
Abstract
The burden of noncommunicable diseases (NCDs) is increasing among people living with HIV (PLHIV) in Ethiopia; however, evidence on NCD prevalence among those receiving antiretroviral therapy (ART) is limited. This study assessed the magnitude of NCDs and associated factors among adult PLHIV attending ART clinics in general hospitals of Sidama Region, Ethiopia. We conducted a hospital-based cross-sectional study, involving 422 PLHIV selected through systematic random sampling. Data were collected using Kobo Toolbox and analyzed with SPSS version 26. Logistic regression identified factors associated with NCDs. The magnitude of NCDs was 24.8% (95% CI: 20.6%, 28.9%). The most common conditions included hypertension (7%), diabetes (5.7%), cardiovascular diseases (4.8%), cancers (4%), and chronic respiratory diseases (3.3%). Older age, urban residence, opportunistic infections, overweight/obesity, and abnormal waist circumference were significantly associated factors. NCDs are common among adult PLHIV in the region, necessitating integrated ART and NCD screening.
Plain Language Summaries
Why was the study done?
In Ethiopia, many people living with HIV are also developing other health problems known as noncommunicable diseases (NCDs). However, we know very little about how common these diseases are among those receiving HIV treatment. This study focused on understanding how many people with HIV attending treatment clinics in the Sidama Region also have NCDs and what factors might contribute to this.
What did the researchers do?
We conducted a study at general hospitals from March 4 to April 30, 2024, involving 422 adults with HIV. Participants were chosen randomly, and information was collected through structured interviews using a survey tool. We analyzed the data to find out which factors are linked to having NCDs.
What did the researchers find?
We found that 24.8% of adults with HIV at these clinics had at least one NCD. The most common conditions were high blood pressure (7%), diabetes (5.7%), heart disease (4.8%), cancer (4%), and chronic lung disease (3.3%). We discovered that older age, living in urban areas, having certain infections, being overweight, and having a large waist size all increased the likelihood of also having an NCD.
What do the findings mean?
NCDs are common among adults with HIV in the Sidama Region. Key factors that increase the risk include older age, urban living, certain infections, and being overweight. To tackle this issue, it's important to combine HIV treatment with regular screenings for NCDs and to improve our healthcare monitoring systems.
Keywords
Introduction
Noncommunicable diseases are the leading cause of death globally, accounting for about 75% of nonpandemic-related deaths in 2021 (43 million people). Of these, 73% happened in resource limited settings. In economically disadvantaged nations, which bear 82% of premature deaths (<70 years), cardiovascular conditions is leading cause (19 million deaths). Other leading causes include cancer (10 million), chronic respiratory diseases (4 million), and diabetes-related deaths 2 million). 1 The increasing burden, which is brought on by urbanization, ageing populations, and lifestyle factors (such as smoking, poor diet, inactivity, and air pollution), disproportionately affects younger people in resource-constrained conditions where healthcare systems are unable to prevent, detect, and treat. 2
The burden of NCDs among PLHIV has become a significant public health concern, especially for those on ART. 3 Even though ART has greatly extended life expectancy, it has also been linked to a higher risk of NCDs because of a confluence of factors, including HIV-related immune activation, chronic inflammation, ART-related metabolic complications, and conventional risk factors like smoking, eating poorly, and leading a sedentary lifestyle. 4 The burden of noncommunicable diseases is a challenging issue for HIV care programs that necessitates the use of integrated healthcare techniques. 5
A complex interaction of variables, including co-infections, lifestyle choices, and HIV-specific factors, influences the presence of NCDs in people living with HIV. 6 Significant causes include unhealthy habits like smoking, drinking, and not exercising. 7 Furthermore, opportunistic infections like tuberculosis and co-infections like hepatitis B or C raise the risk of NCDs in this population. 8 The presence and progression of NCDs are also significantly influenced by HIV-related variables, including as immunosuppression, chronic inflammation, and the long-term consequences of ART.9,10 NCD distribution in PLHIV varies based on demographics, including socioeconomic status, age, gender, and healthcare availability. Since PLHIV have a higher risk of developing NCDs than the general population, integrated care measures are essential. 11
In Ethiopia, NCDs represent a growing public health challenge, accounting for an estimated 554 deaths per 100,000 population. It is estimated that about 25 Ethiopians die every hour due to NCDs. The majority of these deaths are attributed to cardiovascular diseases (42%), followed by neoplasms (17%), digestive disorders (15%), diabetes mellitus (12%), and chronic respiratory diseases (7%). 12 In contrast, the burden of NCDs among adult PLHIV attending ART clinics in Ethiopia has also emerged as a significant concern. 13 This increased burden is attributed to the combined effects of chronic HIV infection, long-term exposure to ART, and traditional lifestyle-related risk factors. 14
Moreover, PLHIV in Ethiopia are increasingly experiencing NCD comorbidities, partly due to the historically limited integration of NCD services within HIV care programs, which has often led to delayed diagnosis and treatment of chronic conditions. 13 While HIV care programs have been highly effective in controlling viral diseases, they have traditionally focused primarily on viral suppression and opportunistic infection management, often overlooking the prevention and management of chronic noncommunicable illnesses. 15 Improving patient outcomes and attaining long-term health system resilience need bolstering healthcare systems to deliver integrated HIV and NCD services. 16
The increasing prevalence of HIV-NCD comorbidity in Ethiopia is posing a new public health concern. However, there are substantial evidence gaps of the local burden of NCDs in PLHIV due to regional differences in sociodemographic, lifestyle, HIV prevalence, and healthcare access. This highlights the need to assess regional patterns in HIV-NCD co-occurrence. Thus, this study assessed the magnitude of NCDs and associated factors among adult PLHIV attending ART clinics of general hospital Sidama Region, Ethiopia.
Methods and Materials
Study Area and Period
This study was carried out among adult PLHIV receiving care at ART clinics in general hospitals within the Sidama Region. As one of the 12 federal regions in Ethiopia, it lies just over 273 km from Addis Ababa in a southern direction. Home to approximately five million people, the region is structured into four zones, 30 rural districts, six town administrations, and a single city administration. The region's healthcare system comprises 553 health posts, 140 health centers, 17 primary hospitals, seven general hospitals, and one tertiary hospital, with ART services accessible at all government hospitals. The investigation took place over a 2-month period, commencing on March 4th and concluding on April 30th, 2024.
Study Design and Reporting Standards
This study employed an institution-based cross-sectional design and was conducted and reported in accordance with the STROBE Statement checklist for cross-sectional studies. A completed STROBE checklist is provided in the Supplemental Materials. 17
Study Population and Eligibility Criteria
The study population comprised all PLHIV aged ≥18 years attending ART clinics in Sidama Region's four general hospitals during the study period. We excluded PLHIV who had physical disabilities, mental illness, or declined to participate in the study.
Sample Size Determination
The required sample size for estimating the magnitude of NCDs was computed using the single-population proportion formula. The calculation incorporated a 95% confidence level (CL), a 5% margin of error, a prior estimate of 51.3% prevalence of NCDs among adult PLHIV, 18 and a 10% anticipated nonresponse rate. The calculated sample size was 422 participants.
To assess the factors associated with NCDs, the required sample size was computed using the double population proportion formula via Epi Info™ 7. A prior study 18 had established ART duration as a significantly associated factors of NCDs. The calculation incorporated the following parameters: 95% CL, 80% statistical power, a 1:1 allocation ratio between participants with ≥6 years of ART exposure and those with <6 years, and an outcome of 39.3% in the unexposed group, and an odds ratio (OR) of 2.0. Based on these inputs, the sample size estimation yielded 317 participants. Consequently, the final sample size for the study was determined to be 422.
Sampling Procedures
Among the seven regional general hospitals, four facilities (Adare, Bona, Leku, and Yirgalem) were randomly selected through simple random sampling. The sample was distributed proportionally according to each hospital's 2-month HIV patient registry data at ART clinics (counted unique patients). A systematic random sampling method was then employed to select study participants. Using the ART patient registry, we derived the sampling interval (K) through the formula K = N/n, where N = 834 and n = 422, yielding an interval of approximately 2. The initial participant from each hospital was randomly selected through a lottery-based selection process.
Study Variable
The primary outcome variable was the presence or absence of NCD comorbidities among adult PLHIV receiving ART. The NCDs assessed in this study included hypertension, diabetes mellitus, cardiovascular diseases, cancer (any type), and chronic respiratory diseases; all were extracted from medical records except hypertension. Moreover, ten independent variables were analyzed: (1) age, (2) place of residence, (3) occupation, (4) ART duration, (5) khat chewing, (6) physical activity, (7) opportunistic infections, (8) clinical stage, (9) waist circumference, and (10) body mass index (BMI, kg/m2).
Data Collection Procedure
Data was gathered using an interviewer-administered, pretested, structured questionnaire. The data collection tool was developed based on a thorough review of relevant literature.16,18,19 The tool was initially prepared in English, then translated into Amharic by a native language expert, and back-translated into English by another bilingual expert to ensure accuracy. The questionnaire covered key domains, socio-demographic/economic factors, clinical factors (duration of ART use, WHO HIV stage, and opportunistic infections), behavioral factors (cigarette smoking, alcohol use, chewing chat and physical inactivity), psychosocial factors, anthropometric measurements and medical records review. Under the supervision of two MPH-qualified experts, four health officers (all holding a bachelor of science) gathered data through in-person interviews and document analysis. The Kobo Toolbox application, installed on Android devices, facilitated data collection with automatic submission to a central server.
PLHIVs’ weight was measured using a SECA digital scale (Seca GmbH & Co. KG, Germany), without shoes and with light clothing, to the nearest 100 g. The weighing scale was positioned on a level surface. Height measurement was conducted using a measuring tape attached to a vertical wall, with a horizontal headboard touching the highest point of the head. Height was recorded in meters to the nearest 0.1 cm, while barefoot or in thin socks. To reduce discrepancies between observers, all measurements were conducted by a skilled anthropometrist. 20
The BMI computation involved taking a person's weight in kilograms and dividing it by their height in meters multiplied by itself (kg/m2). Participants were classified based on BMI: ≥30 kg/m2 indicated obesity, 25–29.9 kg/m2 signified overweight, while 18.5–24.9 kg/m2 represented normal weight. 21
Waist circumference was measured at the midpoint between the lower rib margin and the iliac crest using a nonstretchable measuring tape, with participants standing upright and breathing normally. Two consecutive measurements were taken to the nearest 0.1 cm, and the average was recorded; a third measurement was performed if the first two differed by more than 1 cm. Waist circumference readings were assessed using the WHO-defined threshold values. As per these standards, a waist circumference above 94 cm for males or 80 cm for females is considered abnormal. 22
A calibrated digital blood pressure monitor was used to record measurements while participants remained seated in a relaxed position, with their arm comfortably rested at heart level. Measurements were taken after a 5-min rest, with two readings recorded at 3-min intervals; a third reading was taken if the difference exceeded 5 mm Hg, and the average was used for analysis. Hypertension was defined as systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥ 90 mm Hg.23,24
Data Quality Control
Data collectors and supervisors underwent thorough training in Kobo Toolbox and interview techniques. The tool was pretested on 5% of the sample, leading to necessary refinements. Daily supervision ensured accuracy, with errors promptly corrected. PLHIVs’ physical measurements were taken using calibrated scales. Kobo Toolbox streamlined data entry, preserving quality, while supervisors verified completeness to maintain data integrity.
Data Management and Analysis
Data were collected using the Kobo Toolbox platform and then imported into SPSS Version 26.0 for analysis. Measures of dispersion, central tendency, and frequency distributions were used to characterize the data. Principal component analysis (PCA) was used to determine the household's wealth index. Body mass index was calculated as weight in kilograms divided by the square of height in meters (kg/m2). Waist circumference was classified based on established cutoff values, with measurements compared to standard thresholds to assess central obesity risk (94 cm for men, >80 cm for women).
Bi-variable and multivariable logistic regression analyses determined the association between independent variables and the outcome variable. Variables with a P < 0.25 in the bivariable model were included in the multivariable logistic regression model to mitigate the impact of confounding variables. The model's fitness was assessed using the Hosmer and Lemeshow tests (P = 0.624), and multicollinearity was examined using the variance inflation factor (VIF ≤ 2.203). Statistical significance in the multivariable analysis was declared at a P < 0.05. Findings were presented using adjusted odds ratios (AOR) and 95% CI.
Results
Sociodemographic and Economic Characteristics of Study Participants
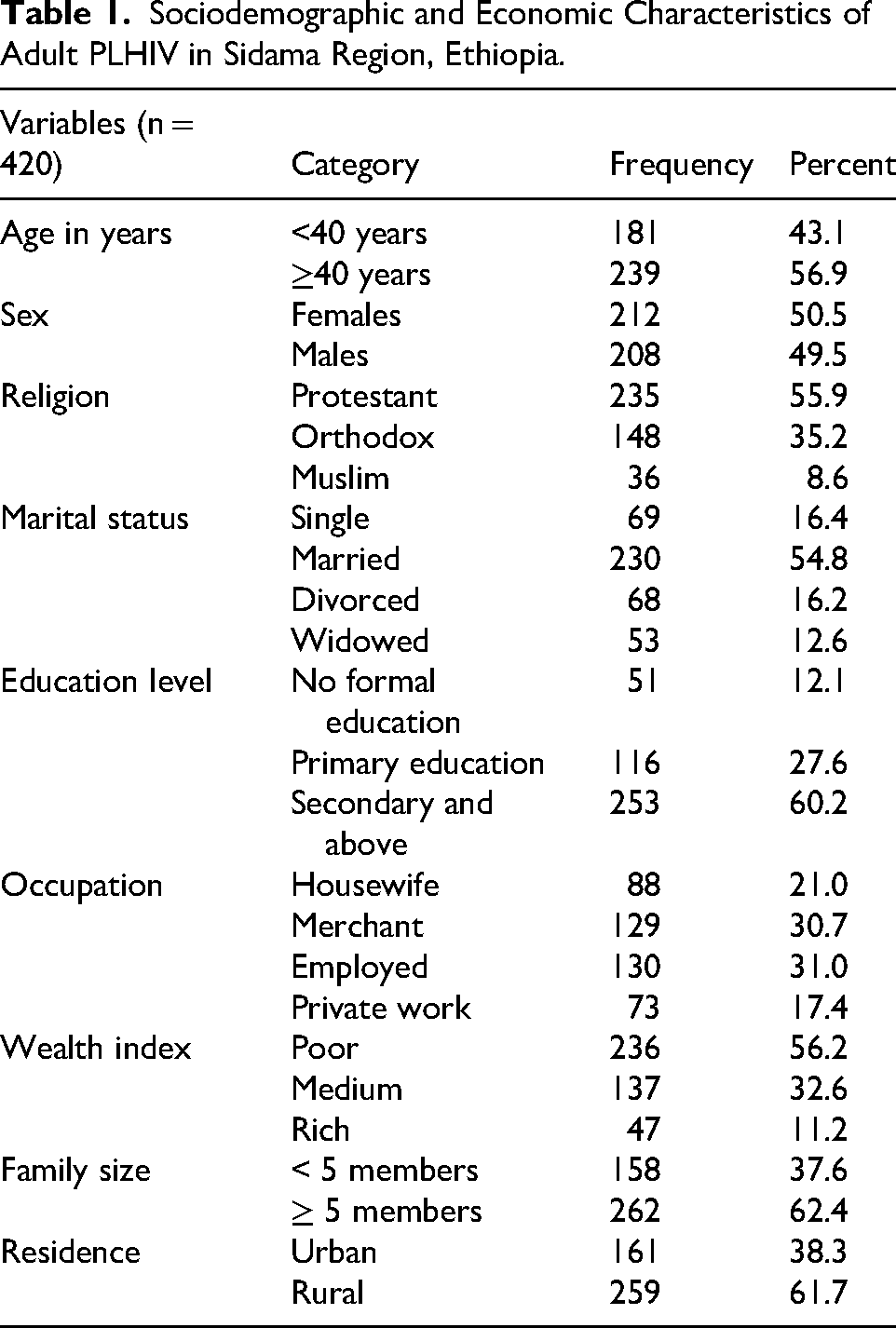
A total of 420 adult PLHIVS participated in this study, resulting in a response rate of 99.5%. The median age of the respondents was 40 years, with an interquartile range (IQR) of 14 years. Two hundred thirty-nine (56.9%) of the respondents were aged 40 years and above. Half (49.5%) of the respondents were male. Two hundred thirty five (55.9%) of the study participants were Protestant religion followers. Regarding the participants’ marital status, more than half (54.8%) were married. Two hundred fifty three (60.2%) of the respondents had attended primary education or higher. About one-third (31%) of the study participants were employed. Slightly greater than one-third of the respondents (38.3%) were urban dwellers. Two hundred and sixty two (62.4%) of respondents’ families had five or more members. Pertaining to wealth tertiles, 56.2% of study participants’ households were categorized as having a poor wealth index (Table 1).
Sociodemographic and Economic Characteristics of Adult PLHIV in Sidama Region, Ethiopia.
Lifestyle and Health-Related Factors among Study Participants
Regarding lifestyle and health-related factors, study participants reported the following habits. Four-fifths (81%) of respondents expressed no concern about salt or sugar levels in their food, while 90.5% consumed fruits or vegetables fewer than 5 days per week. The vast majority (93.4%) did not engage in regular physical exercise. Substance use patterns included alcohol consumption (19.3%), habitual khat chewing (16.7%), and cigarette smoking (5.7%). Regarding metabolic health, 22.1% were overweight or obese (BMI ≥25 kg/m2), and 21.4% had an abnormal/elevated waist circumference (≥94 cm for men, >80 cm for women), indicating increased metabolic risk (Table 2).
Lifestyle and Health-Related Factors among Adult PLHIV in Sidama Region, Ethiopia.

Clinical Stage and Opportunistic Infection among Study Participants
According to WHO clinical staging for ART, 54.3% of study participants were classified as stage I. The median ART duration was 5.75 years (IQR: 6 years), with about half (49.3%) of respondents on treatment for ≥ 6 years. Opportunistic infections were reported by 59% of respondents, with 13.8% of these cases involving co-infections. The most common opportunistic infections included pneumonia (34.3%), oral thrush (31.0%), chronic diarrhea (19.4%), and tuberculosis (15.3%) (Table 3).
Clinical Stage and Opportunistic Infection among Adult PLHIV in Sidama Region, Ethiopia.

Prevalence of Noncommunicable Diseases among Adult PLHIV
The prevalence of NCDs among adult PLHIV was 24.8% (95% CI: 20.6, 28.9). Two or more NCDs (multimorbidity) were observed in 3.8% of study participants (95% CI: 1.9, 5.6). Hypertension was the most prevalent, affecting 7.0% (95% CI: 4.8, 9.1) of patients, followed by DM at 5.7% (95% CI: 3.5, 7.9). Cardiovascular diseases reported in 4.8% (95% CI: 2.8, 6.8) of cases, while cancer affected 4% (95% CI: 2.1, 5.9) of patients. Moreover, 3.3% (95% CI: 1.6, 5.0) of participants were diagnosed with chronic respiratory disease (Fig 1).

Prevalence of noncommunicable diseases among adult PLHIV in Sidama Region.
Associated Factors of NCDs among Adult PLHIV
In this study, both bivariable and multivariable logistic regression analyses were conducted to identify associated factors of noncommunicable diseases among patients receiving ART. Ten independent variables were considered as candidate variables for the multivariable model, including age, place of residence, occupation, khat chewing, physical exercise, clinical stage, ART duration, opportunistic infection, body mass index, and waist circumference. The multivariable logistic regression analysis revealed significant associations between NCDs and the following factors: age, place of residence, opportunistic infection, waist circumference, and BMI (P < 0.05) (Table 4).
Multivariable Logistic Regression Analysis of Associated Factors of NCDs among Adult PLHIV in Sidama Region, Ethiopia.

Note. AOR = Adjusted odds ratio; ART = Anti-retro viral therapy; BMI = Body mass index; COR = Crude odds ratio; CI = Confidence interval; IQR = Interquartile range; NCDs = Non communicable diseases; PLHV = People Living with HIV.
*P < 0.05, **P < 0.001.
Age was significantly associated with the presence of NCDs among adult PLHIV, with PLHIV aged ≥40 years having 2.16 times higher odds of NCDs compared to their counterparts (AOR = 2.16; 95% CI: 1.03, 4.51). Opportunistic infections also increased the likelihood of NCDs, as patients with recurrent infections had 3.21 times higher odds (AOR = 3.21; 95% CI: 1.51, 6.83). Moreover, place of residence significantly influenced NCDs prevalence, with urban dwellers exhibiting 4.50 times higher odds (AOR = 4.50; 95% CI: 2.27, 8.93) compared to rural residents. Among ART clinic attendees, those with an abnormal or elevated waist circumference (≥94 cm for men, >80 cm for women) had 3.11 times higher odds of developing NCDs (AOR = 3.11; 95% CI: 1.22, 7.93) than their counterparts. Furthermore, BMI was a significant determinant, with each one-unit increase in BMI raising the odds of NCDs by 1.60 times (AOR = 1.60; 95% CI: 1.38, 1.85) (Table 4).
Discussion
This institution-based cross-sectional study assessed the magnitude and associated factors of NCDs among adult PLHIV attending ART clinics in Sidama region general hospitals. The overall prevalence of NCDs was 24.8%, with hypertension (7.0%), diabetes mellitus (5.7%), cardiovascular diseases (4.8%), cancer (4.0%), and chronic respiratory diseases (3.3%) being the most common. Factors significantly associated with NCDs included older age, urban residence, opportunistic infections, overweight/obesity, and abnormal waist circumference.
According to our study, the region's adult PLHIV had a 24.8% prevalence of NCDs. This finding is consistent with studies from Uganda (20.7%) 25 and Central Denmark (21.9%), 26 which reported comparable magnitudes. However, lower prevalence rates were reported in Zimbabwe (15.3%) 27 and Nigeria (17.7%), 28 while higher prevalence was observed in studies from southern Ethiopia (51.3%), 18 Tanzania (57.8%), 29 and Cambodia (47.8%). 30 These discrepancies could be explained by disparities in the study groups’ sociodemographic traits, including age distribution and lifestyle choices. Furthermore, disparities in healthcare access, diagnostic criteria, and regional disease burden could contribute to the observed differences in NCD prevalence.
The present study found a magnitude of hypertension of 7.0% among adult PLHIV in the region. Higher prevalence rates have been documented in eastern Ethiopia (23%), 31 Nigeria (15.5%), 28 Uganda (29%), 32 South Africa (34.6%), 33 and Ghana (36.9%). 34 The observed differences in hypertension prevalence across studies may be attributed to several factors, including variations in socioeconomic and demographic characteristics, lifestyle behaviors, and dietary patterns of the study populations. Moreover, differences in sample size, study settings, and study periods may have contributed to the observed discrepancies.
This study presented 5.7% adult PLHIV were affected by diabetes mellitus. Our findings align with findings from southwest Ethiopia (6.4%), 35 Uganda (4.7%), 25 Zimbabwe (6.9%), 36 and Ghana (7.4%). 37 However, higher prevalence rates were documented in northeast Ethiopia (8.8%), 38 and Vietnam (9.2%). 39 The observed variations likely reflect differences in ART regimens, particularly the use of protease inhibitors versus newer integrase strand transfer inhibitors; diagnostic methodologies; population characteristics, including age distribution and settlement type variation; and exercise and diet related factors.
Our study found that 4.8% of participants were affected by cardiovascular diseases
This study found a 4% magnitude of cancer among adult PLHIV attending ART clinics in the Sidama Region, closely aligning with reports from southern Ethiopia (3.9%) 18 but exceeding estimates from Zimbabwe (1.9%). 43 The similarity with southern Ethiopia may reflect comparable diagnostic capacity and oncogenic risk factors, while the discrepancy with Zimbabwe could be attributed to differences in cancer screening protocols, ART regimen composition, or environmental exposure to carcinogens.
This study presented a 3.3% prevalence of chronic respiratory disease among adult PLHIV in the region. Higher prevalence rates were reported in southern Ethiopia (12%) 18 and Uganda (15.5%). 44 The Ugandan study assessed the prevalence of CRD across all PLHIV, but our investigation concentrated exclusively on PLHIV receiving ART at general hospitals. This could be the reason for the disparity with the Ugandan research. Furthermore, it is probable that the observed heterogeneity results from environmental triggers that are unique to each nation as well as variations in diagnostic protocols.
According to this study, the likelihood of acquiring NCDs increased considerably with each unit increase in body mass index. Studies from northern Ethiopia, 45 eastern Ethiopia, 46 Vietnam, 39 Iran, 47 Tanzania, 48 and Uganda 49 presented comparable results. Higher BMI was significantly associated with NCDs, likely because overweight and obesity promote chronic inflammation, insulin resistance, and metabolic dysfunction—accelerating conditions like diabetes, hypertension, and cardiovascular disease. Overweight or obesity aggravates ART-linked metabolic dysfunction and immune activation, heightening NCD risks
Our study found a significant association between abnormal/elevated waist circumference and the presence of NCDs. Adult PLHIV with elevated waist circumference had three times higher odds of developing NCDs. This finding aligns with studies from Tanzania, 19 likely due to the central role of abdominal obesity in metabolic dysregulation, insulin resistance, and systemic inflammation. This association is true across several groups because excess visceral fat is linked to hypertension, dyslipidaemia, and glucose intolerance—all of which are major risk factors for NCDs.
Aging emerged as a significantly associated factor with NCDs among adult PLHIV in our study. PLHIV aged 40 years and above had about two times higher odds of developing NCDs compared to younger individuals. Studies from Ethiopia 18 and resource limited settings25,27,40,50 reported comparable findings. The combined impacts of long-term ART metabolic side effects, HIV-related chronic inflammation, and normal physiological ageing are probably responsible for the rising incidence of NCDs with ageing. These factors contribute to the presence of conditions such as cardiovascular diseases, diabetes, and hypertension, a trend observed across diverse settings.
The presence of NCDs in adult PLHIV was found to be strongly associated with opportunistic infections (OIs) in our study. Compared to people without recurring OIs, individuals with these infections had a threefold increased risk of developing NCDs. This finding aligns with a study from Uganda. 25 The course of cardiometabolic and pulmonary diseases in this population is accelerated by OI-induced chronic inflammation, immunological dysregulation, and metabolic dysfunction, all of which are likely to be reflected in this association.
The odds of developing NCDs varied between urban and rural areas, as our study found that PLHIV living in urban areas had 4.50-fold increased odds of getting NCDs in comparison to those living in rural areas. This urban preponderance is consistent with research from Uganda, 25 Tanzania, 48 Iran, 47 and Vietnam. 39 Stress-related physiological dysregulation linked to urban living, dietary trends towards processed foods, and increased exposure to sedentary lifestyles could all be contributing factors to the consistent pattern across many contexts.
Limitation of the Study
This study leveraged a large, comprehensive dataset and employed random sampling to ensure representativeness in identifying associated factors of NCDs among adult PLHIV. However, its cross-sectional design limits causal inference. Moreover, reliance on self-reported data introduces potential recall bias, and unmeasured confounders (CD4 count, viral load, lipid profile, and ART regimen) may have influenced the observed associations.
Conclusion
This study identified a high prevalence of NCDs among adult PLHIV in the region, with multimorbidity observed in 3.8% of patients. The most common NCDs included hypertension, diabetes mellitus, cardiovascular diseases, cancers, and chronic respiratory diseases. Associated factors of NCDs among adult PLHIV were older age, urban residence, opportunistic infections, overweight/obesity, and abnormal waist circumference.
Recommendation
To reduce the burden of NCDs among adult PLHIV, integrating ART with NCD screening services and strengthening monitoring systems for early diagnosis and treatment are essential. Targeted lifestyle interventions—such as nutritional counseling, regular physical activity, and routine weight monitoring—can lower obesity risks, a key driver of NCDs. Moreover, longitudinal studies are needed to establish causal relationships between risk factors and NCDs and to better characterize the comorbidity burden in this population.
Supplemental Material
sj-pdf-1-jia-10.1177_23259582261444518 - Supplemental material for Magnitude of Noncommunicable Diseases and Associated Factors among Adult People Living with HIV Attending ART Clinics of General Hospitals in Sidama Region, Ethiopia
Supplemental material, sj-pdf-1-jia-10.1177_23259582261444518 for Magnitude of Noncommunicable Diseases and Associated Factors among Adult People Living with HIV Attending ART Clinics of General Hospitals in Sidama Region, Ethiopia by Amelo Bolka, Frehiwot Mesfin and Selamawit Sikuare in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-2-jia-10.1177_23259582261444518 - Supplemental material for Magnitude of Noncommunicable Diseases and Associated Factors among Adult People Living with HIV Attending ART Clinics of General Hospitals in Sidama Region, Ethiopia
Supplemental material, sj-pdf-2-jia-10.1177_23259582261444518 for Magnitude of Noncommunicable Diseases and Associated Factors among Adult People Living with HIV Attending ART Clinics of General Hospitals in Sidama Region, Ethiopia by Amelo Bolka, Frehiwot Mesfin and Selamawit Sikuare in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Abbreviations
Acknowledgments
We gratefully acknowledge Yirgalem Hospital Medical College for granting permission to conduct this research. Our sincere appreciation extends to the Chief Executive Officers of all participating general hospitals. We are deeply thankful to the study participants for their time and cooperation, as well as to the dedicated data collectors and supervisors whose efforts were instrumental to this study's success.
Ethical Considerations
This study followed the ethical principles outlined in the Declaration of Helsinki for medical research involving human subjects. Ethical approval was obtained from the Institutional Review Board (IRB) of Yirgalem Hospital Medical College (Protocol Number: IRB/070/23, December 4, 2023). Written informed consent was obtained from all participants after a comprehensive explanation of the study's objectives. Participant confidentiality was maintained using pseudonymous codes.
Authors’ Contribution
Study conceptualization: Amelo Bolka. Data curation: Frehiwot Mesfin. Formal analysis: Frehiwot Mesfin, Selamawit Sikuare, and Amelo Bolka. Investigation: Frehiwot Mesfin, Selamawit Sikuare. Methodology: Frehiwot Mesfin, Selamawit Sikuare, and Amelo Bolka. Software: Selamawit Sikuare and Amelo Bolka. Supervision: Amelo Bolka B. Validation: Frehiwot Mesfin and Selamawit Sikuare. Writing—Frehiwot Mesfin and Selamawit Sikuare. Review and editing: Frehiwot Mesfin, Selamawit Sikuare, and Amelo Bolka B.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interests
The authors declare no conflicts of interest regarding the research, authorship, or publication of this article.
Availability of Data
The materials and data utilized in this study are not publicly available due to institutional regulation but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.