
Abstract
Background:
When to allow an athlete to return to unrestricted sporting activity after anterior cruciate ligament (ACL) reconstruction remains controversial.
Purpose:
To report the results of functional performance testing reported in the literature for individuals at differing time points following ACL reconstruction and to examine differences between graft types.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review of Medline, Scopus, and Cochrane Central Register of Controlled Trials was performed using PRISMA guidelines. Inclusion criteria were English-language studies that examined any functional rehabilitation test from 6 months to 2 years following ACL reconstruction. All patient-, limb-, and knee-specific demographics were extracted from included investigations. All functional rehabilitation tests were analyzed and compared when applicable.
Results:
The search term returned a total of 890 potential studies, with 88 meeting inclusion and exclusion criteria. A total of 4927 patients were included, of which 66% were male. The mean patient age was 26.5 ± 3.4 years. The predominant graft choices for reconstruction were bone–patellar tendon–bone (BPTB) autograft (59.8%) and hamstring autograft (37.9%). The most commonly reported functional tests were the hop tests. The results of these functional tests, as reported in the Limb Symmetry Index (LSI), improved with increasing time, with nearly all results greater than 90% at 1 year following primary ACL reconstruction. At 6 months postoperatively, a number of isokinetic strength measurements failed to reach 80% LSI, most commonly isokinetic knee extension testing in both BPTB and hamstring autograft groups. The knee flexion strength deficit was significantly less in the BPTB autograft group as compared with those having hamstring autograft at 1 year postoperatively, while no significant differences were found in isokinetic extension strength between the 2 groups.
Conclusion:
Hop testing was the most commonly reported functional test following ACL reconstruction. Increases in performance on functional tests were predictably seen as time increased following surgery. Those with hamstring autografts may experience increased strength deficits with knee flexion versus those having BPTB autograft. These data provide information that may assist providers in determining timing of return to unrestricted sporting activity.
Anterior cruciate ligament (ACL) injuries are common in the young and athletically active population, with a reported incidence of 0.7 to 2.5 ACL tears per 1000 athletic-exposures. 78 It has been estimated that between 100,000 and 200,000 reconstructions are performed in the United States each year. 13,22 Reconstruction of the ACL using either bone–patellar tendon–bone (BPTB) autograft, 69 hamstring autograft, 97 or allograft tissue 25 has become standard for treatment in patients who have functional knee instability and a desire to return to cutting and pivoting sports. Clinical follow-up has shown a high rate of return to previous level of activity using modern arthroscopically assisted reconstruction techniques. 24,58,64,96
While the need for ACL reconstruction in athletically active individuals who desire a return to cutting and pivoting sports is generally accepted, there is a lack of consensus as to when an athlete may return to sport. In their review of 264 investigations, Barber-Westin and Noyes 9 reported that criterion for return to play was not reported in 40% of studies, with an additional 32% of investigations using only postoperative time. Only 13% of the studies utilized objective criteria for determining when an athlete may return to sport.
Deficits in neuromuscular control of the lower extremity are known to be a risk factor for secondary (retear) ACL injury and are therefore often used in assessing return-to-play readiness. 75,100 Quadriceps strength, in particular, has been associated with physical functioning of the leg following ACL reconstruction. 16,57 Additionally, some authors have evaluated the presence of neuromuscular impairment following ACL reconstruction and its association with secondary reinjury. 75 Hip and knee positions predicted a second injury, 75 emphasizing the importance of addressing these parameters during rehabilitation.
To assist with returning a patient to sports, many groups have developed rehabilitation protocols, each with their own methods and return-to-play criteria. 23,31,104 Areas of particular interest in determining return to play are functional tests (ie, hop testing), lower extremity isokinetic strength measurements, and movement and/or landing mechanics. Yabroudi and Irrgang 104 recently outlined a detailed rehabilitation protocol and allowed full-effort sprinting, cutting, and plyometric activities once the patient reached a quadriceps index of 85% and has successfully completed the early postoperative, strengthening, and neuromuscular control phases. Heckmann et al 31 defined return-to-play criteria through the use of a subjective evaluation, knee examination, and functional testing.
The goal of these rehabilitation programs is ultimately to allow return to play without additional injury to the knee. There has been no consensus as to which functional tests should be utilized to make this determination or what values should be achieved at different time points postoperatively. The goal of this investigation was to perform a systematic review of all available studies to provide normative data for functional tests utilized following primary ACL reconstruction to determine return to play. We also sought to detect any difference in the outcomes of functional testing between different graft types.
Methods
The first author performed a systematic review of multiple medical databases, including Medline and Scopus, using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 68 PRISMA guides authors in the appropriate design, conduct, and reporting of a systematic review and/or meta-analysis via appropriate identification, screening, and inclusion of relevant studies for review. The search term we usedi sought to find original research publications that investigated the results of functional testing following primary ACL reconstruction. Level 1, 2, 3, and 4 evidence clinical outcome studies were inclusive. Inclusion criteria were English-language studies that examined any lower extremity functional rehabilitation test from 6 months to 2 years following ACL reconstruction. This timeframe was chosen as the purpose of this investigation was to provide normative data for functional tests to help clinicians determine return to play criteria. This time frame captured data for patients who had undergone rehabilitation before returning to play at 6 months as well as those who had already returned to play and would presumably be maximally rehabilitated (2 years). Even if some patients had returned to play prior to the 6-month time point, their functional testing results would still provide adequate data from which to create normative data.
Exclusion criteria included studies reporting outcomes outside of the 6-month to 2-year postoperative timeframe, revision ACL reconstruction, non–English language, surgical technique, letters to the editor, systematic reviews, meta-analyses, duplicate subject populations, and multiligament knee injuries. Patients with concomitant ACL reconstruction with nonoperative treatment of a medial collateral ligament (MCL) injury were included, however. Studies that reported raw data or did not report results for single-leg testing as normalized data, such as through the use of the Limb Symmetry Index (LSI), were excluded even if results were compared with a healthy control subject. Exceptions to this included testing that required both legs, such as the shuttle run, in which case results were separately reported for males and females. When results were separately reported for 2 different cohorts within the same study, most commonly through the use of separate rehabilitation protocols, the results between groups for each time point were averaged.
Both electronically and print published articles were accepted for inclusion, while meeting abstracts and proceedings were excluded. All references from the studies returned using the search term were cross-referenced for potential inclusion if initially omitted from the search results. If 2 or more separate studies existed that reported on identical patient populations, they were both included as long as they reported functional testing results for different time points between 6 months and 2 years. Figure 1 shows the search algorithm used to generate the final cohort of included investigations.
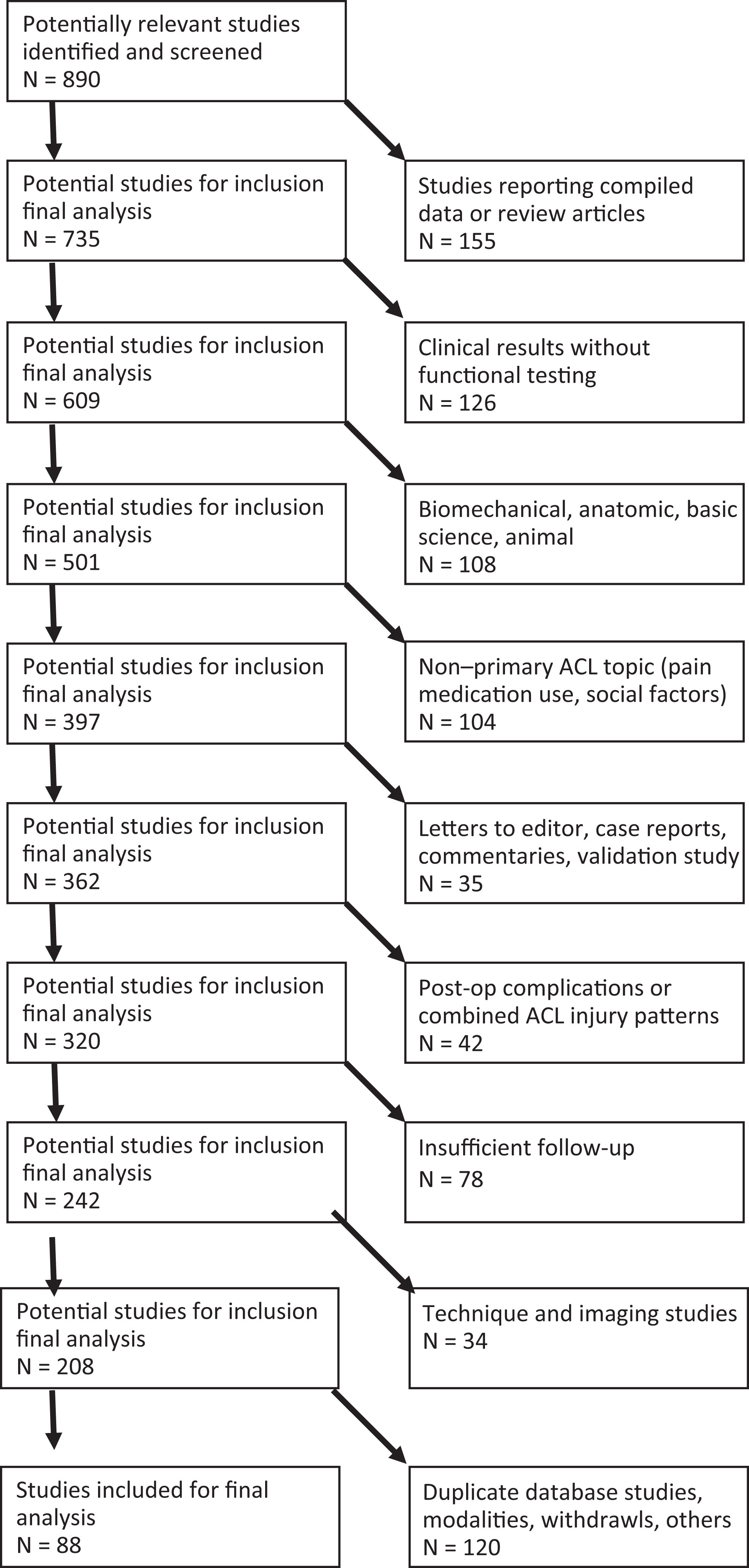
Systematic review search algorithm within Medline database according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Descriptive statistics were used, with results reported as means ± standard deviations. Categorical data were reported as frequencies with percentages. Where applicable, results were compared using the Student t test and linear regression with an alpha value of .05 set as significant.
Results
The search term returned a total of 890 potential studies, with 88 meeting inclusion and exclusion criteria (Figure 1). A total of 4927 patients were included, of which 66% were male. The mean patient age was 26.5 ± 3.4 years. The predominant graft choices for reconstruction were BPTB autograft (59.8%) and hamstring autograft (37.9%). BPTB allograft was used in 1.6% of patients, hamstring allograft in 0.1%, and quadriceps autograft in 0.4%.
The most commonly reported functional tests were the hop tests. These included the single-leg, cross-over, triple, 6-m timed, and single-leg hop height tests (Table 1). In general, the results of these functional tests, as reported in LSI, improved with increasing time, with nearly all results greater than 90% at 1 year after primary ACL reconstruction. For example, single-leg hop LSI averaged 87%, 92%, and 94% at 6 months, 1 year, and 2 years, respectively. When examining the results of the 5 most common hop tests (single-leg hop, cross-over hop, triple hop, 6-m timed hop, and single-leg hop height), there were no significant differences at any time points in the results between those receiving BPTB and hamstring autograft (P > .265).
Studies Reporting the Results of Functional Performance Tests Involving Hopping, Jumping, or Squatting at Varying Time Points After ACLR a
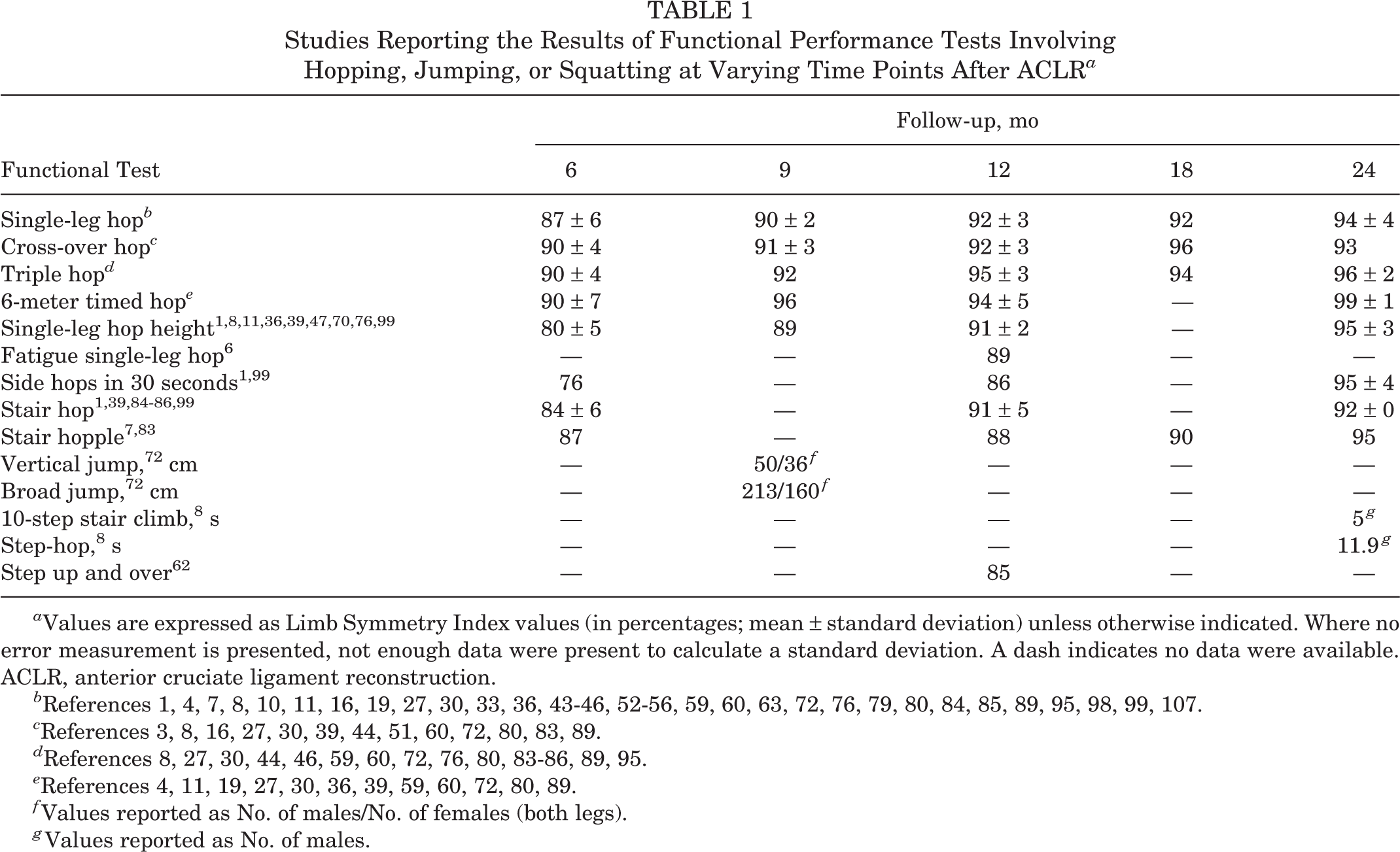
a Values are expressed as Limb Symmetry Index values (in percentages; mean ± standard deviation) unless otherwise indicated. Where no error measurement is presented, not enough data were present to calculate a standard deviation. A dash indicates no data were available. ACLR, anterior cruciate ligament reconstruction.
b References 1, 4, 7, 8, 10, 11, 16, 19, 27, 30, 33, 36, 43–46, 52–56, 59, 60, 63, 72, 76, 79, 80, 84, 85, 89, 95, 98, 99, 107.
f Values reported as No. of males/No. of females (both legs).
g Values reported as No. of males.
Table 2 reports the results of agility testing at varying time points following primary ACL reconstruction. There was no significant difference between times in the co-contraction, shuttle run, or carioca tests over the 6-month to 2-year time period (P > .240). The times for long shuttle, modified agility, and pro shuttle tests were lower for men than women (Table 2).
Studies Reporting the Results of Agility Testing at Varying Time Points After ACLR a
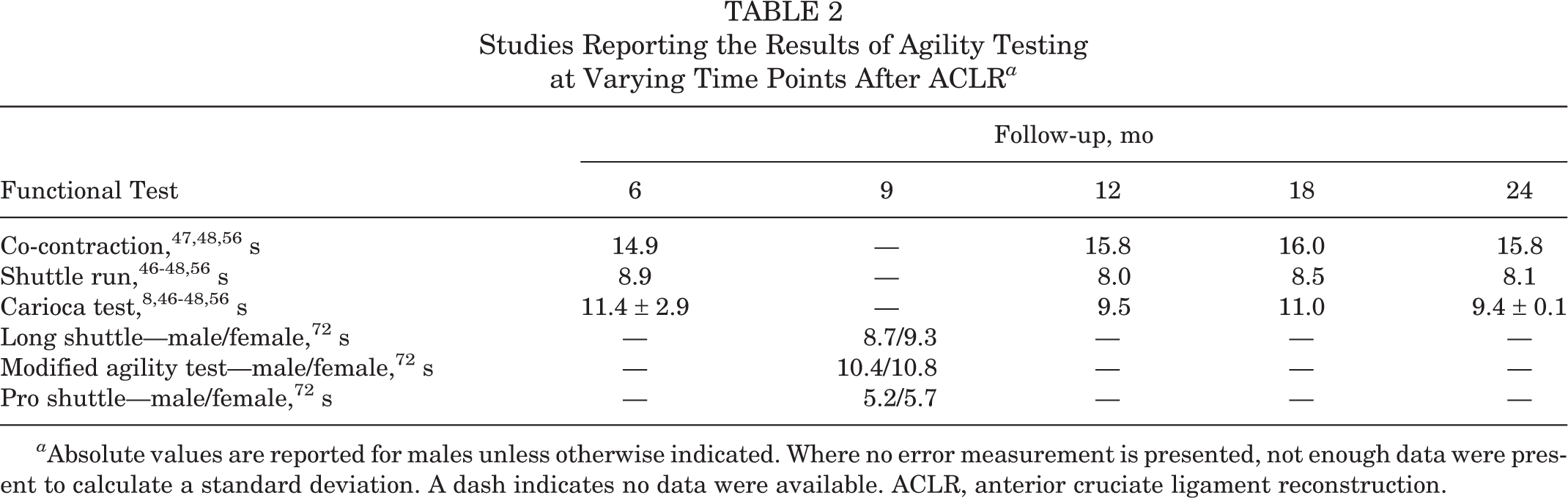
a Absolute values are reported for males unless otherwise indicated. Where no error measurement is presented, not enough data were present to calculate a standard deviation. A dash indicates no data were available. ACLR, anterior cruciate ligament reconstruction.
Results of functional performance tests utilizing a motion analysis with or without a force plate are presented in Table 3. One-leg hop contact time and jump time returned to an average of 98% and 84% LSI, respectively, at 1 year postoperatively. Ground reaction force (GRF) during landing and takeoff were 89% and 73%, respectively, at 8 months. Proprioception was also assessed in a number of investigations (Table 3). In general, postural motion control, reproduction of passive motion of the knee, and overall joint position sense returned to values similar to the contralateral limb from 8 to 12 months following ACL reconstruction.
Results of Functional Performance Tests Utilizing a Force Plate and/or Motion Analysis a
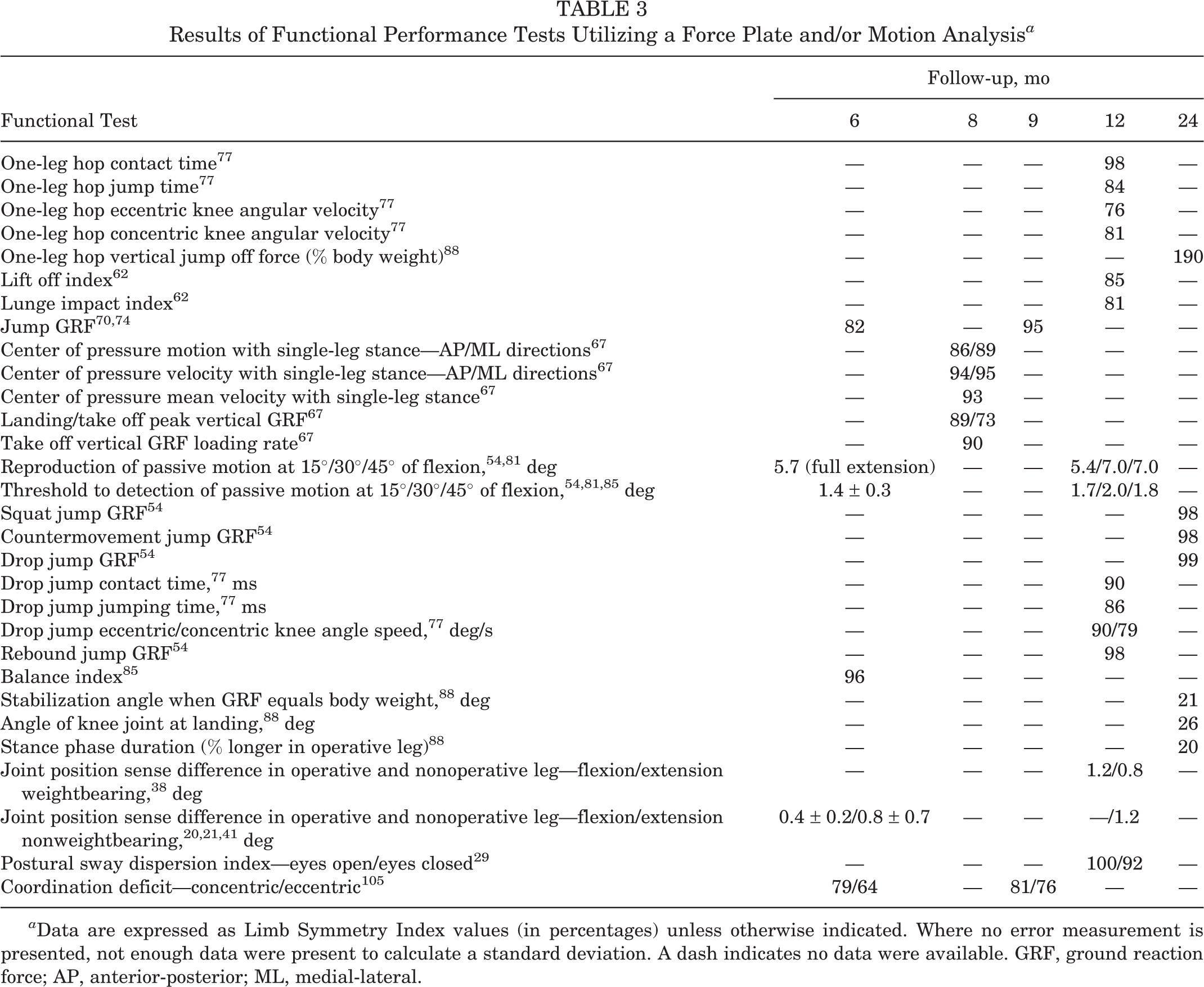
a Data are expressed as Limb Symmetry Index values (in percentages) unless otherwise indicated. Where no error measurement is presented, not enough data were present to calculate a standard deviation. A dash indicates no data were available. GRF, ground reaction force; AP, anterior-posterior; ML, medial-lateral.
Functional testing involving strength assessment following ACL reconstruction was also extensively reported in the literature and is summarized in Table 4. At 6 months postoperatively, a number of strength measures had failed to reach 80% LSI as compared with the uninvolved contralateral leg (Table 4). This was most common for isokinetic knee extension testing in both BPTB and hamstring autograft groups. In comparing all patients, there were significantly greater deficits in isokinetic knee extension values at various angular velocities and multiple time points postoperatively (Table 5). Significant differences were seen for isokinetic knee flexion showing less deficit (versus extension) as compared with the contralateral limb. When comparing the results of the groups by graft type, knee flexor strength deficit at 60 and 180 deg/s was significantly less in the BPTB autograft group (97% and 99%) as compared with those having hamstring autograft (87% and 91%) at 1 year postoperatively (P = .002 and .015). No significant differences were found in isokinetic extension strength between the 2 groups at any time point or at any angular velocity.
Studies Reporting the Results of Functional Performance Tests Involving Strength Testing at Varying Time Points After ACLR a

a All data are expressed as Limb Symmetry Index values (in percentages; mean ± standard deviation). Where no error measurement is presented, not enough data were present to calculate a standard deviation. A dash indicates no data were available. ACLR, anterior cruciate ligament reconstruction. MVIC, maximal voluntary isometric contraction; BPTB, bone–patellar tendon–bone.
P Values Comparing Isokinetic Peak Knee Flexion and Extension Forces at Varying Time Points and Angular Velocities a

a All significant values (P < .05, Student t test) represent increased strength in knee extension versus knee flexion. A dash indicates no data were available.
Discussion
The goal of this investigation was to provide normative data to assist both patients and physicians in determining return to play following ACL reconstruction. A secondary goal was to assess any subtle differences in the performance results of patients with differing graft types. Even with the large amount of published investigations regarding all aspects of ACL reconstruction, as well as functional testing following ACL reconstruction, few clinicians utilize objective data in determining return to play, and there is no evidence-based consensus on when it is appropriate for patients to return to unrestricted sports participation. A recent systematic review by Barber-Westin and Noyes 9 examined 264 studies within the past 10 years describing return to play following primary ACL reconstruction. Of these included investigations, only 13% described objective criteria for return to play. Forty percent gave no criteria, 32% used only time from surgery, and 15% utilized time from surgery along with subjective functional assessment scores.
In this review, the most common functional tests reported in the literature following ACL reconstruction were the hop tests. The 4 standard hop tests (single-leg, cross-over, triple, and 6-m timed hop tests) all averaged greater than 90% LSI at 6 to 9 months postoperatively. Interestingly, when more demanding testing was carried out that required increased stamina in the operative leg, results declined. Although the number of studies reporting results of endurance hop tests is limited, the findings presented in this investigation demonstrated that the results of the fatigue single-leg hop and side hop in 30 seconds showed lower LSI values as compared with the standard hop testing regimen. This may indicate increased fatigability in the operative extremity that is still present at the 6- to 12-month time period. These deficiencies, however, appeared to normalize by the 24-month mark, with LSI values in the mid-90% range, comparable to the other hop testing results.
While an important objective measure, the results of hop testing have not been correlated with return to play. They have, however, been correlated with knee function as measured with self-reported questionnaires. Logerstedt et al 60 examined the correlation between hop testing and the International Knee Documentation Committee 2000 subjective knee form (IKDC 2000) at 6 and 12 months after primary ACL reconstruction. To define “normal” knee function, they utilized published normative data for the top 85th percentile of age- and sex-matched control knees. While preoperative hop testing was not predictive of knee function at any time following ACL reconstruction, postoperative testing was predictive of self-reported knee function. Of the 4 common hop tests examined, the 6-m timed and cross-over hop tests were the best predictors of normal subjective knee function as measured by IKDC 2000. With a sensitivity of 88%, the cross-over hop test most accurately identified those with normal function. This is likely because of the fact that of all the tests, the cross-over hop is the most functionally demanding as it requires coordination and strength in the frontal, sagittal, and coronal planes. Near normal values in this test indicate improved neuromuscular control of the leg.
At 1 year, those with normal knee function had median LSI values of 93% for the single-leg, cross-over, and triple hop tests, while the median value was 96% for the 6-m timed hop. Reinke et al 82 performed a similar investigation with a smaller cohort of patients and found that the triple hop test best correlated with the IKDC score as well as certain subsets of the Knee Injury and Osteoarthritis Outcomes Score (KOOS).
Another common functional test reported in the literature is knee flexion and extension strength testing. In examining the results presented in Table 4, 6 months following ACL reconstruction, mean LSI values for isokinetic knee flexion were in the range of 80% to 90%, with correction to near normal values by 1 year. This trend was not seen in the results for isokinetic knee extension, with values commonly in the 70% range at 6 months and remaining below 90% in almost all categories at the 1-year mark postoperatively. These observations are supported by the data presented in Table 5, with significant knee extension deficits (compared with knee flexion LSI) at a number of time points postoperatively. These results compare with other investigations that have looked at isokinetic strength between BPTB and hamstring autograft reconstruction techniques. Wipfler et al 102 reported isokinetic knee flexion to be 99% and 91% in the BPTB and hamstring autograft groups at 1-year follow-up, while extension was 87% and 92%, respectively. Aglietti et al 2 also reported significantly increased isokinetic extension strength deficits at 1 year follow-up for BPTB versus hamstring autograft patients without concomitant decreased flexion strength in the hamstring graft group.
While the results of functional testing have not been shown to predict return to sport, Hewett et al 35 proposed that strength training with correction of faulty movement biomechanics and balance training are the most effective methods for preventing ACL injuries. Many of these factors can be tested using the motion analysis and force plate data described in Table 3. The effectiveness of these programs in the prevention of initial ACL injury as well as other lower extremity injuries has been demonstrated. 49,61,94,101 Mandelbaum et al 61 investigated whether the use of a neuromuscular and proprioceptive performance program was effective at decreasing the incidence of ACL injury in an elite population of female soccer players. In their cohort study, they found that the program decreased the incidence of ACL injury by 88% and 74% in years 1 and 2, respectively, after initiation of the program.
While normative values as well as values that correlate with perceived “normal” knee function can be provided for functional testing following ACL reconstruction, objective evidence is lacking for determining return to play criteria based on an exact result of a functional test. Many authors have advocated using multiple tests to determine full return to play status. 60,82 Barber-Westin and Noyes 9 report that their protocol includes a less than 10% deficit in strength of the quadriceps and hamstring on isokinetic testing at 180 deg/s; less than 15% deficit in lower limb symmetry for single-hop, triple hop, cross-over hop, and timed hop; greater than 60% normalized knee separation distance on a video drop-jump test; as well as a normal physical examination. For even beginning a return-to-sport rehabilitation regimen, Myer et al 71 recommend a minimum IKDC score of 70, no postsurgical history of giving way or a negative pivot shift, and a minimum baseline strength knee extension peak torque/body mass of 40% and 30% at 300 deg/s and 60% and 50% at 180 deg/s for males and females, respectively. The last stage the athlete must pass before slow reintegration into full athletic activity includes drop vertical jump landing force within 15% LSI, modified agility test (MAT) time within 10%, single limb average peak power test for 10 seconds within 15%, and a perfect score on the tuck jump or improvement of 20 percentage points from the initial score. 71
Limitations of this investigation are based in the weaknesses of the studies included. One potential is that the time frame for functional testing was slightly different than that reported. For example, testing of a patient at 5 or 7 months following surgery, versus at the 6-month time point, may slightly affect results because of the increased or decreased time that the patient has had for rehabilitation. It is possible that some studies reporting on functional testing following ACL reconstruction that met our inclusion and exclusion criteria were not captured. This is minimized, however, with the use of 3 separate databases and cross-referencing of reference sections for investigations that the search algorithm may have missed.
Conclusion
This investigation provides data on all published functional testing following primary ACL reconstruction. The most commonly reported tests were the hop tests as well as isokinetic knee flexion and extension strength. Knee extension strength lagged behind that of knee flexion strength in all graft types, underlining the importance of quadriceps rehabilitation postoperatively. Those with hamstring autografts were found to have decreased isokinetic knee flexion strength versus BPTB autograft patients, while there were no differences in isokinetic knee extension strength between groups at any time point. The values summarized in this investigation should serve as guidance to aid in decision-making when deciding when to return the athlete to unrestricted play following ACL reconstruction.
Footnotes
One or more of the authors declared the following potential conflict of interest or source of funding: C.A.B. is an unpaid consultant for The Foundry and is on the editorial board of the American Journal of Sports Medicine. N.N.V. receives royalties from Smith & Nephew; is a paid speaker for Arthrosurface; is a consultant for Smith & Nephew and Arthrex; owns stock options in Omeros; receives research support from Arthrex, Smith & Nephew, Athletico, ConMed Linvatec, Miomed, Mitek, and Arthrosurface; receives royalties/publisher support from Vindico Medical-Orthopedics Hyperguide and Arthroscopy; and is a board member of the Journal of Knee Surgery, Arthroscopy, SLACK Inc, and the Arthroscopy Association Learning Center committee. B.J.C. is a board member of the Arthroscopy Association of North America; is a consultant for Genzyme, Arthrex, Zimmer, Carticept, Regentis, DJO, and Johnson & Johnson; receives research support from Major League Baseball, MTF, OREF, NIH/MIMAS, Arthrex, Zimmer, Arthrosurface, Medipost, and Johnson & Johnson; and receives royalties from Arthrex and DJO. B.R.B. receives research support from Arthrex, ConMed Linvatec, DJ Orthopaedics, Ossur, Smith & Nephew, and Tornier; receives publisher compensation from SLACK Inc; and is a board member of the American Orthopaedic Society for Sports Medicine and Orthopaedics Today.