
Abstract
Background:
Concussions have become a major public health concern for both youth and professional athletes. The long-term consequences of concussion can be debilitating or even life threatening. To reduce these concerns, baseline neurocognitive performance can aid decision making in postconcussion recovery and return to play for athletes sustaining concussions. To date, these data are not available for lacrosse athletes.
Purpose:
To present baseline neurocognitive performance for Major League Lacrosse (MLL) players and to determine differences between athletes with and without a history of concussion.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A retrospective review was conducted of Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) scores from MLL players who completed baseline testing from June 2010 to June 2011. Inclusion required a valid baseline test and no history of concussion in the 3 months prior to testing. Means ± standard deviations were computed for all demographic variables and ImPACT composite scores including visual and verbal memory, reaction time, and visual motor processing speed. Independent-samples t tests were used to determine differences between athletes with and without a history of concussion.
Results:
Valid baseline ImPACT testing was available for 235 MLL athletes (mean age, 25.1 ± 3.0 years). Forty percent of MLL athletes (n = 94) reported a history of concussion, with 14% of those (n = 13) reporting a history of 3 or more previous concussions. There were no differences on any demographic variables between MLL athletes with and without a history of concussion. MLL athletes with a history of concussion had lower ImPACT composite scores than those without a history of concussion, although only the verbal memory composite was found to be statistically significant (MLL with concussion, 83.2 ± 10.8 vs MLL without concussion, 86.9 ± 9.5; P = .007).
Conclusion:
This study establishes baseline ImPACT scores for MLL and demonstrates that athletes with a history of concussion have poorer neurocognitive performance compared with MLL athletes without a history of concussion.
Clinical Relevance:
These data can serve as normative values for subsequent testing following concussion to assess neurocognitive recovery.
Lacrosse is one of the fastest growing sports in the United States. There is an increasing concern about the incidence of concussion in lacrosse. Studies have shown that the incidence of concussion among high school boys was third highest in lacrosse athletes, second to football and ice hockey. 19,25 The most commonly reported mechanism of concussion in lacrosse is player-to-player contact, predominantly initiated with the player’s head. 18
Neurocognitive testing has become increasingly popular because of the potential long-term consequences resulting from concussion. Postconcussion testing can help identify impairments (eg, impaired reaction time) that might otherwise be missed or cannot be measured on a standard clinical examination; however, more data are needed to support its use. Many concussion experts recommend the implementation of baseline neurocognitive testing for athletes regardless of age or performance level. Individual baseline testing establishes cognitive ability of athletes in a healthy state prior to injury to best manage athletes following a concussion. In the absence of baseline scores, normative values can help determine cognitive recovery and guide return-to-play decision making.
Computerized neurocognitive tests such as Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) have been specifically developed for the evaluation of sport-related concussions. Sensitivity and specificity values have been reported to be 91.4% and 69.1%, respectively, in the acute stages of concussion. 36 Demographic variables, including age and sex, as well as concussion history can influence the results of baseline testing. Studies have suggested that athletes with a history of concussion show lingering performance declines on subsequent neurocognitive testing. 14,30 Therefore, establishing appropriate normative baseline reference values is important for subsequent testing to monitor recovery.
To date, studies have focused on neurocognitive function in professional football players, 23,31 –33,37 professional hockey players, 1 high school athletes, 12,21,26 and collegiate athletes. 11,12,24,26,27 No published studies have investigated the neurocognitive function in professional lacrosse athletes. Therefore, the purpose of this study was 2-fold: (1) to establish neurocognitive reference values for professional lacrosse players and (2) to determine whether neurocognitive performance in lacrosse athletes is influenced by history of concussion. We hypothesized that there will be no difference in neurocognitive test measures between professional lacrosse athletes and published data on contact athletes and that professional male lacrosse athletes with a history of concussion would perform worse on neurocognitive test measures than their peers without a history of concussion.
Materials and Methods
We retrospectively reviewed data from Major League Lacrosse (MLL) players who completed baseline neuropsychological testing from June 2010 to June 2011. ImPACT testing was mandated by the league to be completed by all athletes prior to the start of the season. All athletes individually completed the online version of the ImPACT test. 10 Any athlete with an invalid test score or who had a concussion 3 months prior to testing was excluded from the study. Test scores are determined as invalid by the ImPACT program based on an algorithm of composite and subscale scores as described in the ImPACT Clinical Interpretation Manual. 20 Approval for this study was obtained by Major League Lacrosse and the Orthopaedic Foundation.
Neuropsychological testing was completed using ImPACT, a validated, computerized neuropsychological test designed to assess the neurocognitive effects of sports-related concussions. 10,16,34,35 ImPACT consists of 7 modules that measure attention, verbal and visual memory, reaction time, and information processing speed. 13,20,22 Four composite scores are calculated: visual memory, verbal memory, reaction time, and visual motor processing speed. 13,20,22 Verbal memory assesses memory of words. Visual memory assesses memory of patterns and shapes. Visual motor speed is the speed at which the participants recognize objects. Verbal memory, visual memory, and visual motor speed are reported on a scale from 0 to 100 as well as age- and sex-normalized percentiles. Reaction time is the speed of response to visual objects and is reported in seconds and as age-normalized percentiles. A score of 1.0 is the slowest, least optimal score, with lower scores indicating a faster reaction time. An impulse control composite score is also generated as a validity index; a lower score indicates better performance.
In addition, ImPACT collects demographic information including age, years of education, concussion history, sports participation, and medical-related information as well as an inventory of current symptoms using the Post-Concussion Symptom Scale (PCSS). 13,20,22 The PCSS is a 22-item questionnaire of symptoms associated with concussion. Each symptom is graded on a 7-point Likert-type scale, and a total PCSS score is computed as a sum of each symptom score. A higher PCSS score indicates greater perceived severity of concussive symptoms. Self-report questions pertaining to the number of previous concussions are also included in the demographic portion of the ImPACT test. Classification of athletes on history of concussion was derived from these questions.
Data were compiled and statistical analysis performed using Microsoft Office Excel 2003. Means ± standard deviations were computed for all variables to establish a normative database for this population. Athletes were divided into 2 groups for analysis based on whether they reported a history of concussion. Independent-sample t tests were used to determine differences between athletes with and without a history of concussion on ImPACT composite scores. A Bonferroni correction was applied to correct for multiple comparisons (.05/6), resulting in a significance level of .008.
Results
A total of 244 MLL players completed baseline ImPACT testing as part of the preseason requirement. Of these players, 11 players had invalid scores. Four players repeated baseline testing and had valid scores on reassessment. Six players did not repeat baseline testing, and 1 player completed 2 retests, both of which were invalid; therefore, these players were not included in the final analysis. Two players reported a recent concussion at baseline assessment and were therefore not included in the final analysis. Player 1 reported a concussion 8 days before testing. Player 2 reported a concussion 67 days before testing. His total symptom score was 13; he reported 8 previous concussions with mental confusion following injury, and 5 of 8 concussions reported resulted in loss of consciousness.
Subject characteristics are reported in Table 1. No athletes reported a history of brain injury or autism. There were no differences between athletes with and without a history of concussion on any demographic variable (P > .05).
Subject Characteristics a

a Values are reported as n (%) unless otherwise indicated. ADD, attention deficit disorder; ADHD, attention deficit hyperactivity disorder.
A total of 153 concussions were reported by 94 of 235 athletes (40%). In athletes reporting a history of concussion, the average time from last reported concussion to ImPACT testing was 5.5 ± 4.0 years. Thirteen athletes (6%) reported a history of 3 or more concussions. Fifteen players reported having treatment for headaches; 60% of those reported having had a concussion. Ten players reported having treatment for migraines, with 60% reporting having had a concussion. Two players reported treatment for epilepsy. Both had a history of multiple concussions; 1 player had 4 concussions and the other had 3 concussions. Two players reported treatment for substance or alcohol abuse, and both reported concussions. Four players were treated for psychiatric conditions; 50% reported concussion. Seven players reported dyslexia, and 57% reported concussion. Thirty-four players reported attention deficit disorder or attention deficit hyperactivity disorder; 50% reported concussion.
Means ± standard deviations of ImPACT composite scores are presented in Table 2. Based on the F test, equal variances were assumed for all variables except impulse control score. A significant difference was found on verbal memory score between athletes with and without a history of concussion (t = 2.69, P = .007). There were no differences between groups on visual memory score (t = 1.61, P = .11), visual motor processing speed (t = 0.05, P = .96), reaction time (t = 0.28, P = .78), impulse control (t = 0.21, P = .83), or total symptom score (t = 1.91, P = .06) (Table 2). There were no differences on any of the ImPACT composite scores between athletes reporting a history of 1 to 2 concussions and athletes with reporting a history of 3 or more concussions (P > .05).
ImPACT Scores a

a Values are reported as mean ± SD (95% CI). ImPACT, Immediate Post-Concussion Assessment and Cognitive Testing.
b Major League Lacrosse (MLL) players with a history of concussion scored lower on the verbal memory composite score compared with MLL players without a history of concussion (P < .05).
Discussion
The purpose of this study was to establish baseline neurocognitive status in professional, male lacrosse athletes. We obtained data from 96% of lacrosse players in the MLL during the 2011 season. Forty percent of our study population (94 athletes) reported a previous history of concussion, and 6% (13 athletes) reported having sustained 3 or more concussions. There were no differences in demographic variables between athletes with and without a history of reported concussion. Athletes with a history of concussion scored similarly to those without a history of concussion on all ImPACT composite scores with the exception of verbal memory. Athletes with a history of concussion scored lower on verbal memory composite score compared with the cohort without a history of concussion.
To our knowledge, this study is the first to report neurocognitive performance in professional lacrosse players. A summary table of baseline neurocognitive data in other contact athletes has been included as a reference (Table 3). Our cohort scored similarly to data previously published in National Football League (NFL) football players on all ImPACT composite scores. 37 In comparison to age- and sex-normalized reference data of over 17,000 healthy athletes published by ImPACT, our study population performed in approximately the 50th percentile on all ImPACT composite scores, suggesting possible impaired neurocognitive performance compared with age- and sex-normalized healthy controls (Table 4). 20
Comparison of ImPACT Scores in MLL Players Compared With Other Published Normative Reference Values a
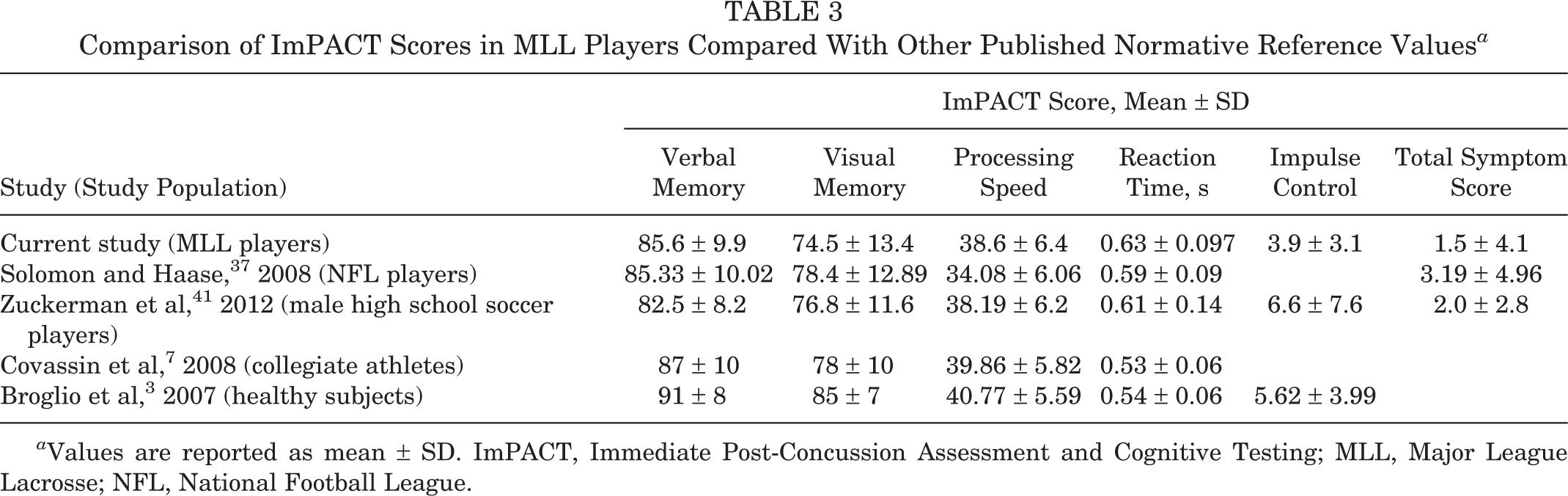
a Values are reported as mean ± SD. ImPACT, Immediate Post-Concussion Assessment and Cognitive Testing; MLL, Major League Lacrosse; NFL, National Football League.
Comparison of ImPACT Scores in MLL Players to Age- and Sex-Normalized Data a

a Data are reported for the entire sample as well as by reported concussion status (ie, players with and without a reported history of concussion). Values are reported as mean ± SD or as age- and sex-normalized percentiles based on published ImPACT normative data. 21 ImPACT, Immediate Post-Concussion Assessment and Cognitive Testing; MLL, Major League Lacrosse.
b Derived from Lovell and Solomon. 23
There is a growing body of evidence demonstrating the possible lingering effects of multiple concussions in athletes. 4,6,14,15 Collins et al 6 assessed the relationship between concussion history and neuropsychological performance in collegiate football players. They found that players with a history of 2 or more concussions perform worse than their peers without a history of concussion on neuropsychological tests that measure constructs of visual scanning, executive functioning, and information processing speed. Iverson et al 14 conducted a case-controlled study of 26 athletes with a history of 3 or more concussions matched to athletes of a similar demographic with no history of concussion. These authors found that athletes with a history of 3 or more concussions had worse verbal memory composite scores. In the present study, we found that athletes with a prior history of concussion scored lower on the verbal memory construct compared with athletes without a history of concussion; however, number of prior concussions did not appear to influence neurocognitive performance.
Reaction time, a common impairment following a concussive event, has been correlated with symptom severity and used as a measure of recovery following concussion. 9 Unexpectedly, our athletes had the worst performance on the reaction time composite score. Overall, our MLL athletes performed below the 30th percentile compared with age- and sex-normalized data in healthy athletes. 20 Impaired reaction time has been associated with injury. 38,39 A 2007 study demonstrated that collegiate athletes who sustained a noncontact ACL injury had lower baseline ImPACT scores, including slower reaction times and processing speeds compared with controls. 38 Therefore, the combination of slowed reaction time and a faster speed of play at the professional level could be detrimental and lead to subsequent injury if the athlete returns to sport without a complete recovery. Further research is warranted to investigate the impact of slower reaction times in this population to determine whether they are at increased risk for subsequent injury.
Proper diagnosis and management of athletes following concussion is key in minimizing short- and long-term consequences. 5 Symptoms alone do not appear to be sufficient indicators for diagnosis or recovery. 40 Studies have shown athletes underreport concussion-related symptoms. 28 Neurocognitive testing has the potential to detect cognitive impairment in otherwise asymptomatic athletes following a concussion. 2,8,27,36,40 Individual baseline data are ideal but not always available due the time-intensive nature of testing and expense. Furthermore, individual baseline testing is not endorsed by some due to poor test-retest reliability and self-report bias. 17,29 In the absence of such information, having appropriate normative reference values, such as those reported in this study, are important and necessary to monitor neurocognitive recovery. Future research should establish normative values for other sports and continue to explore differences between sports and competition levels.
There are several limitations to this study. The small sample size of athletes with history of concussions limits the ability to draw strong conclusions from these data due to low statistical power. While over one-third of our athletes reported a prior history of concussion, only 5% reported 3 or more concussions. Similarly, because of the small sample size of athletes aged 30 to 39 years, the results of stratification by age should be interpreted with caution and warrant further investigation. Third, we acknowledge that self-report of history of concussion is subject to recall bias, particularly when the average time from concussion was an average of 5 years. This may have led to misclassification of athletes based on history of concussion; however, medical documentation on prior concussions in these athletes was not available. Detailed documentation of concussions in all athletes is necessary to elucidate the short- and long-term effects of concussion and recurrent injuries in these athletes.
Conclusion
These data provide normative reference ImPACT scores for professional lacrosse players where currently data are lacking. These data support a possible age-related difference in ImPACT performance as well as in athletes with a history of 3 or more concussions. These baseline scores are necessary to serve as individual comparative values for subsequent postinjury testing, as reference values when baseline scores are missing, to improve the safety of the sport particularly for youth players, and for future research purposes.
Footnotes
The authors declared that they have no conflicts of interest in the development and publication of this contribution.