
Abstract
Background:
Prior studies have attempted to determine morphological characteristics of the medial epicondyle in overhead athletes, but no study has reported on precise quantitative differences between elite overhead athletes and control patients.
Hypothesis:
The medial epicondyle in overhead athletes is larger in volume than those of control patients.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Computer simulation modeling from advanced (computed tomography/magnetic resonance imaging) imaging of the elbow of 37 patients (22 elite overhead athletes, 15 control patients) was performed to provide detailed assessment of the morphological characteristics of the medial epicondyle. Several quantitative metrics regarding the medial epicondyle were measured and compared across both cohorts, including that of epicondyle width (medial-lateral), height (superior-inferior), thickness (anterior-posterior), volume, percentage cortical volume, and morphology of the inferior slope of the epicondyle.
Results:
The medial epicondyle in overhead athletes was significantly larger than that found in nonathlete controls (4976 vs 3682 mm3; P = .001). There was no significance between the 2 cohorts in medial-lateral width (16.8 vs 16.6 mm; P = .68), but there was a difference in anterior-posterior thickness (16.96 vs 14.40 mm; P = .001) and superior-inferior height (39.55 vs 35.86 mm; P = .09) in athletes versus controls. The epicondyle volume was 97.9% cortical bone in athletes compared with 82.3% in control patients (P < .001). There were no differences in the morphology of the inferior epicondyle slope between the 2 groups.
Conclusion:
The medial epicondyle in overhead athletes is larger in volume and anterior-posterior thickness than those of control patients. Additionally, the medial epicondyle is comprised nearly entirely of cortical bone in overhead athletes.
Clinical Relevance:
These quantitative findings support the theory of adaptive remodeling in skeletally immature overhead athletes.
The overhead athlete exposes his or her elbow to extremes of stress and motion during throwing. These stresses predispose this patient population to unique injuries at this joint, 7,8 such as rupture of the ulnar collateral ligament, olecranon stress fracture, posteromedial impingement, and even fracture of the medial epicondyle in youth athletes. Many of these injuries may be due to “overuse” or fatigue, and those requiring surgery often concomitantly require extensive periods of rehabilitation. Moreover, these injuries have been increasing in frequency in younger, adolescent athletes. As such, increased attention has been given toward better understanding these injuries in an attempt to optimize treatment and management techniques. One area demanding increased focus is the underlying anatomy at the medial aspect of the elbow.
In 1965, Adams 1 reported on various radiographic findings appearing in the pitching arms of youth baseball players aged 9 to 14 years. In his study, he reported changes to the medial epicondyle appearing in an overwhelming majority of pitchers in this age group. These findings included accelerated growth and epiphyseal separation of the medial epicondyle along with fragmentation of the physis. Several follow-up studies have attempted to further clarify the morphological differences of the medial elbow in overhead athletes using a variety of modalities, such as plain radiographs and magnetic resonance imaging (MRI) scans. Gugenheim et al 4 studied the radiographs from nearly 600 Little League baseball players and noted that virtually all players demonstrated hypertrophy of the medial epicondyle in the dominant arm, either of the cortex or the trabeculae. They concluded that these findings were not related to symptomatic elbow pain or disability, however. Several authors have used MRI imaging as well. Wei et al 11 reported increased medial epicondyle size on radiographs along with apophyseal widening and separation noted on MRI in symptomatic Little League players, and Hurd et al 6 reported the presence of asymmetric thickening of the anterior band of the ulnar collateral ligament in the dominant arms of asymptomatic high school pitchers without symptomatic implication.
Despite these efforts, much remains unknown regarding the precise, quantitative anatomic differences in the medial elbow between overhead athletes and control counterparts. Clear delineation of these anatomic differences can be invaluable in confirming the presence of adaptive remodeling of the bony structure of the medial epicondyle as a reaction to increased stress from repetitive overhead activities. Variations in morphology of the medial epicondyle between individuals can also contribute to the understanding of optimal surgical planning (ie, tunnel placement and depth) in ulnar collateral ligament reconstruction. The purpose of this study was to quantitatively compare the medial epicondyle between male overhead athletes and control patients, using 3-dimensional (3D) reconstructions of advanced imaging (computed tomography [CT] and MRI scans), to determine if any difference existed in these 2 patient groups. Moreover, we hypothesized that the medial epicondyle in overhead athletes would be larger in volume than those of non–overhead athletes.
Materials and Methods
Image Collection and Rendering
After institutional review board approval was obtained from our institution (protocol IRB-AAAJ1451), 50 consecutive patients presenting with a chief complaint of elbow pain who also had advanced imaging of the elbow (either MRI or CT scan) were considered for this study. Twenty-five patients were considered to be “elite overhead athletes,” indicating that they competed at the collegiate, semiprofessional, or professional level. The remaining cohort of 25 patients were not considered to be overhead athletes and defined to be “control” patients. Inclusion criteria further included patients who had reached skeletal maturity and whose dominant extremity was affected. Those with prior history of trauma affecting the medial epicondyle, who had not reached skeletal maturity, who were female, or whose nondominant limb was affected were excluded from the study. These exclusion criteria were designed to minimize variability in anatomy due to sex and age. Moreover, those whose elbow imaging was either of poor quality or without adequate visualization of the distal humerus included were also excluded. At study commencement, there were 22 overhead athletes and 15 control patients who met all inclusion and exclusion criteria.
These CT scans and MRIs were converted into patient-specific 3D computer models of the elbow using the Materialise Interactive Medical Image Control System software (Mimics; Materialise, Ann Arbor, Michigan, USA). The use of this software to produce anatomically accurate models has been previously verified in a shoulder model 2 and similarly utilized in elbow models of overhead athletes. 3 These elbow models were then uploaded into Materialise rapid prototyping software (Magics; Materialise), where they could be manipulated for measurement of the medial epicondyle.
Measurements Involving the Medial Epicondyle
Using the software’s ability to create user-defined coordinate systems, a humeral Cartesian coordinate system was defined with anatomic landmarks as reference points to standardize the position of each model 10 (Figure 1). The x-axis was defined by the transepidcondylar axis of the humerus, and the y-axis was defined as the longitudinal axis of the humeral shaft for each elbow model. The z-axis was then created as the line perpendicular to both the x- and y-axes to create a 3D coordinate system. This Cartesian coordinate system allowed for manipulation of the models in a standardized fashion, maintaining the exact positions of the humerus. The medial epicondyle was then defined in the coronal x-y plane of each model. A cut was made from the medial-most edge of the trochlea superiorly, parallel to the shaft of the humerus, until it separated the medial epicondyle from the remainder of the humerus, thus defining the borders of the medial epicondyle (Figure 2).
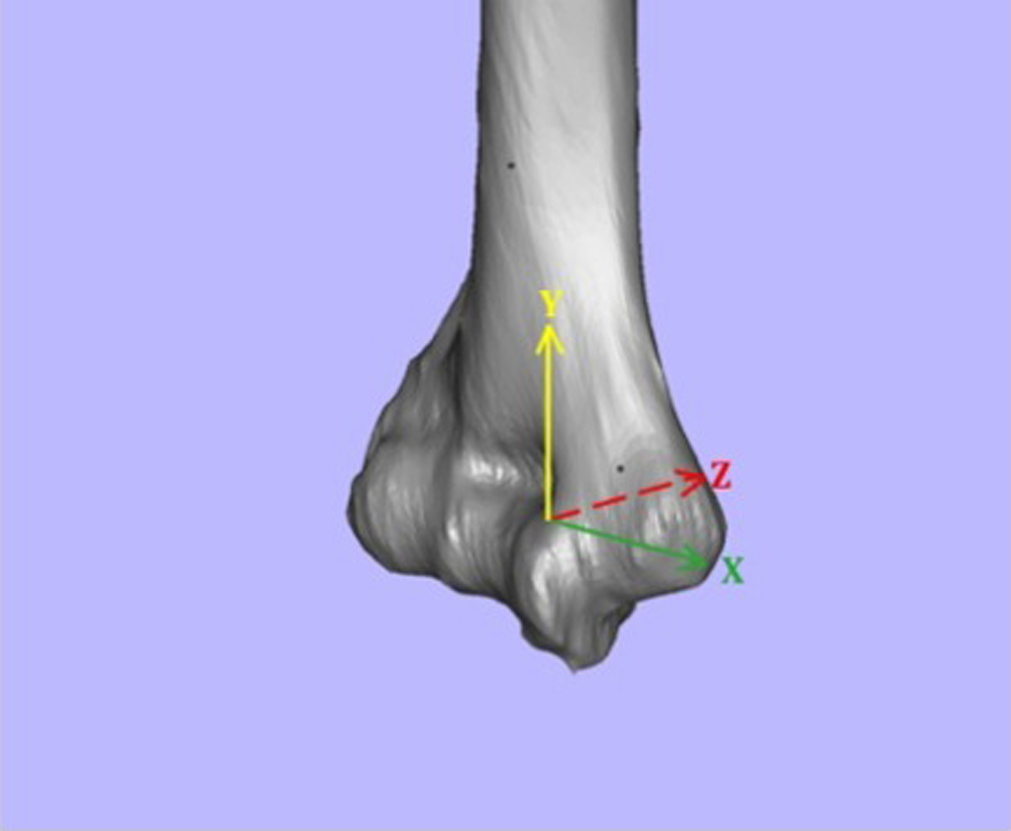
Distal humeral Cartesian coordinate system. The x-axis was defined by the transepidcondylar axis of the humerus, and the y-axis was defined as the longitudinal axis of the humeral shaft for each elbow model. The z-axis was then created as the line perpendicular to both the x- and y-axes to create a 3-dimensional coordinate system.

Anatomic definition of the medial epicondyle. A cut was made from the medial-most edge of the trochlea superiorly, parallel to the shaft of the humerus, until it separated the medial epicondyle from the remainder of the humerus, thus defining the borders of the medial epicondyle.
Measurements of the medial epicondyle included medial-lateral width along the x-axis, superior-inferior height along the y-axis, and anterior-posterior thickness along the z-axis (Figure 3). The volume of the separated medial epicondyle was also measured using the software’s ability to calculate volume. The angle at which the medial epicondyle extrudes from the humerus was termed the “extrusion angle” and was measured in the coronal (x-y) plane. The extrusion angle was defined as the angle formed between the vertical line that separates the medial epicondyle from the humerus and the line connecting the superior-most point of the medial epicondyle to the medial-most point of the medial epicondyle (Figure 4). Finally, the morphology of the medial epicondyle—with respect to the slope of the inferior aspect—was assessed. This region of the epicondyle corresponds to the site of tunnel drilling during reconstruction of the ulnar collateral ligament. Three morphology types were defined, including “mostly flat” (type A), “gently superiorly sloped” (type B), and “sharply sloped” (type C) (Figure 5).

Linear measurements of the medial epicondyle. The medial epicondyle dimensions were measured with regard to (A) medial-lateral width (ML) and superior-inferior height (SI) and (B) anterior-posterior thickness (AP).

Extrusion angle of the medial epicondyle. The extrusion angle of the medial epicondyle was defined as the angle formed by the vertical line extending superiorly from the intersection of the medial aspect of the trochlea and the inferior aspect of the epicondyle at the distal humerus cortex along with a line originating from this point on the distal humerus extending to the most medial aspect of the medial epicondyle.
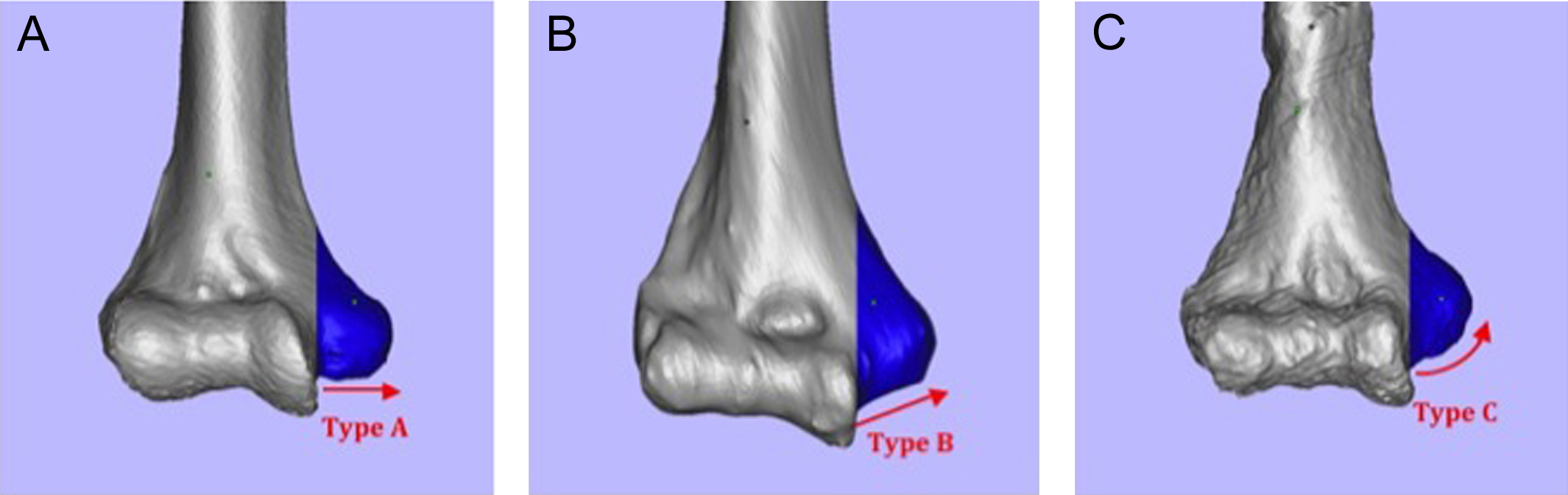
Inferior morphology of the medial epicondyle. Three morphology types were defined with respect to the inferior aspect of the medial epicondyle: (A) type A, or mostly flat; (B) type B, or gently sloping; and (C) type C, or sharply sloping.
The portion of the medial epicondyle volume that was comprised of cortical bone (as opposed to trabecular bone) was measured by creating 3D models of the medial epicondyle for a small subset of patients with CT imaging that showed adequate detail to differentiate cortical from trabecular bone. There were 9 throwing athletes and 4 controls in this subset. By setting the Hounsfeld unit threshold to 300, as described by Schreiber et al, 9 only cortical bone voxels were included in the models. The medial epicondyle's fractional volume was obtained by dividing the volume of this cortical model of the medial epicondyle by the total volume (cortical + trabecular) of the medial epicondyle (Figure 6). The medial epicondyle volume that was derived from cortical bone was compared between overhead athletes and control patients.

Cortical fraction of the medial epicondyle. (A) A 3-dimensional model was created that only included cortical bone. (B) The cortical fraction was defined as the volume of this cortical model divided by the volume of the total medial epicondyle.
Statistical Considerations
For all dimensional categories, measurements were made blind to classification of patient (overhead athlete vs control patient). Interobserver reliability was calculated according to these sets of measurements. A random sampling of 20 total subjects was selected for repeat measurement 2 weeks after initial measurement to provide intraobserver reliability calculations. Interclass correlation coefficients (ICCs) were determined for each measurement comparing the 2 different observers (E.C.M. and K.K.) and the 2 different measurements by the same observer. The subjective measurements of the inferior aspect of the medial epicondyle were used to determine a Cohen kappa coefficient. Comparisons between the medial epicondyle morphology of throwers and nonthrowers were made using chi-square statistical testing. Statistical significance was set at P < .05 for all comparisons. For P < .10, a statistical trend was denoted. Since no prior studies exist comparing these medial epicondyle dimensions, no power analysis was performed.
Results
A total of 50 patients were considered for evaluation; 4 were excluded because of involvement of the nondominant arm, 4 were excluded because they were female, and 5 additional patients were excluded because of poor quality imaging. Of the final 37 patients, 22 were overhead athletes and 15 were control patients. The demographic characteristics of these patients can be found in Table 1. The overhead athletes were younger than their control counterparts and were virtually all baseball players. Among these athletes, the most common position played was pitcher, and the most common chief complaint was related to injury of the medial collateral ligament. Among control patients, common complaints included epicondylitis and trauma.
Patient Demographic Data a

a MCL, medial collateral ligament; N/A, not applicable; SD, standard deviation.
The volume of the medial epicondyle in overhead athletes was significantly larger than that of control subjects (4976 mm3 [range, 2089-7975 mm3] vs 3682 mm3 [range, 1982-5064 mm3]; P = .001) (Figure 7). When considering individual dimensions (Figure 8), there was no significant difference in medial-lateral width of the epicondyle (16.8 mm in overhead athletes [range,12.2-20.2 mm] vs 16.6 mm in controls [range, 12.3-19.2 mm]; P = .68). However, there was a significant difference in thickness in the anterior-posterior plane of the epicondyle (16.96 mm in overhead athletes [range, 14.4-19.9 mm] vs 14.40 mm in controls [range, 10.6-19.4 mm]; P = .001). Moreover, we found a trend toward increasing medial epicondyle height (superior-inferior) in these athletes (39.55 mm [range, 29.4-53.1 mm] vs 35.86 mm [range, 27.6-48.6 mm]; P = .09).

Medial epicondyle volume. The volume of the medial epicondyle in overhead athletes (throwers) was significantly larger (by a factor of 1.35, P = .001) compared with control patients.

Medial epicondyle dimensions. Compared with control patients, the medial epicondyle of overhead athletes (throwers) had greater anterior-posterior thickness (P = .001). There was a statistical trend toward increased height in the superior-inferior direction (P = .09) and a resultant decrease in extrusion angle (P = .06).
Additional measurements included that of extrusion angle and overall epicondyle morphology. In the overhead athlete cohort, the extrusion angle showed a trend toward a lower extrusion angle compared with the control group (33.8° [range, 24.8°-42.9°] vs 37.0° [range, 33.5°-47.5°]; P = .06) (Figure 8). With regard to morphology, of the 22 overhead athletes, 5 (23%) had a type A morphology (eg, relatively flat inferior aspect of the epicondyle), 13 (59%) had a type B morphology (eg, gently superiorly sloping), and the remaining 4 (18%) patients had a type C (eg, sharply sloping) morphology. In control subjects, there were 7 type A patients (47%), 5 type B patients (33%), and 3 type C patients (20%). This was not statistically significant (P = .25) (Table 2).
Inferior Slope Morphology of the Medial Epicondyle a

a There were no significant differences found between the inferior slope characteristics of the medial epicondyle between overhead athletes and control patients (P = .25).
The final morphological calculation was that of medial epicondyle volume derived from cortical bone. In the subset of overhead athletes whose imaging allowed such calculation (n = 9), the medial epicondyle volume was 97.9% cortical bone, and the remaining 2.1% was trabecular bone. In control patients (n = 4), however, we found a cortical contribution of only 82.3% toward overall medial epicondyle volume, with the remaining 17.7% contributed by trabecular bone. This difference in cortical volume contribution was statistically significant (P < .001) (Figure 9).

Medial epicondyle cortical fraction. The cortical fraction of the medial epicondyle in overhead athletes (throwers) was significantly greater (by 15%) compared with control patients.
Finally, inter- and intraobserver reliabilities were calculated. Interobserver reliability was determined to be excellent when considering measurements of medial-lateral width, superior-inferior height, and extrusion angle (ICC: 0.98, 0.99, and 0.97, respectively). Interobserver reliability was moderately good when considering anterior-posterior epicondyle thickness (ICC, 0.74). These findings were similarly true for intraobserver reliability. When considering width, height, and extrusion angle, the ICCs for intraobserver reliability were 0.99, 0.99, and 0.96, respectively. Intraobserver reliability was slightly improved for thickness (ICC, 0.82).
Discussion
This is the first study, to our knowledge, to use 3D computer simulation to compare the morphology of the medial epicondyle in overhead athletes and control patients, assessing a variety of anatomic parameters. This study incorporated 37 patients, and we found that the medial epicondyle in overhead athletes was significantly larger in volume compared with control patients, likely because of an increase in thickness (anterior-posterior), along with a smaller contribution from increased height (superior-inferior). Moreover, epicondyles in overhead athletes displayed, in general, a trend toward more narrow excursions from the humerus. Finally, we found that the medial epicondyles in overhead athletes were composed nearly entirely (>97%) of cortical bone, whereas this structure was only 82% cortical bone in control patients. Our cohort of overhead athletes comprised generally elite-level baseball players (mostly pitchers), while our control patients were those who presented for evaluation of elbow trauma that did not include the medial structures of the elbow.
The findings from this study appear to lend support to the theory of medial epicondyle remodeling in developing overhead athletes. As the volume of this structure was significantly higher in these athletes, it is reasonable to postulate that repeated stresses appear to result in hypertrophy of the epicondyle. This is further supported by composition of the medial epicondyle itself, as it was composed almost entirely of cortical bone in the athletes. Additionally, there was a trend toward “taller” epicondyles (in the superior-inferior direction) along with a more acute extrusion of the epicondyle when compared with control patients. While these findings may have approached higher statistical significance if the sample size was higher, it does suggest that the epicondyle is subject to repetitive traction over time in these athletes, resulting in this alteration in morphology.
Alterations in medial epicondyle morphology and composition may have profound impacts on the delicate and precise relationships between the osseous and the ligamentous structures of the medial aspect of the elbow in the overhead athlete. The ulnar collateral ligament, originating at the medial epicondyle and inserting on the sublime tubercle of the proximal ulna, is crucial in resisting valgus stress during the overhead motion. Any alteration of the morphology of the medial epicondyle may affect the tension of the ligament during maximal exertion, particularly during the late cocking and early acceleration phases of the throwing motion, when the valgus forces at the medial elbow are at their maximum. In this computer simulation, the medial epicondyle was found to be larger in overhead athletes by a factor of 1.35 compared with control patients. It is unclear what ramification a larger size or narrower excursion of the epicondyle may have on injury risk. Moreover, it is unclear why the morphology of the medial epicondyle increased preferentially in the anterior-posterior direction, along with evidence of possible superior-inferior lengthening as well, as compared with hypertrophy and increase in all 3 dimensions equally. The morphologic type of the medial epicondyle should be appreciated prior to ulnar collateral ligament reconstruction to provide optimal location of tunnels.
Prior studies have reported the increased size of the medial epicondyle in the dominant elbow of overhead athletes (compared with the nondominant side). Wei et al 11 noted hypertrophy of the dominant medial epicondylar apophysis or medial humeral cortex in 2 of 9 patients diagnosed with Little Leaguer’s elbow, while Gugenheim et al 4 noted this finding in 95% of 600 Little League pitchers. Hang et al 5 also noted hypertrophy of the medial epicondyle in nearly all 343 Little League players in their study. However, the presence of this radiographic finding, especially related to the presence of elbow symptoms, is still unclear. Moreover, these studies reported on qualitative differences in epicondyle size. While our study did use 2 separate cohorts of patients (as opposed to the nondominant arm in comparison studies), we were able to make quantitative assessments of the medial epicondyle through computer simulation of the patients’ advanced imaging. Additionally, our computer simulation allowed for additional comparisons between the 2 patient cohorts, including those of width, height, and thickness of the epicondyle, as well as extrusion angle and cortical fraction.
There have been prior studies that have used advanced imaging to qualify the morphology of the medial epicondyle in overhead athletes. In a well-designed study by Hurd et al, 6 a cohort of 23 uninjured, high school pitchers were studied with bilateral elbow MRIs. The authors studied both osseous and soft tissue structures and noted a multitude of asymmetric differences between the dominant and nondominant arms of the study group (only 3 pitchers displayed no differences between the 2 arms on MRI). These findings included variations in the ulnar collateral ligament band thickening, presence of posteromedial subchondral sclerosis, presence of posteromedial olecranon osteophytes, and several other less-common findings. While these authors were able to demonstrate the high likelihood of MRI findings on asymptomatic throwers, they did not comment on specific differences in medial epicondyle morphology between the dominant and nondominant elbow. Our study included a similar number of overhead athletes (n = 22) and focused specifically on the osseous medial epicondyle, using both CT and MRI scans to construct 3D computer simulations of the distal humerus.
This study is not without limitations. There were several patients excluded from the study because of poor image quality, involvement of the nondominant limb, or because of female sex. However, these strict inclusion and exclusion criteria were designed to minimize geometric variation due to patient demographics. Moreover, our inclusion of 37 patients is still higher in number than several studies using advanced imaging to investigate characteristics of the medial epicondyle in overhead athletes, specifically throwers. 6,11 Another limitation in this study was the lack of a pure control, for example, imaging of the nondominant arm within the overhead athlete populations. This was in part because of the retrospective nature of this study. Additionally, strict inclusion and exclusion criteria were used to alleviate this lack of inclusion. One additional limitation was the lack of investigation of the soft tissue structures of the elbow (ulnar collateral ligament, articular cartilage, etc). As a result, the findings of this study may only relate to the osseous structures of the elbow related to the medial epicondyle. Finally, the cohort of control patients was older than that of overhead athletes. The impact of this discrepancy was addressed by only including patients who had reached skeletal maturity. However, there may be cortical bone loss in the older patients that would affect the comparison of cortical bone composition between the 2 groups.
Conclusion
This anatomic computer-simulated study was able to detect discrete differences in the morphology of the medial epicondyle between our cohort of overhead athletes and control patients. In overhead athletes, the medial epicondyle has a larger volume and more acute extrusion when compared with control subjects. This difference in size is largely because of increased thickness, along with slightly increased height as well. We found no significant difference in the morphology of the inferior aspect of the epicondyle, but variations within patients undergoing ulnar collateral ligament reconstruction may be important when considering tunnel placement. Future studies will be helpful in determining the precise relationship between these size differences and at-risk soft tissue structures (eg, ulnar collateral ligament) in the overhead athlete. Additionally, such an investigation may assist the treating surgeon in preoperative planning during procedures such as ulnar collateral ligament reconstruction.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: C.S.A. is a consultant for Accumed and Arthrex, receives sutures and implants from Stryker, and receives research support from Zimmer and Major League Baseball. All sponsorship for this project was provided by internal funding from the Columbia University Medical Center Department of Orthopaedic Surgery.