
Abstract
Background
Late diagnosis of HIV remains a critical barrier to effective treatment and improved long-term outcomes. Individuals presenting with low CD4+ T cell counts at diagnosis are at greater risk for opportunistic infections, hospitalization, and mortality. This study aimed to compare clinical, immunological, and virological outcomes among early and late presenters, and to identify factors associated with virologic failure.
Methods
We conducted a retrospective cohort study of 200 patients newly diagnosed with HIV between 2012 and 2019. Participants were categorized into three diagnostic groups based on baseline CD4+ T cell counts: early diagnosis (>350 cells/mm3), late diagnosis 1 (200-350 cells/mm3), and late diagnosis 2 (<200 cells/mm3). Baseline demographics, laboratory markers, clinical outcomes, and treatment responses were compared. Logistic regression was used to evaluate predictors of virologic failure at 6 months.
Results
Late presenters accounted for 71% of the cohort and were more likely to be older, female, unmarried, and have lower education levels. They exhibited significantly lower CD4+ counts, CD4/CD8 ratios, and higher HIV RNA levels at diagnosis (P < .001). Opportunistic infections, hospitalization, and mortality were significantly more common in the late diagnosis 2 group (P < .001). Although virologic suppression was achieved in most patients, immune recovery was significantly impaired in those diagnosed late. Antiretroviral therapy (ART) initiation after 2015 was independently associated with lower risk of virologic failure (OR: 0.39; P = .039).
Conclusion
Late HIV diagnosis is associated with increased clinical morbidity and impaired immune reconstitution, even in virologically suppressed individuals. Early detection, prompt ART initiation, and routine CD4/CD8 monitoring are essential to optimize outcomes. Public health interventions targeting social determinants may help reduce delays in diagnosis and improve equity in HIV care.
Plain Language Summary
Human immunodeficiency virus (HIV) is a virus that attacks the body’s immune system, making it harder to fight off infections and diseases. If HIV is not diagnosed and treated early, it can cause serious health problems. This study looked at medical records of people living with HIV in Turkey to find out how the timing of diagnosis affects their recovery and overall health. We compared people who were diagnosed early with those diagnosed late. The results showed that people who were diagnosed late had more advanced disease and weaker immune systems when they started treatment. Even after beginning HIV medications, their immune systems recovered more slowly. They were also more likely to have serious infections, need hospital care, and experience other health complications. Our findings show that early HIV testing and diagnosis are very important. When HIV is caught early, treatment can begin sooner, helping the immune system recover more effectively and leading to better health outcomes. This study highlights the need for public awareness about HIV and the importance of routine testing, especially for people at higher risk. Making testing easier and reducing stigma around HIV can encourage more people to get tested early and start.
Introduction
Despite major advances in antiretroviral therapy (ART), late diagnosis of HIV infection continues to pose significant challenges to individual and public health. Globally, a substantial proportion of people living with HIV are diagnosed at advanced stages of infection, often with CD4+ T cell counts below 350 cells/mm3 or even 200 cells/mm3. Such delayed presentation not only increases the risk of opportunistic infections (OIs) and AIDS-related mortality but also undermines the benefits of modern ART regimens.1,2
Late presentation is a multifactorial issue influenced by individual, societal, and structural barriers. In Turkey, the number of newly diagnosed HIV infections has steadily increased over the past decade, with a growing proportion of patients presenting at advanced stages. According to national surveillance data, approximately 55% to 60% of new diagnoses occur with CD4 counts below 350 cells/mm3, indicating persistent delays in testing and linkage to care. 3 Socioeconomic disadvantage, lower education level, limited access to testing, and stigma are all recognized contributors to diagnostic delay.4,5 Furthermore, differences in gender, age, and transmission route may also affect the likelihood of timely diagnosis. Addressing these disparities requires a comprehensive understanding of the clinical and demographic profiles of late presenters.6,7
Immunologic markers such as CD4+ and CD8+ T cell counts and the CD4/CD8 ratio provide valuable insights into disease progression and treatment response. Although ART is highly effective in achieving virologic suppression, immune restoration is often incomplete in patients who initiate treatment at advanced stages. This persistent immune dysfunction is associated with increased risk of non-AIDS events and long-term complications.8,9
Materials and Methods
This retrospective cohort study included 200 patients diagnosed with HIV at İzmir Tepecik Training and Research Hospital, a tertiary-level referral center in Western Turkey, between January 2012 and December 2019. Eligible participants were adults who received ART for at least 12 months and had complete clinical and laboratory follow-up data. Exclusion criteria included patients younger than 18 years, those who did not initiate ART, patients with incomplete baseline or follow-up data, and individuals with concurrent malignancy or immunosuppressive therapy that could affect immune parameters. Patients were classified into three diagnostic groups according to their baseline CD4+ T cell count: early diagnosis (CD4 > 350 cells/mm3), late diagnosis 1 (CD4 200-350 cells/mm3), and late diagnosis 2 (CD4 < 200 cells/mm3). Sample size justification: As this was a retrospective study including all eligible patients diagnosed and followed during the study period, no formal sample size or power calculation was performed. The final cohort size (n = 200) reflects all cases meeting the inclusion criteria between January 2012 and December 2019.
Demographic characteristics (age, sex, marital status, education level), transmission route, and laboratory data (CD4/CD8 T cell counts, HIV RNA levels, lipid profile, and liver function tests) were collected retrospectively from electronic medical records. CD4 and CD8 lymphocyte counts were determined by flow cytometry, and plasma HIV RNA levels were measured by real-time polymerase chain reaction. Laboratory assessments were recorded at baseline, 6 months, and 12 months following ART initiation.
In addition to the diagnostic classification based on baseline CD4+ T-cell counts, a treatment-based subgroup analysis was also performed. For this purpose, antiretroviral regimens were categorized according to the inclusion of an integrase strand transfer inhibitor (INSTI). Patients receiving dolutegravir, elvitegravir, or raltegravir were grouped as INSTI, while those treated with non-INSTI regimens (efavirenz-, nevirapine-, or protease inhibitor-based combinations) were grouped as non-INSTI. INSTI-based regimens became the predominant first-line therapy after 2015 in our center.
Clinical outcomes included incidence of OIs, hospitalizations, mortality, and changes in CD4/CD8 ratios. Virologic suppression was defined as plasma HIV RNA <50 copies/mL at 6 months. Virologic failure was defined as HIV RNA >200 copies/mL.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation or median with interquartile range, depending on distribution. Normality was assessed using the Kolmogorov–Smirnov test. The Kruskal–Wallis test or one-way analysis of variance was used for comparisons across diagnostic groups for continuous variables. Categorical variables were analyzed using Pearson's chi-square test or Fisher's exact test. For two-group comparisons (eg, by virological status or treatment type), Mann–Whitney U or Student's t-test was used for continuous variables, and chi-square or Fisher's exact test for categorical variables. Univariate logistic regression analysis was used to identify predictors of virologic failure. Odds ratios (OR) with 95% confidence intervals were reported. A two-tailed P value <.05 was considered statistically significant.
Results
Study Flow
A total of 236 patients diagnosed with HIV infection between January 2012 and December 2019 were initially screened. Thirty-six were excluded due to incomplete baseline or follow-up data, leaving 200 patients in the final analysis. The study flow and classification into diagnostic groups are illustrated in Figure 1.

Study flow chart.
In this study, we aimed to compare clinical outcomes, immunologic parameters, and virologic responses between early and late presenters. We also sought to identify predictors of virologic failure and explore the impact of treatment initiation timing and regimen on patient outcomes. By elucidating the clinical significance of late presentation, we hope to inform public health strategies and improve care for people living with HIV.
Demographic and Clinical Characteristics
The mean age of the patients was 40.4 ± 12.5 years, and 88% were male. The proportion of married individuals was 54%, and the most common educational level was primary to middle school graduation (58.5%). Heterosexual transmission accounted for 52.5% of cases, while homosexual transmission accounted for 32.5%. Late diagnosis was more frequently observed among patients with older age, lower educational level, and unmarried status, suggesting a possible association with social determinants of delayed presentation
As shown in Table 1, late diagnosis was significantly associated with older age (P < .001), being unmarried (P = .004), and having education limited to middle school (P < .001). Heterosexual transmission was more frequent in the late diagnosis group (P = .02), while homosexual transmission was more common in the early diagnosis group (P < .001).
Baseline Demographic and Epidemiologic Characteristics of the Study Population by Diagnostic Group.
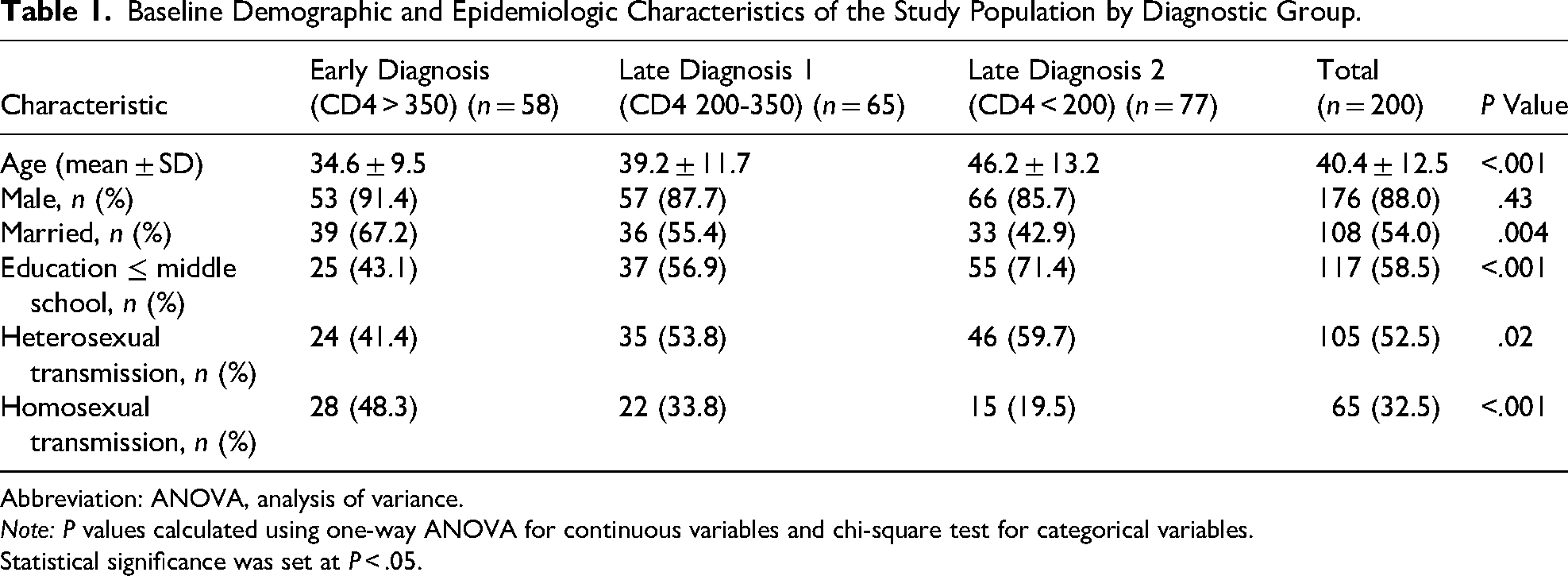
Abbreviation: ANOVA, analysis of variance.
Note: P values calculated using one-way ANOVA for continuous variables and chi-square test for categorical variables.
Statistical significance was set at P < .05.
Baseline Laboratory Findings
At baseline, the early diagnosis group had significantly higher CD4+ and CD8+ T lymphocyte counts, CD4 percentage, and CD4/CD8 ratio, and lower HIV RNA levels and CD8 percentage (P < .001). Late diagnosis 2 (CD4 < 200 cells/mm3) showed marked immunosuppression and high viremia.
CD8+ T cell counts showed a declining trend in the early diagnosis group, while they remained elevated in the late diagnosis groups throughout the 12-month follow-up. This difference was not statistically significant in the posttreatment period (Table 2). Table 2 summarizes the laboratory parameters at baseline, sixth, and 12th months across diagnostic groups.
Laboratory Parameters at Baseline, Sixth, and 12th Months by Diagnostic Group.

Note: P values were calculated using Kruskal–Wallis test for continuous variables and chi-square test for categorical comparisons.
Statistical significance was set at P < .05.
Opportunistic Infections
The overall rate of OIs was 11%, rising to 14% in the late diagnosis group. The most common OIs were esophageal candidiasis (33.9%) and Pneumocystis jirovecii pneumonia (28.5%). The vast majority of OIs occurred in individuals with CD4 < 200 cells/mm3 (P < .001). As detailed in Table 3, rates of OIs increased progressively from 3.4% in early diagnosis to 19.5% in late diagnosis 2 (P < .001). Similarly, hospitalization and mortality rates were significantly higher in the late diagnosis groups (P < .001 and P = .002, respectively).
Clinical Outcomes at 12 Months by Diagnostic Group.

Note: P values were calculated using chi-square test for categorical outcomes.
Statistical significance was set at P < .05.
These results indicate that patients diagnosed in the late stage, especially those with CD4 counts below 200 cells/mm3, had significantly higher rates of OIs, hospitalizations, and mortality within the first year of ART. Early diagnosis was clearly associated with better clinical outcomes.
Virologic Response
By the sixth month of ART, 85.5% of the cohort had HIV RNA <50 copies/mL. This rate was 89.6% in the early diagnosis group and 77.1% in the late diagnosis group (P = .037). Virologic failure (HIV RNA >200 copies/mL) was significantly more common in the late diagnosis group (9.9% vs 2.6%, P = .032). Late diagnosis 2 patients began treatment with higher baseline viral loads and had the highest rate of uncontrolled viremia at month 6 (P = .004). Furthermore, the trend of virologic suppression over the 12-month follow-up period is illustrated in Figure 2. Virologic suppression increased progressively across all diagnostic groups, with the early-diagnosis group achieving the highest suppression rates at each time point.

Virologic suppression over time by diagnostic group.
These comparisons support findings from the logistic regression model and further illustrate the clinical profile of patients with suboptimal virologic response. The variables in Table 4, particularly those with clinical or statistical significance, were used in constructing the logistic regression model shown in Table 5.
Comparison of Patients With and Without Virologic Suppression at 6 Months.

Abbreviation: ART, antiretroviral therapy.
Note: P values calculated using appropriate tests (eg, Mann–Whitney U for medians, chi-square for categorical data).
Statistical significance was set at P < .05.
Factors Associated With Virologic Failure at 6 Months (Univariate Logistic Regression).
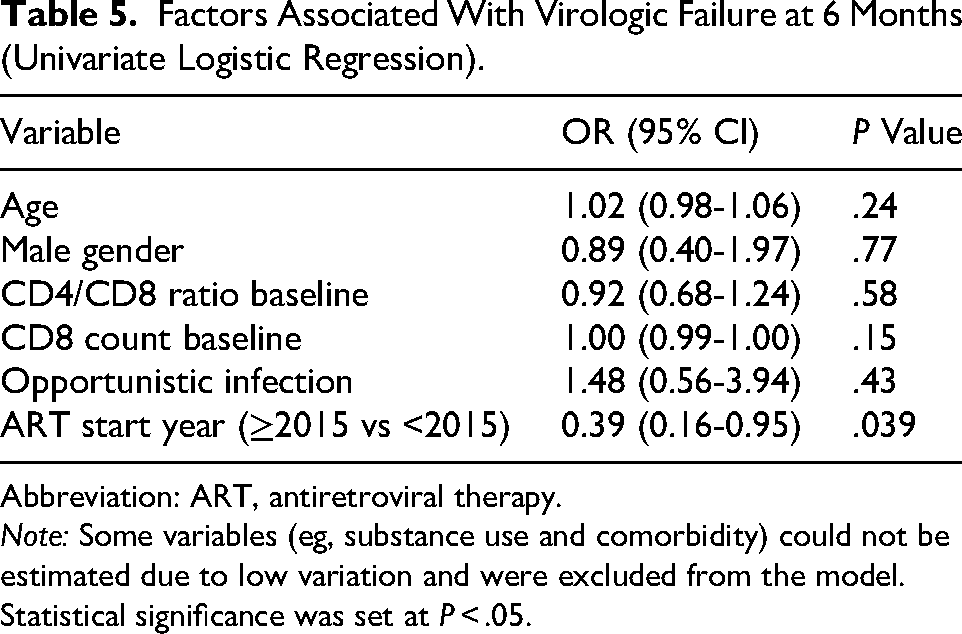
Abbreviation: ART, antiretroviral therapy.
Note: Some variables (eg, substance use and comorbidity) could not be estimated due to low variation and were excluded from the model.
Statistical significance was set at P < .05.
As shown in Table 4, patients without virologic suppression at 6 months had significantly lower baseline CD4 count (183 vs 341; P = .014), lower CD4/CD8 ratio (0.34 vs 0.54; P = .042), and a higher incidence of OIs (38.5% vs 11.1%; P = .011).
A multivariate logistic regression model was constructed including variables with univariate significance; however, due to the limited number of virologic failure events and low variation in some predictors (eg, comorbidities, substance use), reliable coefficient estimation was not possible, and no statistically significant predictors were identified.
In the univariate analysis, later calendar year of treatment initiation (2015 or later) was associated with a lower risk of virologic failure (P = .039). Therefore, only univariate results are presented in Table 5.
As seen in Table 5, among the univariate predictors of virologic failure, only ART initiation in or after 2015 was significantly protective (OR: 0.39; P = .039), supporting the role of improved regimens in recent years.
Immunologic Response
CD4+ T cell counts increased significantly in all groups. However, late diagnosis patients, particularly late diagnosis 2, failed to reach CD4 > 500 cells/mm3 by month 12. The median CD4 count at 12 months was 783 cells/mm3 in the early group versus 454 cells/mm3 in the late group (P < .001). Figure 3 shows the trend in CD4+ T cell recovery over time, illustrating the persistent gap between early and late diagnosis groups.

Median CD4+ T cell counts over time by diagnostic group. Note: CD4+ T cell counts increased in all groups during the 12-month follow-up, with persistently lower recovery in late presenters, especially those with CD4 < 200 cells/mm3.
CD4/CD8 ratios increased but did not normalize (>1) in any group. As shown in Table 2, CD4/CD8 ratio significantly increased in all groups but remained subnormal in late diagnosis groups, especially late diagnosis 2, which failed to reach a ratio >0.5 at month 12 (P < .001).
Regression models attempting to predict 12-month CD4 > 500 cells/mm3 outcomes demonstrated that certain patient groups could not be reliably estimated, reflecting the strong immunologic benefit of early diagnosis and methodological limits of the model.
CD8 T Cell Dynamics
CD8+ T cell counts decreased during treatment in the early diagnosis group, while increasing in late diagnosis groups. This difference was not statistically significant in posttreatment periods.
Biochemical Parameters
Baseline alanine aminotransferase (ALT), cholesterol, low-density lipoprotein (LDL), and high-density lipoprotein (HDL) levels were higher in the early group. HDL was significantly lower in the late group patients (P < .001). Posttreatment, HDL levels improved in all groups but remained lowest in late diagnosis 2.
Bone Mineral Density
Bone mineral density (BMD) abnormalities were more common in the late diagnosis group, although the difference was not statistically significant.
Treatment Initiation Timeline and Regimen Changes
Among 65 patients diagnosed before 2015, 75% initiated ART within 60 days. The median time to treatment initiation was 0 days in both pre- and post-2015 periods, indicating adherence to guideline recommendations. Although the difference in the 75th percentile of initiation time between the two periods was not statistically significant, it suggested a trend toward earlier ART initiation in recent years, with the 75th percentile decreasing from 60 days before 2015 to 30 days after 2015.
Patients diagnosed between 2012 and 2015 were more likely to receive non-nucleoside reverse transcriptase inhibitor (NNRTI)-based (especially efavirenz) or limited protease inhibitor (PI)-containing regimens. After 2015, most patients (121 of 135, 89.6%) received INSTI-based combinations—most commonly dolutegravir (52.1%), followed by elvitegravir (43.0%) and raltegravir (4.9%). Virological failure at 6 months was lower among INSTI users than non-INSTI users, although this difference did not reach statistical significance (Table 6).
Immunological and Clinical Outcomes According to ART Regimen.
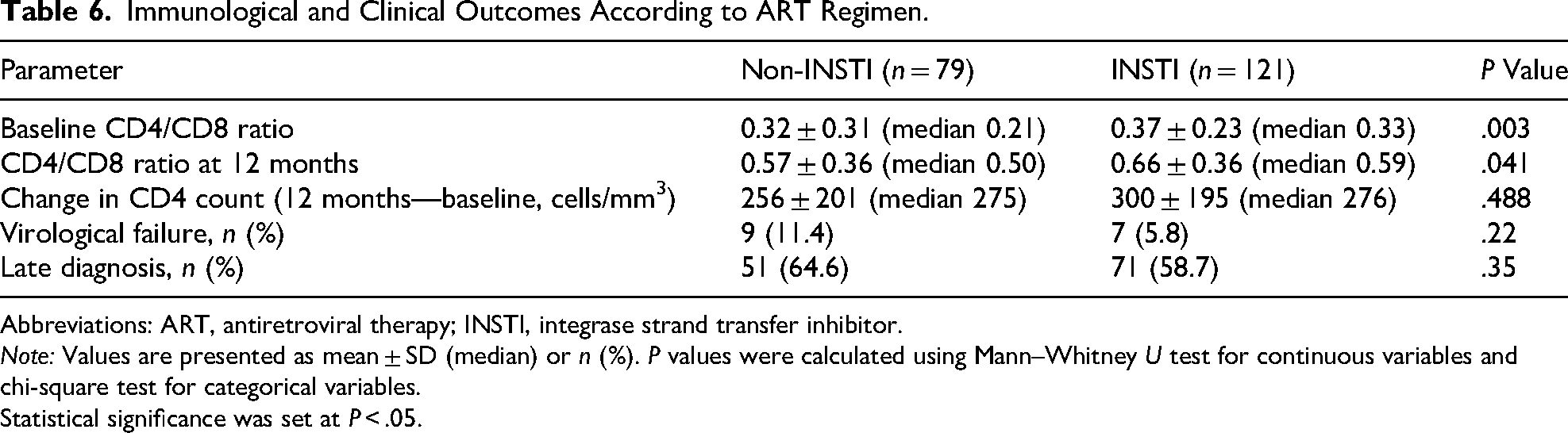
Abbreviations: ART, antiretroviral therapy; INSTI, integrase strand transfer inhibitor.
Note: Values are presented as mean ± SD (median) or n (%). P values were calculated using Mann–Whitney U test for continuous variables and chi-square test for categorical variables.
Statistical significance was set at P < .05.
The INSTI group demonstrated higher CD4/CD8 ratios both at baseline and at 12 months, indicating a more favorable immune reconstitution pattern (both P < .05). However, absolute CD4 gain did not differ significantly between groups (Table 6).
Mortality
Mortality occurred only in the late diagnosis group (5.5%). No deaths were recorded in the early diagnosis group (P < .001). Leading causes of death included Pneumocystis jirovecii pneumonia (PCP), toxoplasmosis, and Cytomegalovirus (CMV) infections. During follow-up, ART regimen changes were required in 82 patients, most commonly due to reduced BMD.
Discussion
This study investigated the clinical, immunological, and virological profiles of individuals newly diagnosed with HIV infection, with particular emphasis on the predictors and consequences of late presentation. In our cohort, 71% of individuals were classified as late presenters, a prevalence consistent with previously reported figures from various regions, particularly in middle-income settings. 10 This finding reinforces the persistent global challenge of delayed HIV diagnosis despite ongoing public health efforts.
Lower educational status emerged as a significant predictor of late presentation. Individuals with limited formal education were significantly more likely to be diagnosed at advanced stages of infection, aligning with international evidence suggesting that lower health literacy and socioeconomic disadvantage are major barriers to early testing and care engagement. 11 While male patients comprised the majority of the cohort, female patients were overrepresented among late presenters, a pattern observed in other regional studies. 12 These disparities emphasize the need for gender-sensitive and equity-focused approaches in HIV screening strategies. 13
Late presenters exhibited significantly lower CD4+ T cell counts and CD4/CD8 ratios and higher HIV RNA levels at diagnosis, confirming more advanced immunosuppression. These laboratory markers are well-established prognostic indicators and strongly predict the risk of OIs, morbidity, and mortality. 14 In our cohort, OIs such as P. jirovecii pneumonia and esophageal candidiasis were more frequently observed among patients with lower CD4+ counts, particularly in the advanced late presentation subgroup (CD4 < 200/mm3). 15 Mortality was observed exclusively among late presenters (5.5%), with leading causes of death including PCP, CMV infection, and toxoplasmosis. Notably, hospitalization rates also followed a similar trend, with a significant increase observed among late presenters, particularly in those with CD4 counts <200 cells/mm3. This suggests a substantial burden of HIV-related morbidity in patients diagnosed at advanced stages. 15 These findings highlight the clinical consequences of severe immunosuppression at the time of diagnosis.
Hypocholesterolemia, particularly reduced HDL levels, was also significantly associated with late presentation. This metabolic profile may reflect underlying systemic inflammation, malnutrition, or advanced HIV-related immune activation. 16 In addition, early presenters exhibited significantly higher baseline ALT, LDL, and total cholesterol levels. These biochemical differences may further reflect varying degrees of systemic inflammation and nutritional status at the time of diagnosis, although their clinical significance warrants further investigation.
Despite these unfavorable baseline features, both early and late presenters demonstrated virological suppression and CD4+ recovery at 12 months post-ART initiation. However, immune reconstitution was significantly less pronounced among late presenters, especially those with CD4 < 200/mm3. These individuals had the lowest CD4/CD8 ratios at baseline and at 12 months, consistent with persistent immune dysregulation despite viral suppression.17,18 While most individuals in the early diagnosis group achieved CD4+ counts above 500 cells/mm3 by month 12, the majority of late presenters, particularly those with CD4 < 200 cells/mm3, failed to reach this threshold. This underscores the limited regenerative capacity of the immune system when treatment is initiated at an advanced stage. 19
The CD4/CD8 ratio, while not an independent predictor of virologic failure in our regression model, remains a relevant immunologic marker. In our cohort, individuals with elevated CD8+ counts and persistently low CD4/CD8 ratios showed attenuated immunologic recovery. The persistent elevation of CD8+ T cell counts and subnormal CD4/CD8 ratios in late presenters may reflect ongoing immune activation and immunosenescence, even after virologic suppression. This pattern is consistent with previous studies linking high CD8 counts to chronic inflammation and poor immune restoration.20,21 Therefore, routine CD4/CD8 monitoring may offer additional prognostic value beyond traditional CD4 counts in the long-term management of HIV infection. Treatment initiation timing and regimen selection were additional factors influencing outcomes. Although the median time to ART initiation was 0 days in both pre- and post-2015 periods, the 75th percentile decreased from 60 to 30 days, suggesting improved adherence to early ART guidelines. Patients initiating ART after 2015 were significantly less likely to experience virologic failure (P = .039), likely reflecting the widespread adoption of INSTI-based regimens. After 2015, INSTI-based regimens became more widely used. In a subgroup analysis, patients receiving these regimens showed a significantly greater increase in CD4/CD8 ratio at 12 months (P = .041), supporting a more favorable immune reconstitution pattern with INSTI-based regimens. 22 This observation is consistent with previous studies reporting favorable immune restoration profiles with INSTI-based combinations. At the cohort level, patients who failed to achieve virologic suppression at 6 months were characterized by significantly lower baseline CD4 counts, lower CD4/CD8 ratios, and higher rates of OIs. These findings indicate a complex immunovirological profile associated with suboptimal ART response and reinforce the need for close monitoring and individualized care in such patients. 23
BMD abnormalities, although not significantly different across diagnostic groups, were the most common reason for ART regimen change, affecting 82 patients. These findings highlight the need for routine metabolic monitoring, especially in late presenters, who may be at higher risk for ART-related complications.
While an exploratory analysis stratifying CD4/CD8 ratio using a <0.3 cut-off did not yield statistically significant findings, the consistently poor immune recovery in patients below this threshold supports its continued utility as a monitoring tool. Attempts to predict CD4 > 500 cells/mm3 at 12 months using regression analysis were limited by baseline immune status: most early presenters reached this threshold, whereas few late presenters did. This modeling limitation emphasizes the strong prognostic value of early immune status.
This study has several limitations. First, its retrospective design may introduce selection bias and restrict causal inference. Second, the regression model excluded certain variables, such as substance use and comorbidities, due to low variability. Third, although CD4/CD8 ratio was analyzed as a prognostic marker, the lack of a universally accepted threshold limits its clinical applicability. Despite these limitations, the study offers valuable insights into the consequences of delayed HIV diagnosis.
Conclusion
In conclusion, this study reinforces the prognostic importance of early HIV diagnosis and timely ART. While virologic suppression was achieved in most individuals, those presenting with advanced immunosuppression experienced compromised immune recovery, particularly in terms of CD4/CD8 ratio normalization and mortality risk. Educational level and female sex were associated with delayed diagnosis, emphasizing the need for targeted public health strategies. Moreover, earlier ART initiation and the use of modern regimens have improved virologic outcomes. These findings support continued expansion of early testing, social determinant-focused outreach, and long-term immunologic monitoring to improve outcomes for people living with HIV.
Routine assessment of CD4/CD8 ratios may enhance prognostic stratification and inform tailored long-term management approaches even in virologically suppressed individuals.
Highlights
Over half of patients were diagnosed with HIV at an advanced disease stage. Late presenters had slower immune recovery despite viral suppression. Low CD4/CD8 ratio persisted, indicating immune dysregulation. Delayed diagnosis increased mortality and opportunistic infections. Early testing and rapid ART initiation remain critical for better outcomes.
Footnotes
Acknowledgments
The authors would like to thank the staff of the Infectious Diseases Department at the University of Health Sciences, Tepecik Training and Research Hospital, where the study was conducted, for their support during data collection and patient follow-up. This article is based on the medical specialty thesis of Dr Nadide Ergün, titled “Evaluation of Prognosis in Patients with Early and Late HIV Diagnosis,” conducted at the University of Health Sciences, Tepecik Training and Research Hospital, Izmir, Türkiye.
Ethical Considerations
This study was approved by the Ethics Committee of the University of Health Sciences, Tepecik Training and Research Hospital (Decision No: 2020/2-6, Date: January 2020), where the study was conducted.
Informed Consent/Patient Consent
The requirement for informed consent was waived by the Ethics Committee due to the retrospective design of the study.
Author Contributions
NE designed the study, collected and analyzed the data, and drafted the manuscript. GE supervised the study and revised the manuscript critically for important intellectual content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.