
Abstract
Background:
Shoulder instability is a common problem in young athletes and can lead to pain and decreased ability to participate in high-level activities. Little is known about the modifiable risk factors for glenohumeral joint instability.
Hypothesis:
Isometric shoulder strength at baseline would be a modifiable risk factor associated with subsequent first-time anterior instability events.
Study Design:
Cohort study.
Methods:
Study participants were freshmen entering the United States Military Academy in June 2006. All participants completed bilateral isometric strength evaluations with a hand-held dynamometer at baseline upon entry into the study. Variables measured included internal and external rotation at 0° (IR0, ER0) and internal and external rotation at 45° of abduction (IR45, ER45). All subjects were followed for subsequent glenohumeral joint instability events until graduation in May 2010. Independent t tests were used to analyze the data.
Results:
Baseline strength data were available for 1316 shoulders with no prior history of instability, of which 26 went on to have an acute first-time anterior shoulder instability event while the individuals were at the academy. There were no significant differences in mean strength between shoulders that did not go on to develop instability (uninjured; n = 1290) and those that did develop anterior instability (injured; n = 26). The mean strength values in pounds of force for uninjured and injured shoulders, respectively, were as follows: IR0 (49.80 vs 49.29; P = .88), ER0 (35.58 vs 33.66; P = .27), IR45 (47.38 vs 46.93; P = .88), and ER45 (40.08 vs 38.98; P = .59).
Conclusion:
No association was found between isometric shoulder strength measures at baseline and subsequent first-time anterior glenohumeral joint instability within the high-risk athletic population studied in this prospective cohort.
The glenohumeral joint has an extremely wide range of motion, rendering it susceptible to dislocations and subsequent instability. 32 This common orthopaedic problem can lead to pain, poor function, and a decrease in overall health.6,21,25 A young, athletic population involved in athletics and military activities may be at higher risk for shoulder instability.18,19,21,32
Both static and dynamic stabilizers are engaged in keeping the glenohumeral joint stable. Static stabilizers include the glenoid labrum, the glenohumeral ligaments and capsule, the articular surface of the glenoid, and the negative intra-articular pressure. Dynamic stabilizers include the rotator cuff and periscapular musculature. A balance between static and dynamic stabilizers as well as coordinated contraction of rotator cuff muscles is essential for glenohumeral stability. The rotator cuff works to center the humeral head on the glenoid during motion.3,13,23,28
Numerous studies have investigated a link between shoulder strength and instability. ‡ Several demonstrate or imply that an imbalance in or alteration of rotator cuff strength may lead to shoulder pain and possible injury.1,15,23,25,27,28 In a dynamic cadaver shoulder model study, Wuelker et al 30 found that anterior-posterior displacement at the glenohumeral joint increased 39%, with a 50% loss of rotator cuff force. A recent study by Edouard et al 4 reported an association between rotator cuff weakness and recurrent anterior instability. Based on their findings, the authors posed the question of whether the rotator cuff weakness was the cause or the result of the instability and recommended further prospective study to answer this important question. The purpose of the current study was to prospectively examine the association between baseline rotator strength and the subsequent risk of first-time glenohumeral instability during 4 years of follow-up. The hypothesis was that rotator cuff weakness would be a modifiable risk factor for subsequent first-time anterior glenohumeral instability.
Materials and Methods
Design
A prospective cohort study of freshman entering the United States Military Academy (USMA) in June 2006 was conducted. We obtained demographic data, physical examination, magnetic resonance imaging, and strength assessments at baseline and followed all subjects for 4 years to document all subsequent glenohumeral instability events in the cohort until graduation in May 2010. The primary outcome of interest was the relationship between baseline rotator strength and the advent of subsequent glenohumeral instability during the follow-up period, defined as a glenohumeral dislocation. The institutional review board at our institution reviewed and approved this study prior to initiation.
Participants
Of the 1311 members of the incoming class of 2010 at USMA, 1050 students (80%) agreed to participate in and gave informed consent for this study. Seven hundred fourteen students (1428 shoulders) completed baseline assessments. The participants were healthy and medically fit according to the standards of the USMA. Athletic participation included a variety of sports and physical requirements throughout the 4 years of school. 14 Exclusion criteria included current shoulder symptoms (pain, weakness, instability), history of shoulder instability or trauma, neurologic disease, and current cervical or thoracic spine pain or surgery. Potential subjects completed baseline questionnaires to establish demographics, history of prior injury, and history of physical activity. All subjects underwent a standardized evaluation by an orthopaedic surgeon, including active range of motion, assessment of generalized joint hypermobility, and tests for shoulder impingement and instability. 20 We excluded 112 shoulders for prior history of glenohumeral instability. After excluding those with a history of instability, 1316 shoulders were included for analysis in the current study (Figure 1). Each shoulder was considered as an individual unit to eliminate possible strength bias based on handedness within subjects.
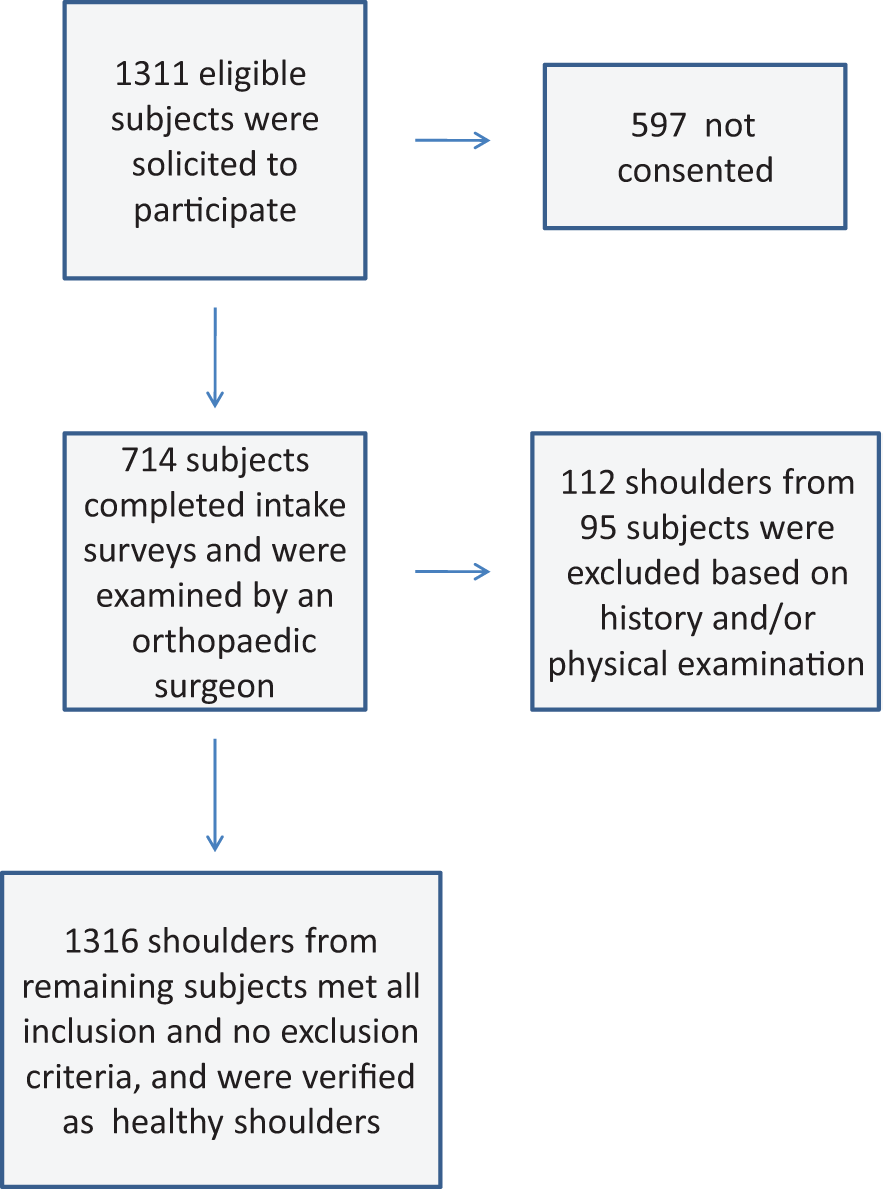
Flow diagram showing study subjects available for analysis.
Hand-Held Dynamometer Isometric Strength Testing
A hand-held dynamometer (Model 01163; Lafayette Instrument Co, Lafayette, Indiana), found to be valid and reliable in several studies,9,11,31 was used to measure bilateral isometric shoulder strength. Three researchers obtained the strength measurements after reviewing and practicing the standardized testing protocol, testing positions, and procedures described below. Intraclass correlation coefficients were calculated along with intra- and interrater reliability for all 3 researchers. Intraclass correlation coefficients for interrater reliability ranged from 0.792 for external rotation in neutral position to 0.905 for internal rotation in 45° of abduction. Intraclass correlation coefficients for intrarater reliability across trials were similar, ranging from 0.725 to 0.985 for rater 1, 0.631 to 0.969 for rater 2, and 0.776 to 0.957 for rater 3. 29
The strength measures recorded included internal and external rotation in the neutral position (IR0 and ER0) and internal and external rotation in the 45° abducted position (IR45 and ER45). The dynamometer was placed just proximal to the styloid process of the wrist for all measurements. Subjects were asked to produce a 5-second maximal contraction (make test) to record during each trial rather than a break test during which they could not hold the contraction for 5 seconds.22,26 The greater of 2 trials completed for each position was used as the measure of muscular strength. 2
Measurements of IR0 and ER0 were obtained with subjects in the seated position with the upper extremity in the neutral position (Figure 2). This most closely replicates the position commonly used for clinical assessments. Strength measurements have been found to be similar between the seated unsupported neutral position and a bolster-supported position keeping 30° each of abduction, scaption, and diagonal position. 22 The IR45 and ER45 measurements were taken with subjects in the supine position with the shoulder abducted to 45° and neutral flexion/extension (Figure 3). A bolster was used to assist in maintaining 0° of flexion/extension. The supine IR45 and ER45 helped to stabilize the scapulothoracic joint, with the shoulder abducted to the scapular plane. This position is commonly used during manual muscle testing of the rotator cuff musculature. 10
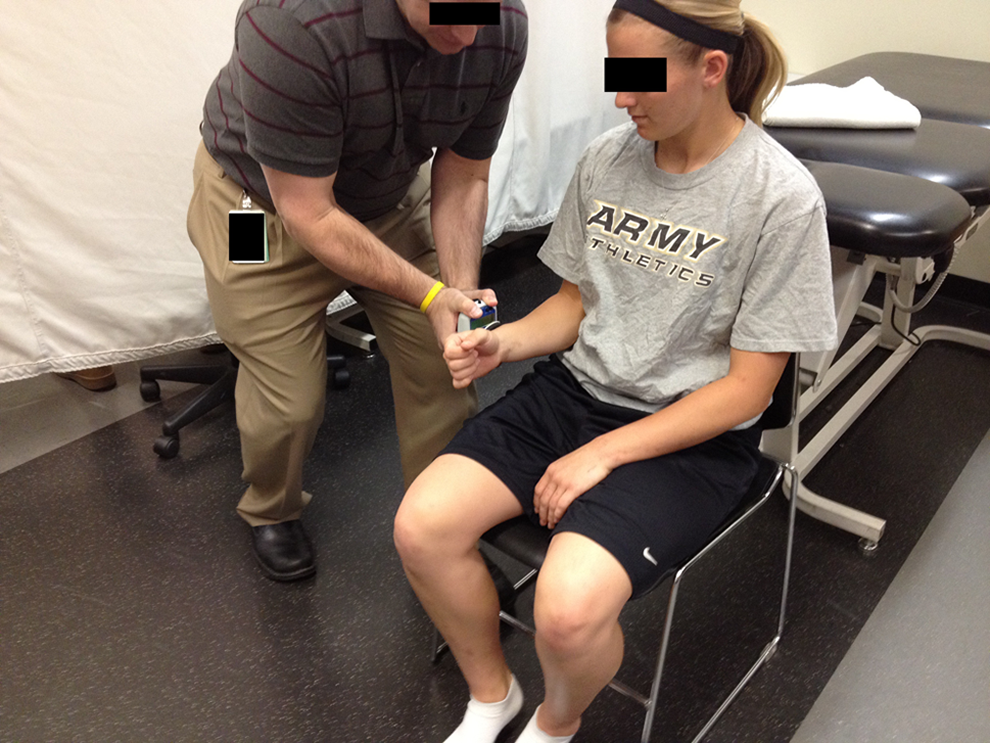
Measurement of external rotation at 0° of abduction with the subject in a seated position, maintaining the elbow and wrist at neutral position and hand-held dynamometer just proximal to radial styloid.

Measurement of internal rotation at 45° of abduction with the subject in a supine position, maintaining the elbow and wrist at neutral position and hand-held dynamometer just proximal to radial styloid.
Statistical Analysis
Initially, means and standard deviations were calculated for continuous variables and counts and frequencies for categorical variables. Independent t tests were used to compare strength measures between those who experienced a first-time anterior instability event during follow-up and those who did not, using each shoulder as the unit of analysis. Subsequently, univariate and multivariable Cox proportional hazards models were used to examine the association between baseline strength measure and the time to first-time anterior instability during the follow-up period. Multivariable models for each strength measure were controlled for the influence of sex, height, weight, and hand dominance. All statistical analyses were performed using the STATA SE version 10.1 (StataCorp, College Station, Texas).
Results
Of the 1316 shoulders included in the analysis, 26 sustained an acute first-time anterior instability event during follow-up and 1290 did not. Means and standard deviations for each strength measure by group are reported in Table 1. There were no significant differences in rotator cuff strength between shoulders in which acute instability events occurred when compared to those that did not sustain an instability event. Furthermore, there were no differences in the ratios of internal to external rotation strength between groups. Similar results were observed in univariate Cox proportional hazards regression models and in multivariable models after controlling for the influence of sex, height, weight, and hand dominance (Table 2).
Strength Measures (in Pounds of Force) for Injured and Uninjured Shoulders for Internal and External Rotation a

a SD, standard deviation; IR, internal rotation; ER, external rotation.
Hazard Ratios Between Groups Comparing the Time to Acute Instability Events During Follow-up a
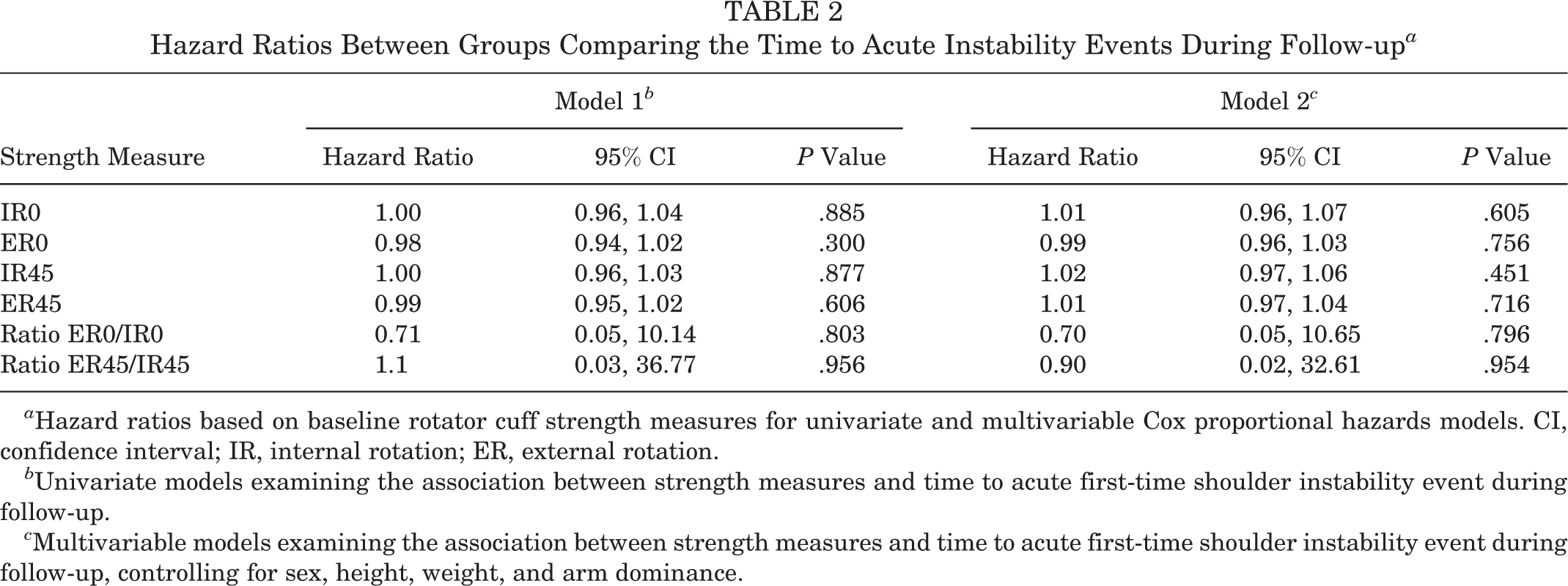
a Hazard ratios based on baseline rotator cuff strength measures for univariate and multivariable Cox proportional hazards models. CI, confidence interval; IR, internal rotation; ER, external rotation.
b Univariate models examining the association between strength measures and time to acute first-time shoulder instability event during follow-up.
c Multivariable models examining the association between strength measures and time to acute first-time shoulder instability event during follow-up, controlling for sex, height, weight, and arm dominance.
Because we did not observe an association between baseline strength measures and first-time glenohumeral instability during the follow-up period, a post hoc power analysis was conducted using the data in Table 1 to determine the number of subjects that would be needed to detect a significant difference in rotator cuff strength between groups. The results suggest that the effect of baseline strength on subsequent first-time shoulder instability risk is quite small (Table 3).
Estimated Sample Size Needed to Detect a Significant Difference in Baseline Rotator Cuff Strength Measures Between Shoulder Instability Cases and Uninjured Controls During the 4-Year Follow-up Period a

a Sample size estimates based on group means and standard deviations in Table 1, assuming a P value of .05 and power of 0.80. IR, internal rotation; ER, external rotation.
Discussion
The purpose of this research was to determine whether strength was a modifiable risk factor for first-time anterior glenohumeral dislocation. We did not find an association between baseline shoulder strength and the risk for subsequent first-time anterior glenohumeral instability. Also, there was no difference in the ratio of internal rotation strength to external rotation strength between subjects who went on to experience acute instability events and those that did not. To our knowledge, this is the first prospective study investigating a possible link between baseline strength and subsequent first-time anterior glenohumeral instability events.
Several previous studies discuss an imbalance in rotator cuff strength as a cause for shoulder pain and injuries in general.1,15,23,25,27,28 These were cross-sectional or case-control studies measuring strength in injured cases versus uninjured controls or no controls at all. As a result, they could not adequately assess the temporal relationship between rotator cuff strength and subsequent instability. A consistent finding in these studies is a decrease in shoulder internal rotation strength in injured shoulders, including those with instability. Some authors have demonstrated that rehabilitation programs that increase rotator cuff strength and improve imbalances may help prevent injuries.8,17 Another common hypothesis is that injured or stretched static constraints force the dynamic rotator cuff muscles to compensate for the loss of static stabilization, causing imbalances and leading to injury.12,23,25 Glousman et al 7 found increased biceps and supraspinatus activity in shoulders with anterior instability. Myers and Lephart 16 emphasized the role of proprioception in shoulders with capsuloligamentous injuries, stating that the combination of neuromuscular interruption and mechanical failure created an unstable shoulder.
Although most research shows a trend associating lack of shoulder strength with shoulder instability and injury, not all studies were in agreement with this concept. In looking at male baseball players and comparing strength between those with and without translational instability, Falla et al 5 determined that there were no strength differences between groups and concluded that strength testing cannot be used as a diagnostic tool to identify people with glenohumeral translational instability. Stickley et al 24 studied peak torque ratios and shoulder history in adolescent female volleyball athletes and found that rotator cuff strength was not predictive of injury history. Notably, these studies did not address solely acute first-time instability events and did not attempt to determine the causal relationship between strength and instability. Despite the inconsistent research associating shoulder strength and instability, a general conclusion is that specific rehabilitation programs can and should be developed to create a dynamically balanced shoulder.
Particular attention was given to the recent study by Edouard et al, 4 in which the authors compared strength in patients having recurrent anterior instability with a group of healthy nonathletic subjects with no shoulder symptoms. They found that rotator cuff weakness was associated with recurrent anterior instability. However, as opposed to some previous studies,1,23,28 Edouard et al found no difference in the ratio of external and internal strength. Their conclusion was that patients with recurrent anterior instability have rotator cuff weakness, but it was unclear whether this weakness was due to anterior instability or the cause of it. Our study implies that the strength deficit is a result of anterior instability, because we found no differences in the strength of shoulders that did and did not develop an acute first-time anterior instability event during follow-up.
The greatest strength of this study is that we prospectively followed a large cohort of active subjects with a baseline strength assessment for 4 years to document subsequent anterior instability events. Previous studies have only concentrated on specific groups of athletes such as swimmers,1,23 baseball players,5,15 volleyball players,24,27 tennis players, 17 throwing athletes, 7 or subjects that already had instability.4,8,25,28 Furthermore, many of these studies did not focus on acute first-time anterior instability events. Although our subject cohort may not typify the average person, the population is one that is especially vulnerable to acute shoulder instability events across a wide variety of athletic activities. 21 It is comparable to a young athletic high school or college-aged population. To our knowledge, this is the first large, prospective study looking at the association between baseline shoulder rotator cuff strength and subsequent first-time anterior shoulder dislocation.
There were several limitations to our study. Only 26 acute first-time glenohumeral instability events were observed during the follow-up period, which may have negatively affected the study power; however, a post hoc power analysis suggests that the effect size associated with baseline shoulder strength and subsequent instability is quite small. The study population, while being a young athletic cohort, may have a bias toward fewer injuries because of the admission requirements of the Military Academy. Prospective students are prescreened for health problems to include previous musculoskeletal instabilities and also must pass certain physical testing requirements before admittance. These requirements may exclude potential subjects with extreme rotator cuff weakness at baseline. Additionally, the study excluded potential subjects who were having current shoulder symptoms or instability, which prevented the inclusion of anyone who had shoulder instability before attendance at the USMA. Also, we did not delineate exactly how the instability events occurred, which could have been useful to compare traumatic and atraumatic mechanisms, if present. With regard to rotator cuff testing, we only tested strength at baseline and did not follow strength measurements throughout the 4 years of patient participation in activities at the Academy. Students may have increased strength during their time at USMA, effectively decreasing their possibility of potential weakness-related shoulder injuries. In addition, testing was done at 0° and 45° of abduction, whereas most instability episodes happen at higher abduction angles. Finally, we examined only the internal and external rotation muscles, whereas other muscles such as the pectoralis major, serratus anterior, biceps, and others are certainly involved as secondary dynamic stabilizers of the shoulder.
Conclusion
The results of the current study suggest that there is no association between baseline shoulder isometric strength and subsequent first-time anterior glenohumeral instability in the young athletic cohort studied. This implies that strength deficits found in subjects with anterior instability are likely the result of instability and/or inadequate rehabilitation and not the cause of the instability. It also appears that isometric rotator cuff strength is not a modifiable risk factor for first-time anterior glenohumeral instability. Further prospective research is needed to identify the modifiable risk factors associated with first-time shoulder instability injuries to develop effective primary prevention interventions.
Footnotes
The views and opinions expressed in this article are those of the authors and do not reflect the official policy of the Department of the Army, the Department of Defense, or the US Government.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was aided by a grant from the Orthopaedic Research and Education Foundation.