
Abstract
Background:
Scapular kinematic movement patterns between patients with subacromial impingement and healthy controls have been extensively investigated. However, a high degree of variability has been reported in the literature pertaining to differences between these 2 groups.
Purpose:
To investigate the influence of subacromial pain on scapular kinematics.
Study Design:
Controlled laboratory study.
Methods:
A total of 21 patients with stage 2 subacromial impingement who received local anesthetic injections as part of their normal treatment were recruited for this study. The postinjection kinematic data from these patients were compared with those of healthy age-, sex-, and arm dominance–matched controls.
Results:
Subacromial injections of anesthetics resulted in increased scapular anterior tilting; however, no changes were noted in upward or internal rotation. When compared with healthy controls, patients had greater anterior tilting and upward rotation of the scapula.
Conclusion:
The study findings indicate that the removal of pain in patients with impingement results in further dyskinesis of the scapula.
Clinical Relevance:
Pain may be causing patients with subacromial impingement to limit scapular tilt and upward rotation, and movement limitations may continue after an anesthetic injection.
Shoulder pain is the third most common musculoskeletal disorder reported in the general population. 36 In the United States, the direct annual cost for treating shoulder pain totals approximately $7 billion. 26 Of these musculoskeletal complaints, the most common diagnosis of shoulder pain is subacromial impingement syndrome. 10,38 Subacromial impingement is characterized by a reduction of the acromiohumeral distance, resulting in mechanical compression of the supraspinatus tendon beneath the acromion process of the scapula and the superior aspect of the humeral head. 1,28,30,32 For shoulder complaints resulting in medical intervention, 22% of treatments involves anesthetic injections with corticosteroids. 38
A reduction in the acromiohumeral distance is thought to be a factor contributing to rotator cuff degeneration, subacromial bursitis, and pain. 13,21,32,39 Kinematic factors such as superior humeral translations and scapular orientation may influence the acromiohumeral distance during elevation of the arm. 3,7,9,11,14 Both an increase in scapular anterior tilting (sagittal plane) and a decrease in upward rotation (coronal plane) may reduce the acromiohumeral distance during elevation of the arm, where anterior tilting of the scapula lowers the anterior acromion toward the head of the humerus and upward rotation elevates the lateral acromion away from the humerus. 11,13,29 The acromiohumeral distance has been reported to be lowest when the arm is elevated between 60° 7 and 90°, 14 thus highlighting the importance of scapular orientation at mid to high range of humeral motion. 21
Numerous studies have examined differences in scapular kinematics between patients with impingement versus healthy controls. 17,20,21,23,24,35 Although the kinematic findings from these studies are quite variable, the majority of these studies suggest that patients with impingement have more anterior scapular tilting than healthy controls during arm abduction and flexion and no differences in scapular external rotation when compared with healthy controls. 11,21,23 However, a recent meta-analysis including 9 studies indicated that constant patterns in kinematics cannot be established between patients with impingement and controls. 35 Because of the high between-subject variability for scapular kinematics, little is known regarding abnormal scapular motion and the impingement phenomenon. Furthermore, the etiology of impingement is somewhat of a conundrum; it is unknown whether patients first have scapular dyskinesia and then develop impingement or if the impingement leads to the scapular dyskinesia. In populations without impingement, such as wheelchair users, individuals with clinical shoulder pain have been reported to have greater upward rotation and anterior tilt of the scapula. 27 This finding suggests that pain may be associated with abnormal scapular motion. In addition, one case study found that patients with painful scapulothoracic tumors later developed subacromial impingement. 16 This finding suggests that subacromial impingement may be secondary to scapular dyskenisia when pain is present. 16
Local anesthetic injections in conjunction with corticosteroids are commonly administered to patients with stage 2 subacromial impingement syndrome by orthopaedic surgeons and general practitioners. 2,8,15 Stage 2 impingement is characterized by thickening of the subacromial bursa and deterioration of the supraspinatus tendon; however, stage 2 impingement does not include tearing of the supraspinatus tendon. 29 Local anesthetics are used as a diagnostic tool, as well as a modality to temporarily decrease shoulder pain. 8,15 Following subacromial anesthetic injections, patients have been reported to have increased humeral elevation 2,8,15 and increased strength in arm abduction and external rotation. 5,31 However, in patients with rotator cuff tears, a reduction in pain following a subacromial injection resulted in decreased scapulothoracic motion and greater reliance on glenohumeral motion during arm elevation. 33 A multitude of biomechanical differences have been reported for patients with cuff tears, which include changes in supraspinatus tendon length, 12 fatty infiltration of cuff muscles, 6 changes to the glenohumeral center of rotation, 9 and altered glenohumeral kinematics. 41 Therefore, the purpose of this study was to investigate whether patients with stage 2 subacromial impingement will respond favorably to an anesthetic subacromial injection. We hypothesize that the reduction of pain in patients with stage 2 impingement will result in decreased anterior tilt and increased upward rotation of the scapula during arm elevation. Furthermore, we hypothesize that posttreatment scapular kinematics will be similar to healthy controls.
Methods
Twenty-one patients (13 males, 8 females) with stage 2 impingement syndrome and 21 healthy control subjects were recruited for this study. Mean ± SD demographic data for patients were as follows: age, 55.6 ± 8.3 years; height, 174.1 ± 7.9 cm; and weight, 78.6 ± 13.4 kg. Mean ± SD demographic data for control participants, which were matched within 5 years of age to a patient of the same sex and arm dominance (19 right-handed individuals) were as follows: age, 54.4 ± 8.9 years; height, 172.9 ± 9.4 cm; and weight, 77.8 ± 15.1 kg. For the patient population, our inclusion criterion required a positive sign for at least 3 of the following 5 tests: Hawkins-Kennedy, Neer, painful arc, empty can (Jobe), and/or painful external rotation resistance. Patients having had shoulder surgery on the symptomatic side, a positive Spurling test, traumatic shoulder dislocation or instability in the past 3 months, reproduction of shoulder pain with active or passive cervical range of motion, or signs of a rotator cuff tear (drop-arm test, lag signs, gross external rotation weakness assessed by a manual muscle test) were excluded from this study. Radiographs were taken for all patients, and patients were excluded if the result of their image test indicated a rotator cuff tear, calcific bursitis, or any other pathology inconsistent with stage 2 subacromial impingement. The experimental protocol was approved by the institutional review board at the affiliation of the third author (A.K.). Written and verbal instructions of testing procedures were provided, and written consent was obtained from each subject prior to testing.
Instrumentation
The Fastrak magnetic tracking device (Polhemus) was used for collecting 3-dimensional in vivo kinematics of the shoulder complex (Figure 1). The Polhemus unit consists of a transmitter, 3 receivers, and a digitizer, all wired to a system electronics unit that determines the relative orientation and position of the sensors in space. The transmitter serves as a global reference frame and was fixed to a rigid plastic base and oriented such that its coordinate axes aligned with the cardinal planes of the human body. The digitizer sensor was used to identify anatomical landmarks with respect to the global reference frame. After digitization, the arbitrary coordinate systems defined by the Polhemus were converted to anatomically appropriate coordinate systems based on the recommendations of the International Society of Biomechanics Committee for Standardization and Terminology. 40

Experimental setup depicting electromagnetic scapular and humeral sensors.
Setup and Digitization
For digitization, participants were asked to stand in a neutral position with their arms relaxed by their sides. Once receivers were attached to the participant, they were not moved until the end of the entire protocol. The first receiver was placed on the thorax on the manubrium of the sternum at approximately the level of T3. The second receiver was positioned on the humerus by mounting it to an orthoplast device positioned on the proximal humerus with elastic straps. The final receiver was positioned over the scapula after mounting it on a custom scapular tracking device machined from plastic. 19 This tracker was attached to the scapular spine and posterior-lateral acromion with Velcro. The transmitter was then positioned approximately 30 cm behind the participant and was elevated to the height of their scapula. Anatomical landmarks were then digitized using the Polhemus stylus. The thoracic landmarks were T8, xiphoid process, C7, and jugular notch. The scapula landmarks were the root of the scapular spine, inferior angle, and posterior lateral boarder (acromial angle) of the scapula, which were digitized. The humeral landmarks were the medial and lateral epicondyles and the estimated center of the humeral head. To calculate the center of the humeral head, the humerus is manipulated in small circular arcs within the midrange of motion of the humerus. The center of the humeral head was defined by the point that moves the least with respect to the scapula through a least-squares algorithm during humeral calibration. 19 No materials were removed during the protocol or for the treatment phase, and only 1 calibration file was generated for the pre- and postinjection measurements for the patient group.
Experimental Procedure
Once the digitization and calibration were completed, participants completed 3 arm elevation trials. Each elevation trial consists of the patient raising their affected arm in the scapular plane (30° from the frontal plane) and returning along the same path to a count of 4 in each direction. Trials were repeated when the participant’s arm elevation deviated from the scapular plane (based on visual real-time feedback provided to the investigator digitally). Data were collected continuously at a rate of 40 Hz for the 3 trials and then averaged for data analysis. Patients were asked to give their current shoulder pain level on an analog pain scale immediately after completing the shoulder elevation task.
Following the scapular kinematic evaluation, patients received 2 subacromial injections of (1) anesthetic (3 mL lidocaine with epinephrine) and (2) corticosteroid (6 mL of 0.5% bupivacaine and 1 mL of 40 mg methylprednisolone acetate) as part of their normal treatment (Figure 2). Patients were then given a 15-minute adjustment period and were asked to move their arm to disperse the drug within the subacromial bursa. Following the adjustment period, patients were asked to repeat their arm elevation task following the same procedure as before. Immediately following the postinjection arm elevation task, patients were again asked to give their current shoulder pain level on an analog pain scale. Patients were blinded from their previous analog pain scale submission. For testing healthy subjects, the same kinematic evaluation was performed; however, no subacromial injections were given to the control group.

(A) Anesthetic subacromial injection with epinephrine and (B) anesthetic injection with corticosteroid.
Statistical Analysis
To determine whether there were differences in pain following treatment, a paired t test was used between pre- and postinjection visual analog scale pain scores. To determine the influence of treatment on scapular kinematics, three 2-way repeated-measures analyses of variance (ANOVAs) were used. Each rotation of the scapula, upward and internal rotation, and scapular tilt were treated as unique dependent variables. Humeral elevation angle at 4 increments (30°, 60°, 90°, and 120°) was treated as the first independent variable, and condition (preinjection, postinjection) was treated as the second independent variable. For significant interactions, pairwise comparisons were performed using the Fisher least significant difference test (LSD). To compare the effect of treatment with respect to healthy controls, three 2-way mixed effects ANOVAs were used. Humeral elevation angle at 4 increments was treated as the repeated-measures independent variable, and group (postinjection vs controls) was treated as the between-subjects factor. For significant interactions, pairwise comparisons were performed using the LSD. Because of the natural influence of humeral elevation on scapular kinematics, we did not perform post hoc testing for significant main effects of humeral elevation angle.
Results
Following the anesthetic subacromial injection, all patients reported verbally that their pain was reduced by at least a moderate amount. From our visual analog pain scales, patients reported a significant reduction in pain (mean, 65% reduction; P < .001), which marked a 35-point difference on average from pre- to postinjection.
For scapular tilt, there was a significant interaction between treatment and humeral elevation angle (P = .032). Post hoc pairwise comparisons indicated that treatment had no significant influence on scapular tilt at 30° and 60° of humeral elevation (P > .05). However, significant differences were detected for 90° (P = .04) and 120° (P = .007), with differences in anterior tilting of 2° and 3.5°, respectively. Comparing postinjection kinematics for patients with impingement versus healthy controls, a significant interaction between humeral elevation angle and group (controls vs impingement population) was detected (P = .006). Post hoc pairwise comparisons indicate that no significant differences were found between groups at 90° of humeral elevation (P > .05); however, significant differences were detected at 120° of humeral elevation, where the impingement group had on average 7.1° ± 2.9° greater anterior tilting than controls (P = .02) (Figure 3).

Anterior tilting angle during arm elevation preanesthetic (red) and postanesthetic (blue) injection versus healthy controls (green). #Significant difference for between-subject comparisons; *significant difference for within-subject comparisons.
For the influence of treatment and humeral elevation on scapular upward rotation, no significant interactions were detected (P = .93). No significant main effect was detected for treatment (P = .17). When comparing postinjection upward rotation to control subjects, a significant interaction between humeral angle and group (controls vs impingement population) was detected (P < .001). Post hoc pairwise comparisons indicate that no significant differences were pronounced between groups at 30° or at 120° (P > .05). However, at 60° of humeral elevation, the impingement group had on average 5.1° ± 1.9° greater upward rotation than controls (P = .013). At 90° of humeral elevation, the impingement group had on average 7.1° ± 1.8° greater upward rotation than controls (P = .001) (Figure 4).
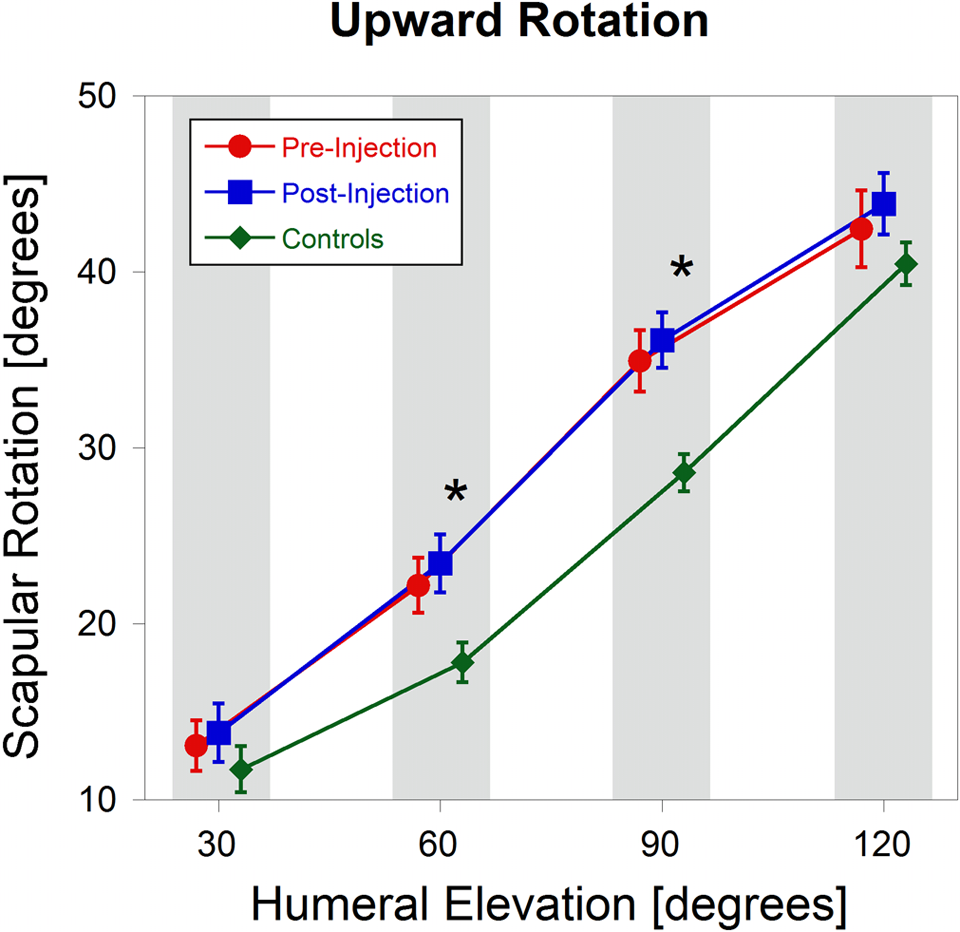
Upward rotation angle during arm elevation preanesthetic (red) and postanesthetic (blue) injection versus healthy controls (green). *Significant difference for between-subject comparisons.
For scapular internal rotation, no significant interactions between treatment and humeral elevation were detected (P = .629). No significant main effects of treatment (P = .167) or humeral elevation (P = .977) were detected. When compared with healthy controls, no significant interactions were detected (P = .974) (Figure 5).

External rotation angle during arm elevation preanesthetic (red) and postanesthetic (blue) injection versus healthy controls (green). #Significant difference for within-subject comparisons; *significant difference for between-subject comparisons.
Discussion
We hypothesized that the reduction of pain in patients with stage 2 impingement would result in decreased scapular anterior tilt and increased upward rotation and would result in no changes in scapular internal rotation during elevation of the arm. Additionally, we hypothesized that kinematics following the injection would be more representative of the kinematics of healthy control subjects. For anterior tilting, our results did not support the hypothesis. Following the injections, patients demonstrated a 2° increase in anterior tilting at 90° of humeral elevation and a 3.5° increase in anterior tilt at 120° of elevation (see Figure 3). When compared with healthy controls, patients postinjection had 7.1° greater anterior tilting at 120° of arm elevation (see Figure 3). For upward rotation, our results did not support our hypothesis. No kinematic changes were detected following the injections; however, when compared with healthy controls, patients postinjection had 5.1° greater upward rotation at 60° and 7.1° greater upward rotation at 90° of arm elevation (see Figure 4). For scapular internal rotation, our hypothesis was supported, since no significant changes were noted following the subacromial injection or when compared with healthy controls (Figure 5).
In studies examining differences in scapular kinematics versus healthy controls, most studies agree that patients with subacromial impingement have greater scapular anterior tilt than healthy control subjects. 11,17,20,21,23 Our findings agree with the literature, especially at arm elevation angles of 90° and 120°. Previous reports indicate that the acromiohumeral distance is minimized as the arm approaches greater arm elevation angles. 7,14 In healthy individuals, scapular kinematics tend toward less anteriorly tilted scapular positions at greater elevation angles, presumably to provide a greater acromiohumeral clearance. 21 Healthy control subjects in our study tended toward a less anteriorly tilted scapula at greater elevation angles, which agrees with the literature. 22,37 The anterior acromion is the predominant site of impingement, where acromial shape and orientation can greatly influence degeneration of subacromial tissues. 4,28 It has been postulated that the contact pressure beneath the acromion is associated with diffuse anterior shoulder pain. 4,28,32,39 Following the reduction in pain using an anesthetic subacromial injection, our results indicate an increase in anterior scapular displacement, which may further reduce the acromiohumeral distance. 21 Furthermore, the differences in scapular tilt following treatment were most prevalent at greater arm elevation angles, thus potentially exacerbating the effects of a reduced acromiohumeral distance. 7,14,34 Our results indicate that subacromial pain may be related to scapular tilt, especially at greater humeral angles (see Figure 3). However, it is possible that increased fluid in the subacromial bursa postinjection had an influence on scapular tilt, perhaps because of increased subacromial pressure.
For scapular upward rotation and patients with impingement syndrome, there is less agreement pertaining to trends in kinematics when compared with healthy controls. Several studies suggest that patients have decreased scapular upward rotation, 11,21 1 demonstrated increased upward rotation, 24 and several others found no differences. 17,23 Our findings suggest that when compared with healthy controls, patients demonstrate greater upward rotation, agreeing with 1 other study. 24 Our control participants demonstrated a linear increase in scapular upward rotation with arm elevation, which is consistent with the literature. 18,22,25,37 Following the subacromial injection, we found no significant changes in upward rotation (see Figure 4). This finding suggests that pain reduction via an anesthetic injection may not have an influence on scapular upward rotation in patients with subacromial impingement. In patients with rotator cuff tears, subacromial injections have been shown to decrease scapulothoracic motion and increase glenohumeral contribution toward arm elevation. 33 This may be related to an increase in humeral abduction strength following subacromial injections. 5,31 Our patients did not show evidence of rotator cuff tears; therefore, differences in our results and Scibek et al 33 could be related to other factors such as fatty infiltration of the cuff muscles, 6 differences in cuff tendon lengths, 12 and changes to the center of rotation of the glenohumeral joint due to superior translation of the humerus associated with rotator cuff tears. 9
Limitations
Our experimental design included a pre- and posttreatment measurement for patients with subacromial impingement; however, for practical reasons, no treatment condition was given to healthy control subjects. Therefore, from our study, it is impossible to determine whether the changes observed in scapular kinematics were due to changes in pain or some other influence of the subacromial anesthetic injection, such as increased fluid in the subacromial bursa. The subacromial injection added approximately 10 mL of fluid into the subacromial bursa. The additional fluid within the subacromial bursa could potentially influence scapular kinematics by changing subacromial contact pressure. Future studies could use a placebo injection to investigate the influence of adding fluid to the subacromial bursa. Additionally, the size of the subacromial bursa could be taken into account with respect to scapular kinematics in patients with impingement. Furthermore, we acknowledge that even experienced physicians may not inject the intended areas or diagnose subacromial impingement with 100% accuracy. Future studies could incorporate imaging for verification of injection location as well as validation of the stage 2 impingement diagnosis.
Conclusion
An anesthetic subacromial injection successfully reduces pain in patients with impingement. However, the subacromial injection may temporarily further exacerbate scapular abnormalities by increasing anterior tilt, specifically at arm elevation angles of 90° and 120°. Our findings suggest that pain may be related to kinematics of the scapula and could be important for reducing scapular tilt, especially at higher arm elevation angles in patients with impingement. Furthermore, it is possible that the subacromial injection did not correct the scapular dyskinesia because of some neuromuscular scapular stabilization deficit. It is likely that patients will need corrective physical therapy emphasizing scapular stabilization to improve their symptoms.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from the Eugene and Clarissa Evonuk Foundation for Graduate Studies.