in elite athletes. Conversely, Oh et al, 19 in 2011, determined that concomitant SLAP and rotator cuff repair may not have an adverse effect on the outcome. Our results, like those of Oh et al, 19 indicate that treatment of combined SLAP and rotator cuff tears resulted in a good functional outcome.
Overhead athletes frequently have increased external rotation and a loss of internal rotation. This situation occurs owing to posterior capsular contracture, anterior capsular laxity, and increased humeral retroversion. The balance of glenohumeral internal and external rotation is necessary for effective pitching and minimalizes translation of the glenohumeral joint. 11 Wilk et al 26 reported an increase in the incidence of shoulder injuries due to alteration of the glenohumeral motion kinematics. Training programs should be modified to correct the glenohumeral internal rotation deficiency in overhead athletes. Posterior capsular stretching and anterior capsular strengthening exercises may prevent injury and improve recovery during postoperative rehabilitation.
The weaknesses of this study include the retrospective analysis of a cohort of only 34 elite athletes. The small number of patients did not allow for comparison between patients participating in different sports or analysis of specific lesions.
Conclusion
Shoulder pain is a common complaint in elite overhead athletes. SLAP lesions are a common cause of shoulder pain and functional impairment. Clinical diagnosis is very important because of lack of diagnostic tests and different accompanying lesions. The KJOC score is suitable for evaluation of elite athletes’ shoulder injuries. Depending on the mechanism of injury, SLAP lesions may frequently occur with Bankart or posterior labral lesions and rotator cuff tears. Anatomic repair and aggressive rehabilitation facilitate a high rate of return to sport at the same level of athletic performance.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.