
Abstract
Objectives
Preexposure prophylaxis (PrEP) uptake among young sexual minority men of color remains low. Tailored motivational interviewing (TMI) has been shown to promote behavior change across the youth HIV prevention and care continua but has not been tested in PrEP. This study tested the proof of concept of the TMI for PrEP Choices (TMI-PC) implementation package among a cohort of providers.
Methods
This included: (1) online modules (2) TMI workshop; and (3) Motivational Interviewing (MI) technique practice and feedback. Providers completed surveys prior to and posttraining and 2 coded standard patient interactions; one following the workshop and one three months after the workshop.
Results
At baseline, providers reported high familiarity and confidence with PrEP overall and daily oral PrEP. On-demand and injectable PrEP familiarity increased significantly among providers. Immediately posttraining, half of the providers scored in the intermediate or advanced fidelity range, which increased to 75% at follow-up. Change in mean MI coach rating scale scores among providers increased significantly.
Conclusion
This study provides proof of concept for the TMI-PC Implementation Package, which appears to be ready for testing in a randomized clinical trial.
Keywords
Introduction
Young sexual minority men (YSMM) continue to be the population most impacted by HIV in the United States. 1 Among all diagnosed HIV infections in 2022, 65% were sexual minority men (SMM). 2 Young people have the poorest outcomes along the HIV prevention and care continua, and the unique developmental challenges facing youth potentiate these outcomes. 3 Emerging adults are less likely to know their HIV status compared to older adults3,4 and least likely to link to and adhere to HIV treatment or biomedical prevention including preexposure prophylaxis (PrEP). 5 Racial and ethnic disparities persist in HIV diagnoses among SMM, with 37% of diagnoses among Black or African American (Black) SMM and 33% among Hispanic or Latino (Hispanic) SMM, compared with 24% among White SMM. 2
HIV can be prevented with the use of HIV PrEP, but U.S. data suggest that young people have the greatest unmet need for PrEP among all age groups 6 and young people of color may be most at risk for low PrEP uptake in the United States. 7 Thus, despite the substantial declines in HIV transmission achieved over the past decade, the full benefits of available tools and interventions have yet to be realized in YSMM, especially among YSMM of color. Providers’ limited knowledge of PrEP and Centers for Disease Control (CDC) guidelines remains a challenge to increasing PrEP uptake. 8 PrEP education and support tools have been developed for provider and client use but have been underutilized.9–11 Providers who serve YSMM of color need resources to deliver tailored education, shared decision-making, and autonomy supportive communication to increase uptake of the growing array of PrEP options. 12 Motivational interviewing (MI) is an evidence-based framework for such communication, and CDC's compendium of HIV best practices include more than 25 named interventions with an MI component. 13 Yet, MI can be difficult to deliver with fidelity, as one study found that adolescent HIV providers had low levels of MI competence despite reporting having received some MI training. 13
MI is a method of communication designed to increase intrinsic motivation for behavioral change through communication microskills that convey autonomy support, reinforce motivational language, and support collaborative treatment planning. 14 Developmentally and culturally tailored MI for HIV-related behaviors (TMI) has been shown to promote behavior change across the youth HIV prevention and care continua.15,16 Implementation strategies to address provider fidelity to TMI have been shown to increase providers’ competency 15 and their clients’ health outcomes in a randomized stepped wedge trial of youth HIV treatment clinics, but TMI implementation has not yet been tested in PrEP providers. Furthermore, with the rapid rise of digital health innovations, TMI implementation strategies could be adapted to reduce clinician and implementer burden by replacing some live training components with digital health. Thus, the current study tested the proof of concept of the TMI for PrEP Choices (TMI-PC) blended implementation package on providers’ confidence around PrEP and providers’ TMI competence as part of a larger CDC initiative. 17
Methods
Following mixed methods formative process to adapt TMI-PC and design the online modules18,19 this study uses a pre–post survey design to evaluate proof of concept of the TMI-PC implementation package15,17 in improving provider confidence. Additionally, a posttest only evaluation of TMI competence used a standard patient interaction model to prepare for a full-scale implementation trial. Details of the methods are described below. The protocol was approved by the Institutional Review Boards of Florida State University (Approval No. 00003623). Providers completed written informed consent prior to completing study activities. Providers were compensated US$50 for completing the pretraining survey; US$50 for completing the posttraining survey, and first standard patient interaction; and US$50 for the 3-month postfeedback standard patient interaction.
Participants
From January 2024 to March 2024, we recruited PrEP providers from 7 participating clinic sites in the United States that already participated in the earlier formative work for this study. Prior to participation in this study, all clinics provided PrEP care. Four of the clinics specialize in care for adolescents and youth. We asked clinic representatives to provide contact information for any staff at their clinic who discussed PrEP with clients. We attempted to recruit all those providers we had contact information for. Thirty-one providers were enrolled that provided PrEP. Data collection began immediately following the first consent in January 2024 and concluded July 2024 when the last standard patient interaction was conducted. Eligibility criteria included being a PrEP provider at one of our participating sites, defined as any site staff member who discusses PrEP with clients. Each site provided a list of their PrEP providers for the study team to contact. All providers on the list of PrEP providers were contacted via email and sent a link to a brief screener. If providers screened eligible, they were sent a link for the electronic consent form. We prioritized enrollment of providers who had prescribing privileges to ensure that at least 50% of the provider sample could prescribe PrEP. If providers consented, they had to complete a contact information form and pretraining survey to be considered fully enrolled.
TMI-PC Implementation Package
TMI-PC implementation consisted of 3 strategies: online modules, live virtual workshop training, and coded feedback on 2 standard patient interactions. The first part of TMI-PC training included online PrEP training modules to educate providers on currently available PrEP options and communication strategies for discussing sexual health and PrEP options based on MI principles. These strategies feature tips on how to build rapport with clients including YSMM. The flexible and interactive modules were created using the Easygenerator online authoring tool, which allows learners to complete their assigned courses over multiple sessions at any time. The interactive features used throughout the modules are designed to keep providers engaged. Some of these features include checks for understanding, embedded videos, and links to external content. Each module also contains at least one case-based scenario. These scenarios were based on real-world interactions that study team providers experienced during interactions with clients. Case-based scenarios feature fictional YSMM clients who likely represent the clients providers encounter in their respective clinics.
The research team developed these modules using a variety of content sources including CDC produced guidelines and materials, research articles, and expert guidance. Examples of content sources included CDC's PrEP for the Prevention of HIV Infection in the United States—2021 Update: A Clinical Practice Guideline 9 to provide clinical guidance on PrEP initiation and follow-up; PrEP efficacy research articles to inform providers on the efficacy of the different PrEP modalities20–24; and CDC's A Guide to Taking a Sexual History 25 to provide recommendations on taking a sexual history for all clients. In addition to modules covering PrEP regimens, we also include modules on the need for PrEP; PrEP screening and start-up; postexposure prophylaxis (PEP); and PrEP adherence and persistence. The modules were refined to their final form through an iterative feedback process with subject matter experts within the EPICC team. Table 1 lists the titles and brief descriptions of each module.
Online PrEP training module titles and topics used in EPICC and mChoice.

Abbreviations: PEP, postexposure prophylaxis; PrEP, reexposure prophylaxis.
Following completion of the online PrEP training modules, providers received the TMI components (see Naar et al, 2019 26 for initial development). First, two 3-h live, virtual TMI training sessions led by a member of the MI network of trainers who had previously delivered TMI training. TMI-PC included distinct training modules: (1) introduction to TMI and PrEP choice; (2) TMI spirit, cultural humility, and stigma reduction; (3) managing counter change talk and discord with empathy and autonomy support; and (4) eliciting and motivation for PrEP. The training utilized videos of PrEP providers engaging with YSMM, which demonstrated TMI integrated with cultural humility. The videos were created specifically for this study with youth input. The workshops are structured with cooperative learning activities, video examples, and behavioral skills acquisition steps (modeling, verbal and behavioral rehearsal, feedback). 27 Following the training, providers received automated feedback with tailored video examples based on their MI competence in coded standard patient interactions (see below).
Data Collection
After consenting, providers completed a brief survey of demographics and 11 questions rated on a 5-point Likert scale prior to initiating the TMI-PC implementation package. Three items addressed MI familiarity, intentions and comfort, 4 items addressed familiarity with different PrEP formulations, and 4 items addressed confidence discussing different PrEP formulations with groups of people providers likely encounter in clinic. Then providers were sent a link to access the PrEP training modules. The study team monitored progress for course completion and overall course score on checks for understanding. After completing the PrEP training modules and TMI training, providers completed a posttraining survey similar to the survey completed prior to starting the TMI-PC training.
Providers were then scheduled for two standard patient interactions: one immediately after the TMI-PC workshop (see below) and another 3 months postworkshop. Standard patient interactions took place over the phone and involved a member of the study team acting as a client based on a predetermined scenario using real world examples from providers and developed with youth advisors. Providers were given basic background information about the scenario and client prior to beginning the scenario including name, age, race, gender, context of visit (PrEP initiation or follow-up), exposure/risk (eg, condomless sex with main partner), medications, and target behavior (eg, medication adherence). During the interaction, the provider attempted to use strategies gained from the TMI-PC package. Interactions typically lasted less than 30 min and were recorded to code for provider competence.
Upon completing the standard patient interaction, a member of the study team completed an Qualtrics based form for the MI Coach Rating Scale (MI-CRS) V3.1. 28 The MI-CRS provides coders with descriptions of provider interactions related to each potential score for all of the included MI competencies. Items 1 and 2, indicating empathy and collaboration respectively, were rated as global items based on coder overall impression and consistency of behavior demonstration. Items 4, 5, 8, 9, 11, 12, and 13 were rated according to competency fidelity, scoring one for none of the time, 2 for more not than often, 3 for more often than not, and 4 for most of the time. These items indicate competency in eliciting ideas and motivations for behavior change, balancing client agenda with focus on the target behavior, affirmations, summaries, solicitation of feedback, managing counter change talk, and cultural humility. The MI-CRS provides specific guidelines for items 3, 6, 7, and 10 which indicate provider competency in supporting client autonomy, use of reflective statements, strategic use of reflections, and use of open-ended questions respectively. Coders using the MI-CRS meet quarterly to enforce rating consistency.
Coder training included a minimum of 6 h of TMI training and 3 h of coding training. Subsequently, coders co-coded standard expert consensus recordings until they reach absolute agreement for 8 of 12 items and no more than one category discrepancy from the expert consensus. Coders attend a monthly coding lab to co-code sessions and discuss discrepancies. MI-CRS consists of 12 indicators of MI competency rated 1 to 4 representing beginner, novice, intermediate, and advanced competency. Overall scores indicate provider MI competency as Beginner (<2.0), Novice (≥2.0 to <2.6), Intermediate (≥2.6 to <3.3), or Advanced (≥3.3). An additional experimental rating in demonstrating cultural humility was reported but not integrated into overall provider score. Qualtrics outputs a feedback form with individual item scores, mean item scores and categories, and an algorithm-based list of the top 3 scores or “strengths” and the lowest 3 scores or “areas for improvement.” Video links for specific skill examples are embedded for each item. Although blind to condition is not possible in a single arm trial, raters were not aware of the timing of the workshop. Analyses addressed differences between the first MI-CRS (immediately postworkshop) and the second MI-CRS (after receiving one automated feedback report from the first rating).
Outcomes
The study included outcomes based on changes in MI familiarity; PrEP familiarity and confidence; and MI-CRS. MI familiarity was measured by 2 survey items compared prior to MI training and post-MI training. PrEP familiarity and confidence were measured by survey items compared prior to completing the PrEP modules and afterwards. Lastly, standard patient interactions were coded and scored. MI-CRSs were compared immediately posttraining and postfeedback.
Statistical Analysis
Scores for the pre- and postsurvey and for the postworkshop and postfeedback MI-CRS scores were evaluated for significance of difference using the nonparametric Wilcoxon signed-rank test for hypothesis testing of repeated measurements on a single sample. 29 With regard to overall competency on the MI-CRS, we combined Beginner and Novice into one group and Intermediate and Advanced into another group as Intermediate and above is considered the fidelity threshold. 27 Any providers who did not complete both pre- and postsurveys and both standard patient interactions were not included in the Wilcoxon signed-rank test calculation. The reporting of this study conforms to the Strengthening the reporting of observational studies in epidemiology statement for cohort studies (Supplemental File S3). 30
Results
We enrolled providers from 7 participating sites. Figure 1 includes a map of EPICC's participating sites.

EPICC participating sites.
The sample included 31 providers. A majority of providers were white (61.3%) and female (64.5%). Most providers were clinicians (74.2%), had previously prescribed PrEP (61.3%), and had been in their current position ≤ 5 years (74.2%). Table 2 describes the sample at baseline.
Sample description.
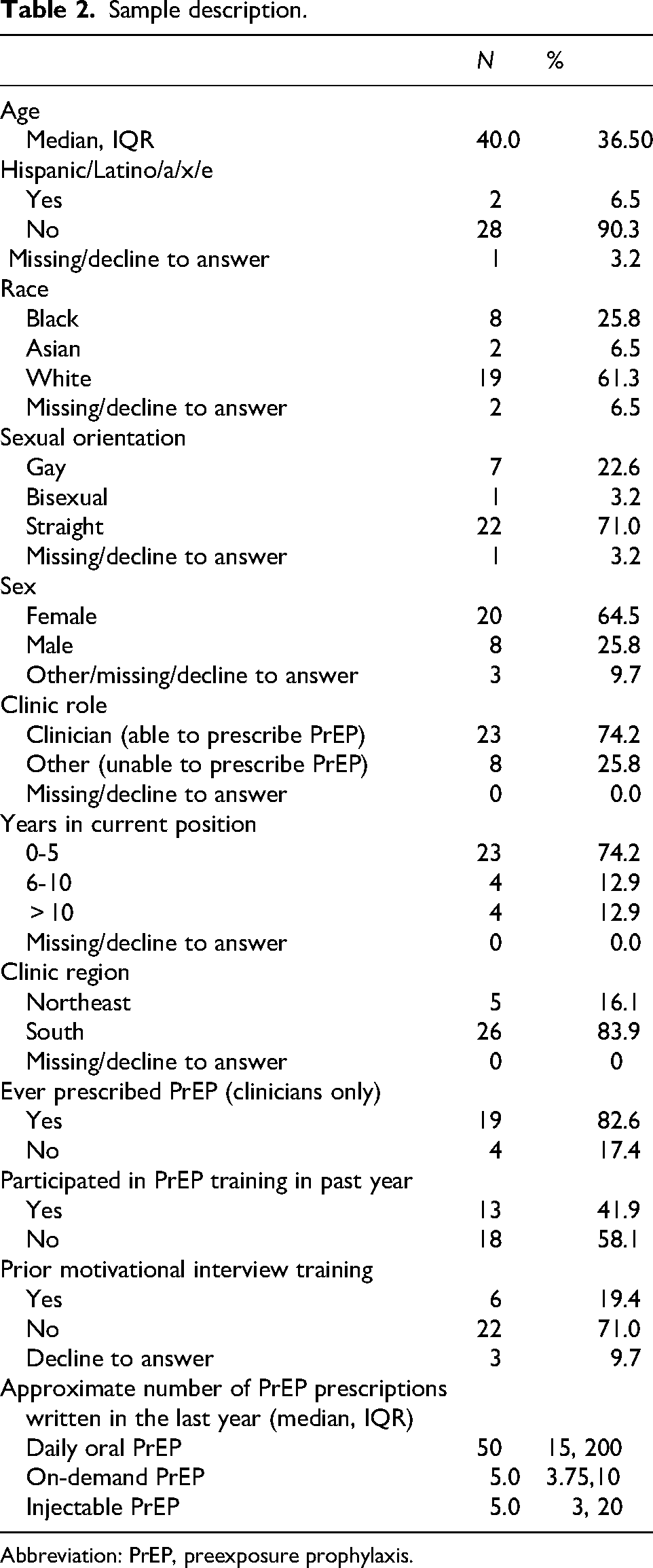
Abbreviation: PrEP, preexposure prophylaxis.
As Table 3 demonstrates, changes in use or planned use of MI and comfort using MI from pretraining to posttraining were all significant. The effect size for how often used or will use MI was large while the effect size for comfort using MI was medium.
MI familiarity changes prior to training and after training. How often used MI with clients (1 = always; 5 = never) and comfort using MI (1 = completely uncomfortable and 5 = completely comfortable).

As Table 4 demonstrates, familiarity with both on-demand and injectable PrEP increased significantly. Changes in confidence discussing PrEP generally and confidence discussing each type of PrEP were significant. All effects sizes were medium except for confidence discussing on-demand PrEP, which was large. Immediately posttraining, half the group scored in the fidelity range, and after the first feedback 75% of the group scored in the fidelity range (P = .016). Change in mean MI-CRS scores (from 2.62 to 3.01) was also significant (P < .001). We also examined changes in scores by item (see Table 5) to guide future training. Two items did not meet fidelity criteria after the first feedback: reflection: question ratio and summaries.
PrEP familiarity (1 = very unfamiliar; 5 = very familiar) and confidence discussing PrEP (1 = not at all confident; 5 = very confident).

Abbreviation: PrEP, reexposure prophylaxis.
Changes in MI-CRS scores by item.

Discussion
Given the evolving PrEP landscape and the increasing availability of new options and formulations, there is an urgent need for evidence-based tools and provider education to maximize PrEP uptake and adherence, particularly within community-based settings. This study provides proof of concept for the TMI-PC Implementation Package demonstrating significant and rapid improvements in both provider confidence in PrEP counseling and MI competence leveraging mobile health to reduce the number of face-to-face hours. Given the well-documented racial, ethnic, and age-related disparities in PrEP use, the TMI-PC implementation package sought to equip providers with evidence-based skills to facilitate client-centered discussions on PrEP decision-making while incorporating cultural humility and stigma-reduction approaches.
A striking finding of this study was that 50% of practitioners achieved MI fidelity after the initial workshop alone, a notable improvement over the original TMI study. 27 Further, 75% of providers reached fidelity after their first feedback session, underscoring the impact of structured, competency-based feedback in accelerating MI skill acquisition. These findings are particularly noteworthy as this is the first study to demonstrate such improvement through feedback only, without additional coaching interventions beyond the first session (significant difference, 75% fidelity and the mean was in the intermediate range). In addition to providing feedback regarding scores, there were also recommendations with tailored embedded video examples to highlight MI skills to improve competence. This varied from the EMEE study by Miller, 31 which did not see such success utilizing feedback on scores only. This improvement in provider skills underscores the value of structured, competency-based feedback with embedded modeling of skills to enhance MI proficiency. Additional factors that may have been instrumental in explaining meaningful gains includes the use of a blended learning approach, which combined interactive online modules, virtual MI training, along with structured and strategically placed feedback with youth developed video examples.
While most MI competency metrics showed significant improvement, reflection-to-question ratio (ideally 2:1) and using summaries effectively (ideally 2 per interaction) remained areas of limited progress. One possibility for this could be an overreliance on directive questioning styles. Some providers may naturally default to closed-ended questions when talking with clients about medication and/or treatment, such as discussing PrEP uptake, particularly when in time-limited clinical settings. Also, these 2 items rely on counts of instances of skills which may have been hard to achieve without coaching or boosters. While exploratory, these findings suggest that future MI training models should include additional practice sessions focused specifically on these skills.
Several key areas remain for future exploration. These include further analysis of the exploratory cultural humility item on the MI-CRS and evaluating the impact of the second feedback session. While this study assessed short-term competency gains, longitudinal follow-up evaluations could determine whether practitioner MI skills remain stable over time or require periodic reinforcement. A preworkshop assessment of skill would further demonstrate TMI-PC's success. This study did not include a sample size calculation as this is not atypical for proof of concept studies.
Conclusions
The changing PrEP landscape and the emergence of new options and formulations highlight the need for provider education and tailored tools to enhance PrEP uptake and adherence within diverse populations. This study provides preliminary evidence that TMI-PC is an effective implementation strategy enhancing provider MI competency and supporting PrEP decision-making in communities disproportionately affected by HIV. This study provides proof of concept of the TMI-PC implementation strategy enhancing provider MI competency and supporting PrEP decision-making in communities disproportionately affected by HIV.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251391273 - Supplemental material for Proof of Concept of the Tailored Motivational Interviewing for PrEP Choices Implementation Package for Providers to Support PrEP Uptake and Adherence Among Young Sexual Minority Men
Supplemental material, sj-docx-1-jia-10.1177_23259582251391273 for Proof of Concept of the Tailored Motivational Interviewing for PrEP Choices Implementation Package for Providers to Support PrEP Uptake and Adherence Among Young Sexual Minority Men by Sylvie Naar, PhD, LP, Crissi Rainer, MSc-GH, Salome Cockern, PhD, Leah King, MPH, Jonathan Morgan, BA, and Lisa Hightow-Weidman, MD, MPH in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251391273 - Supplemental material for Proof of Concept of the Tailored Motivational Interviewing for PrEP Choices Implementation Package for Providers to Support PrEP Uptake and Adherence Among Young Sexual Minority Men
Supplemental material, sj-docx-2-jia-10.1177_23259582251391273 for Proof of Concept of the Tailored Motivational Interviewing for PrEP Choices Implementation Package for Providers to Support PrEP Uptake and Adherence Among Young Sexual Minority Men by Sylvie Naar, PhD, LP, Crissi Rainer, MSc-GH, Salome Cockern, PhD, Leah King, MPH, Jonathan Morgan, BA, and Lisa Hightow-Weidman, MD, MPH in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582251391273 - Supplemental material for Proof of Concept of the Tailored Motivational Interviewing for PrEP Choices Implementation Package for Providers to Support PrEP Uptake and Adherence Among Young Sexual Minority Men
Supplemental material, sj-docx-3-jia-10.1177_23259582251391273 for Proof of Concept of the Tailored Motivational Interviewing for PrEP Choices Implementation Package for Providers to Support PrEP Uptake and Adherence Among Young Sexual Minority Men by Sylvie Naar, PhD, LP, Crissi Rainer, MSc-GH, Salome Cockern, PhD, Leah King, MPH, Jonathan Morgan, BA, and Lisa Hightow-Weidman, MD, MPH in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors thank all the providers who participated in this study.
Ethical Approval
This work follows a protocol reviewed and accepted by the Institutional Review Board of Florida State University (Approval No. 00003623). Participants provided informed consent prior to enrollment in the study.
Author Contributions
Conceptualization: SN and LHW; data collection: CR, JM, and LK; data analysis: CR, SN, and NC; manuscript preparation: SN, CR; NC, LK, and LHW; revision and approval of the final manuscript: all authors. All authors have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
This study is supported by funding from the CDC under award U01PS005246.
Data Availability Statement
The data sets generated and analyzed during this study will be available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.