
Abstract
Background
In Cameroon, people living with HIV (PLHIV) receiving antiretroviral therapy (ART) have a high prevalence of hypertension (HTN) and an increased risk of cardiovascular mortality. Managing HTN in this population is a major challenge. This qualitative study, conducted at the Yaoundé Central Hospital, Cameroon, in 2024, explored the barriers and facilitators to hypertension management in PLHIV.
Methods
The study involved 15 participants, including 9 PLHIV diagnosed with hypertension, 03 healthcare providers, and 03 psychosocial agents. A quota sampling approach was used to recruit participants. Data was collected through 12 in-depth interviews and a focus group with 3 psychosocial agents. Data collection took place over a period of 5 months, from January to May 2024. A semistructured interview guide was used to explore participants’ perceptions of hypertension management. Data analysis was based on the COM-B model to interpret the results, using NVivo software.
Results
Identified barriers included a lack of knowledge about hypertension, difficulties in accessing medications due to high costs, and psychosocial issues such as family stress affecting treatment adherence. Additionally, cultural and religious beliefs, such as a preference for traditional treatments and miraculous healings, limited engagement with conventional medicine. However, facilitators included regular visits for ART follow-up, which allowed for hypertension screening, and financial support from families that facilitated access to treatment. The proactive involvement of healthcare providers and continuous communication also contributed to treatment adherence.
Conclusion
The study highlights the need for interventions that address socio-economic, cultural, and medical barriers to improve hypertension management in PLHIV, particularly through enhancing access to care and raising awareness.
Plain Language Summary
In Cameroon, many people living with HIV also suffer from high blood pressure, which puts them at greater risk of heart disease and early death. Managing both conditions can be difficult. This study, conducted in 2024 at the Yaoundé Central Hospital, aimed to understand what makes it easier or harder for people with HIV to manage high blood pressure. Researchers interviewed 15 people, including 9 individuals living with HIV and hypertension, and 6 healthcare workers. The results showed that many people lack knowledge about high blood pressure and struggle to afford treatment. Family stress and beliefs in traditional or religious healing sometimes prevent people from following medical advice. On the other hand, regular HIV clinic visits allow for blood pressure checks, and family support can help with medication costs. Health workers also play a key role by encouraging and guiding patients. This study shows that managing high blood pressure in people living with HIV requires more than just medicine. It also depends on education, financial support, and trust between patients and healthcare providers. Making treatment easier to access and raising awareness can help people stay healthier and avoid heart-related problems in the future.
Introduction
The widespread use of antiretroviral therapy (ART) has led to viral suppression in 92% of people living with HIV in sub-Saharan Africa, 1 resulting in a 68% reduction in AIDS-related deaths globally and 64% in sub-Saharan Africa. These improvements have narrowed the life expectancy gap between people living with HIV (PLHIV) and those without HIV.2–4 However, the increased life expectancy of PLHIV has led to a rise in noncommunicable diseases, particularly cardiovascular diseases (CVDs),4–6 with hypertension being a major concern.7–9 HIV-positive adults on ART are more likely to have hypertension than those without HIV, 10 with 35% of ART users globally affected, compared to 30% of HIV-negative adults. 4 HTN is 1 of the major cardiovascular risk factors, responsible for severe complications such as stroke, myocardial infarction, heart failure, and chronic kidney failure. These conditions lead to considerable morbidity and premature mortality, especially in low-and middle income countries (LMICs), where access to healthcare and anti-hypertensive treatments remain limited. 11 Recent global and regional reports consistently confirm the high and rising prevalence of hypertension in sub-Saharan Africa (SSA), associated with low rates of detection, treatment, and control. 12
At the same time, advances in HIV care, thanks to antiretroviral therapy (ART), have significantly improved the life expectancy of people living with HIV (PLHIV).13,14 However, this increase in longevity is accompanied by a rise in noncommunicable chronic diseases, including HTN. Several factors explain this trend, including the side effects of certain ARTs, chronic inflammation induced by HIV infection, and metabolic changes associated with the aging of this population.11,14,15 Currently, approximately 25.2% of PLHIV are hypertensive globally, with particularly high prevalence rates in sub-Saharan Africa, ranging from 12.5% to 28.5%, depending on the country.16–20
Despite this concerning situation, the management of HTN in PLHIV remains insufficient in many countries due to various structural and organizational barriers. 21 Although several models of integrating HTN care into HIV clinics are available, 22 in sub-Saharan Africa, most healthcare systems remain focused on infectious diseases, with vertical HIV-specific services that are often poorly integrated with chronic disease care, such as hypertension.22–25 This fragmentation of care, coupled with low rates of HTN screening in HIV clinics, limited access to antihypertensive medications, and a lack of training for healthcare professionals, complicates the management of hypertension in PLHIV.17,26–30
In Cameroon, hypertension prevention is not systematically integrated into HIV care programs. Nevertheless, several hypertension prevention initiatives are available. These include the LeDEA project (International epidemiology Databases to Evaluate AIDS), 31 and the VIHeillir avec le VIH project 32 which address interventions in certain areas of Cameroon. Care for people living with HIV is generally provided in specialized clinics, while patients with noncommunicable diseases (NCDs) receive treatment in general medicine services. Unfortunately, there is little overlap in the management of HIV and NCDs, particularly regarding hypertension. This rigid separation limits the understanding of the true burden of NCDs among people living with HIV. Moreover, the lack of integration between HIV care services and those dedicated to NCDs results in a lack of data on access to hypertension treatment and outcomes among people living with HIV in Cameroon.
As part of our doctoral research program, a cross-sectional study was conducted among 554 people living with HIV (PLHIV) followed at the Yaoundé Central Hospital to assess the burden of hypertension. The results revealed a hypertension prevalence of 36.8%, with 78.4% of patients being aware of their hypertensive status. Nearly half of the cases (49.5%) were classified as Grade I hypertension. The analysis of the care cascade showed a treatment initiation rate of 66.7%, a retention in care rate of 45.6%, and effective blood pressure control in only 22.6% of patients. These findings highlight the still insufficient management of hypertension among PLHIV, despite significant screening efforts.
In this context, our study aimed to identify the barriers and facilitators to the management of hypertension in PLHIV in Cameroon at Yaoundé Central Hospital. A better understanding of these factors can help guide public health strategies toward more effective integration of cardiovascular care into HIV services, thereby improving the quality of life of PLHIV and reducing the burden of cardiovascular diseases in this vulnerable population. Thes paper presented the barriers and facilitators influencing the screening, diagnosis, initiation, adherence, and control of hypertension.
Material and Methods
Study Design
This study employed a descriptive qualitative phenomenological approach, designed to explore the lived experiences and perceptions of people living with HIV (PLHIV) diagnosed with hypertension, as well as healthcare providers involved in their care. Data was collected through semistructured individual interviews and focus group discussions, conducted using a topic guide informed by the COM-B model (capability, opportunity, motivation, and behavior), which provided a theoretical framework to examine behavioral drivers and barriers within the hypertension care cascade. Data collection took place over a period of 5 months, from January to May 2024.
Participants were recruited voluntarily during routine HIV care visits at the study site, using a quota sampling technique to ensure representation across key demographic and clinical profiles. All interviews and discussions were audio-recorded, transcribed verbatim, and coded deductively. Thematic analysis was performed to identify factors that either facilitated or hindered effective hypertension management among PLHIV, based on their direct narratives and reported experiences.
The reporting of this study conforms to the Quality Improvement (SQUIRE) reporting guidelines 33 (Supplemental Material: Equator checklist).
Study Settings
The study took place at Yaoundé Central Hospital (YCH), a secondary-level facility with a dedicated infectious diseases unit. This hospital is an ANRS (National Agency for Research on AIDS and Viral Hepatitis) site-ANRS being a French organization that funds and coordinates scientific research on HIV/AIDS, viral hepatitis, and other infectious diseases. Specifically, our work was conducted at the Day Hospital Service (DHS). Established in 1997 and inaugurated in 1998, the DHS was the first fully operational department at YCH. 34 It is a pioneering service in Cameroon, providing care for people living with HIV. It offers information and diagnostic services (with a particular focus on STIs and HIV), HIV screening, and a variety of consultations (including dermatology, STIs, and general medicine). It also supports medical students working on their theses. We selected this facility because it has the largest and most long-standing cohort of treatment-adherent people living with HIV in Cameroon. Currently, it serves more than 12,000 patients.
Data Collection Tools
Data were collected using semistructured interview guides specifically developed for this study, drawing on the COM-B behavioral framework and WHO recommendations for hypertension management among PLHIV. The guides were designed by the research team and subsequently validated by a committee of professors in medicine and epidemiology at the University of Dschang. A pretest with a small sample of participants was also conducted to ensure clarity, cultural appropriateness, and alignment with the study objectives. Feedback from the validation process and the pretest was incorporated to refine the final version of the guides used for data collection.
Population Definition
The study population consisted of people living with HIV (PLHIV) diagnosed with hypertension (HTN) and their healthcare providers, all recruited from the Day Hospital Service of the Yaoundé Central Hospital. Eligible participants included PLHIV aged 21 years or older, diagnosed with hypertension for at least 3 months and under care at the hospital, as well as healthcare providers with a minimum of 2 years of experience at the facility. Participation was voluntary, and written informed consent was obtained from all participants. Individuals with cognitive impairments that could interfere with their ability to participate in interviews and those who withdrew consent during the study were excluded.
Selection Criteria for Participants
Inclusion Criteria
Participants were eligible if they:
Were people living with HIV (PLHIV) followed at the Yaoundé Central Hospital HIV clinic. Were 18 years or older. Had a diagnosis of hypertension (documented in the medical record or confirmed during routine consultation). Had been enrolled in HIV care for at least 6 months. Were willing and able to provide informed consent to participate in interviews or focus group discussions. Or were healthcare providers working in the HIV clinic, specifically:
- State registered nurses. - Psychosocial workers. - The administrator of the HIV clinic all of whom were directly involved in the delivery or management of hypertension care for PLHIV.
Exclusion Criteria
Participants were excluded if they:
Were critically ill and unable to participate in discussions (eg, acute opportunistic infection, hypertensive emergencies). Had cognitive or communication impairments limiting their ability to respond. Were pregnant women receiving antenatal care (different hypertension care pathway). Declined or were unwilling to provide informed consent.
Sampling Strategy Definition and Recruitment
We employed a quota sampling method, a nonprobabilistic technique used to ensure the inclusion of diverse participants based on predetermined characteristics (age, sex, and profession). 35 This approach was chosen because it allows for the deliberate selection of participants who can provide rich, relevant insights into the research topic while maintaining diversity within the sample.35–39
Participant Recruitment Process
Participants were recruited from the Yaoundé Central Hospital, specifically from the Day Hospital Service (DHS). People Living with HIV (PLHIV) diagnosed with hypertension were identified through hospital medical records by a research assistant in collaboration with treating physicians. Eligible patients were approached during routine medical visits and informed about the study. Healthcare providers were selected based on their roles in the hospital and experience in HIV care. Invitations were extended through official communication channels, including direct invitations from hospital administrators and the research team. Those interested received a detailed explanation of the study objectives and procedures before providing written informed consent.
By targeting individuals within the hospital setting, we sought to capture diverse experiences and perspectives, contributing to a comprehensive understanding of hypertension management. Data collection continued until information saturation was reached. The study included 15 participants: 9 PLHIV diagnosed with hypertension and 6 healthcare providers.
Compensation or Incentives
Participants were not financially reimbursed, but they received refreshments during interviews and focus group discussions as a token of appreciation for their time. Additionally, they were provided with general health information related to hypertension and HIV care, ensuring that their participation had some educational benefit.
Data Collection
Data was collected through 12 in-depth interviews (9 PLHIV, 1 administrator, and 2 physicians) and 1 focus group involving 3 psychosocial agents. Psychosocial agents are professionals or trained personnel who provide psychological, social, and emotional support to individuals or groups facing situations of vulnerability, illness, stress, or crisis. In qualitative research, individual interviews are commonly considered 1 of the most effective methods for gaining a deep understanding of participants’ perspectives. 40 Additionally, focus groups are viewed as an innovative approach that allows for the generation of new ideas and a deeper understanding of the topics being studied by facilitating rich exchanges among participants.41,42
Data were collected using semistructured guides specifically tailored for each type of qualitative method: Individual interviews for patients (IDIs), Key informant interviews health care providers (KIIs), and focus group discussions (FGDs). While the core thematic structure of the guides was consistent anchored in the COM-B model domains of Capability, Opportunity, and Motivation each guide was adapted to the specific objectives and context of the respective interview format. The IDI and KII guides focused on eliciting individual perspectives, personal experiences, and professional insights, whereas the FGD guide was designed to stimulate collective discussion and explore shared experiences and group dynamics. All guides were pretested with a sample of participants not included in the final study to ensure clarity and relevance of the questions. This process allowed for refinement of the tools to maximize the quality and depth of the data collected.
The interview guide was initially tested on 2 PLHIV with hypertension, 1 physician, and 1 psychosocial agent at the same data collection center. The pilot test was conducted by the lead author (TO) and a research assistant. This process allowed us to collect feedback from participants on the tool, identify ambiguous or difficult questions (which were simplified or removed), assess the flow of the interview, and record the time needed to complete the questionnaire. Data from the pilot interviews were thematically analyzed to identify main themes and potential gaps in information. Following this feedback, the guide was revised and improved, resulting in the final version.
After the pilot test, a separate guide was developed for PLHIV with hypertension who had been attending the Day Hospital for over 5 years, as well as for prescribing physicians, the administrator, and psychosocial agents responsible for patient follow-up. This guide aimed to explore the practices for hypertension prevention within the center and how patients managed their blood pressure. TO (Male, epidemiologist) and a research assistant obtained informed consent from participants before conducting one-on-one interviews (in the office assigned to the research team) in French. TO, a PhD student in epidemiology specializing in cardiovascular health and related care for PLHIV, and the research assistant (a master's student in Public Health and Epidemiology), both with extensive experience in conducting semistructured interviews, led this data collection phase.
Throughout data collection, we monitored the information gathered to ensure the consistency of emerging themes. This process enabled us to identify additional aspects that needed to be explored further in subsequent interviews, until we realized that no new information was emerging, signaling data saturation. Data analysis began immediately after the first few interviews, as part of the iterative process. The interviews, which lasted 30 to 45 min, were audio-recorded, and field notes were taken to assist in the interpretation of the audio recordings. No follow-up interviews were conducted, and no compensation was provided for the participants. Data saturation was reached during data collection, indicating that no new themes emerged from additional interviews.
Data Analysis
Data analysis was guided by the COM-B model (capability, opportunity, motivation—behavior), which provided a theoretical framework for organizing and interpreting the qualitative data. This model has been previously applied in similar research contexts, including a 2021 study in Uganda exploring barriers and facilitators to HTN/HIV integration 43 (Table 1). The COM-B model informed the development of the initial coding structure, allowing transcripts to be deductively coded based on its 4 core dimensions.
COM-B Domains Revealing Barriers or Facilitators to Integrating Hypertension Management into HIV Care.

NVivo software (version 14.23.3) was used to support the coding process and enable a constant comparative approach across all transcripts. This iterative process helped to identify recurrent patterns, ensure consistency in coding, and facilitate cross-case analysis. Following initial coding, codes were clustered into broader categories, which were then synthesized into overarching themes. These themes were further analyzed using the 5A framework (availability, accessibility, affordability, acceptability, and accommodation), a model commonly employed to examine healthcare access in chronic conditions such as diabetes, 44 mental health disorders, 45 and HIV . This dual-framework approach allowed for a comprehensive understanding of both behavioral and systemic factors influencing hypertension care among PLHIV.
Bottom of the form
Audio recordings of interviews were transcribed verbatim, anonymized, and verified for accuracy. The data were then imported into NVivo 12 Plus (QSR International), 46 a qualitative data analysis software used to facilitate systematic organization and coding of textual data. A thematic content analysis approach was employed.47,48 Two researchers (TO and IMR) independently read and reread the transcripts to ensure familiarization with the content. Through an open coding process, recurrent issues related to access to hypertension care among PLHIV were identified and labeled as initial codes within NVivo. These codes were then compared and refined collaboratively, with discrepancies discussed and resolved through consensus with the broader research team. 49 A finalized codebook was developed and applied across the full dataset within NVivo.
Techniques to Enhance Trustworthiness
To strengthen the rigor and credibility of our qualitative analysis, we used several strategies. Methodological triangulation was applied by combining in-depth interviews with focus group discussions, allowing us to capture both individual and collective perspectives. An audit trail was maintained, including field notes, reflexive memos, and coding records in NVivo, to ensure transparency. Double coding and peer debriefing were conducted to enhance reliability and reduce interpretive bias. In addition, a limited form of member checking was performed by presenting preliminary findings to a subset of participants and clinicians, which confirmed the resonance of our themes. Finally, the lead interviewer kept reflexive notes to acknowledge and monitor potential researcher influence. Together, these techniques enhanced the credibility, dependability, and confirmability of the findings and support their transferability to similar HIV care settings.
Results Sample Description
In our study, we explored the facilitating factors and barriers to accessing hypertension (HTN) care among people living with HIV (PLHIV) with hypertension at the Day Hospital of Yaoundé Central Hospital. Our qualitative analysis included 15 participants, with a mean age of 58 years and 66.67% being women. Participants were purposefully selected to ensure demographic diversity, including variations in age, gender, and professional roles such as Day Hospital administrators, healthcare providers, patients, and psychosocial support workers. Individual interviews for patients were conducted with PLHIV to gain an in-depth understanding of their lived experiences, attitudes, and behaviors regarding the concurrent management of hypertension and HIV. Additionally, healthcare providers and administrators, as key informants, were interviewed to identify barriers and facilitators to hypertension care more comprehensively. As part of this study, only 3 APS out of the ten approached were available. The focus group was therefore conducted with these 3 participants, who were among the most experienced and had already provided follow-up to several PLHIV with hypertension. Their contributions helped to enrich the identification of barriers and facilitators related to the care and retention of hypertensive PLHIV within the care pathway, particularly regarding hypertension prevention. Table 2 provides a detailed description of the study sample.
Participant Characteristics at Yaounde Central Hospital (YCH).

Barriers to Affective Hypertension Care at Yaoundé Central Hospital
Table 3 presents the key challenges faced by PLHIV in managing hypertension at Yaounde Central Hospital. These challenges are categorized according to the 3 core components of the COM-B model for behavior change: capability, opportunity, and motivation.
COM-B Categorized Barriers to Hypertension Care Among PLHIV at Yaoundé Central Hospital.

Capability-related barriers include limited knowledge of hypertension management and physical constraints, such as advanced age; Opportunity-related barriers encompass inadequate medical equipment, the high cost of antihypertensive medications, and restricted access to cardiologists; Motivational barriers involve patients’ preference for traditional treatments, financial constraints, and concerns about potential medication side effects.
Barriers to Hypertension Screening and Management Among PLHIV
Among the 9 participants included in the study, 7 did not know what blood pressure meant. These 7 individuals were people living with HIV (PLHIV) who had been newly diagnosed with hypertension at the time of data collection. Their understanding of hypertension was limited to the notion that “it is not a good thing.
Furthermore, vision problems among adult PLHIV emerged as a barrier to accessing hypertension screening. In addition, a lack of appropriate equipment for routine blood pressure monitoring in the care services was highlighted. Psychosocial agents (PSAs) also reported this equipment shortage as a major difficulty. Furthermore, some patients exhibit negligence or a lack of interest in screening. Male, PLHIV, 43 years old, hypertensive: I don’t know anything about hypertension. I’ve heard about it, but I never looked for more information. Every time I come to get my ARVs, they put the cuff on my arm; I just thought it was a routine medical procedure. I never asked any questions. Female, PLHIV, 49 years old, hypertensive: I don’t know much. I only know that high blood pressure is not a good thing. Female, 73 years old: I can’t see. I only see shadows. So, I can’t read my blood pressure, I don’t know how to answer you. PSA, 32 years old: The electronic blood pressure monitor doesn’t always work. Sometimes we can go for three months without batteries because it's not funded by the HIV prevention program. We often buy batteries ourselves with our own money. PSA, 41 years old: At the reception, we only have one blood pressure monitor. It was only in 2024 that the supervisor bought it. But with just one device, it's difficult to take the blood pressure of all the patients who come for HIV follow-up. On average, we receive about 200 PLHIV per day. Female PSA 37 years old: some, even when we approach them, even when we call them for vital signs, they run away they just want to go see the doctor. Otherwise, we are always available. But some patients make sure to avoid having their vitals taken.
Barriers to Treatment Initiation for Hypertension Among PLHIV
Among PLHIV, initiating hypertension treatment is often delayed by key barriers. The most cited (8/9 participants) was financial difficulty, including the cost of medications and medical tests. Many were also discouraged by the shift from free HIV services to paid hypertension care. Social influence and preference for traditional remedies (5/9) further reduced adherence to prescribed treatment. Additionally, some patients favored prayer over medical care, believing in miraculous healing. Female, 55 years old, farmer: I know that when they referred me to the cardiologist, I saw that they were going to prescribe some tests. But I didn’t have the money. I didn’t have the money to pay for those exams. 04 Females and 01 Male, PLHIV: Medical doctor: some say they are going to church to pray. They believe that by praying, hypertension will disappear. Female, 68 years old, trader: Yes, since it's not given for free, that's the problem. You see, if it were free like the other one, I would be there. Health administrator:
Retention in Treatment and Effective Blood Pressure Control Are Critical but Particularly Challenging Stages for People Living With HIV
Several obstacles have been identified, including family conflicts, which affect emotional stability and, consequently, medical follow-up even among those on regular treatment. Additional challenges include real or perceived side effects of medications, limited access to treatment due to high costs or unavailability, and the shortage of cardiologists, resulting in long waiting times. Economic and family stress, along with the absence of visible symptoms, further reduce treatment adherence. Finally, some patients lie about their compliance, which complicates clinical monitoring. Woman, 46 years old, married, housewife: …in my household, I always have problems. My husband gives me trouble, so I don’t have peace. You see, I don’t have peace of heart. Woman, 66 years old, retired: Three days later, I started taking it; the cough, the cough, the cough, the cough. I kept coughing. I stopped taking it… Man, 52 years old, teacher: …the cost to see the cardiologist went from 3000 to 5000 CFA. And that's expensive… Sometimes you even get there, and they tell you the cardiologist has too many patients. They will give you another appointment. That's the problem we often face. Woman, 44 years old: It's a bit difficult for me because I don’t do anything in life. I’m responsible for my younger sisters and my mother. My father passed away… Patient (1/9), on adherence: The doctor talked to me a lot. He asked, ‘Why aren’t you taking the medicine?’ I lied to them and said I was.
Facilitating Factors of Effective Hypertension Care at Yaoundé Central Hospital
We also categorized the facilitators according to the 3 components of the COM-B model for behavior change: Capability, Opportunity, and Motivation (Table 4). Capability-related facilitators include the availability of qualified human resources and the extensive technical platform at the Yaoundé Central Hospital. This includes psychosocial workers who provide close follow-up for people living with HIV (PLHIV), case managers, registered nurses, general practitioners, and an integrated cardiology unit.
COM-B Categorized Facilitators of Hypertension Management Among PLHIV at Yaoundé Central Hospital.
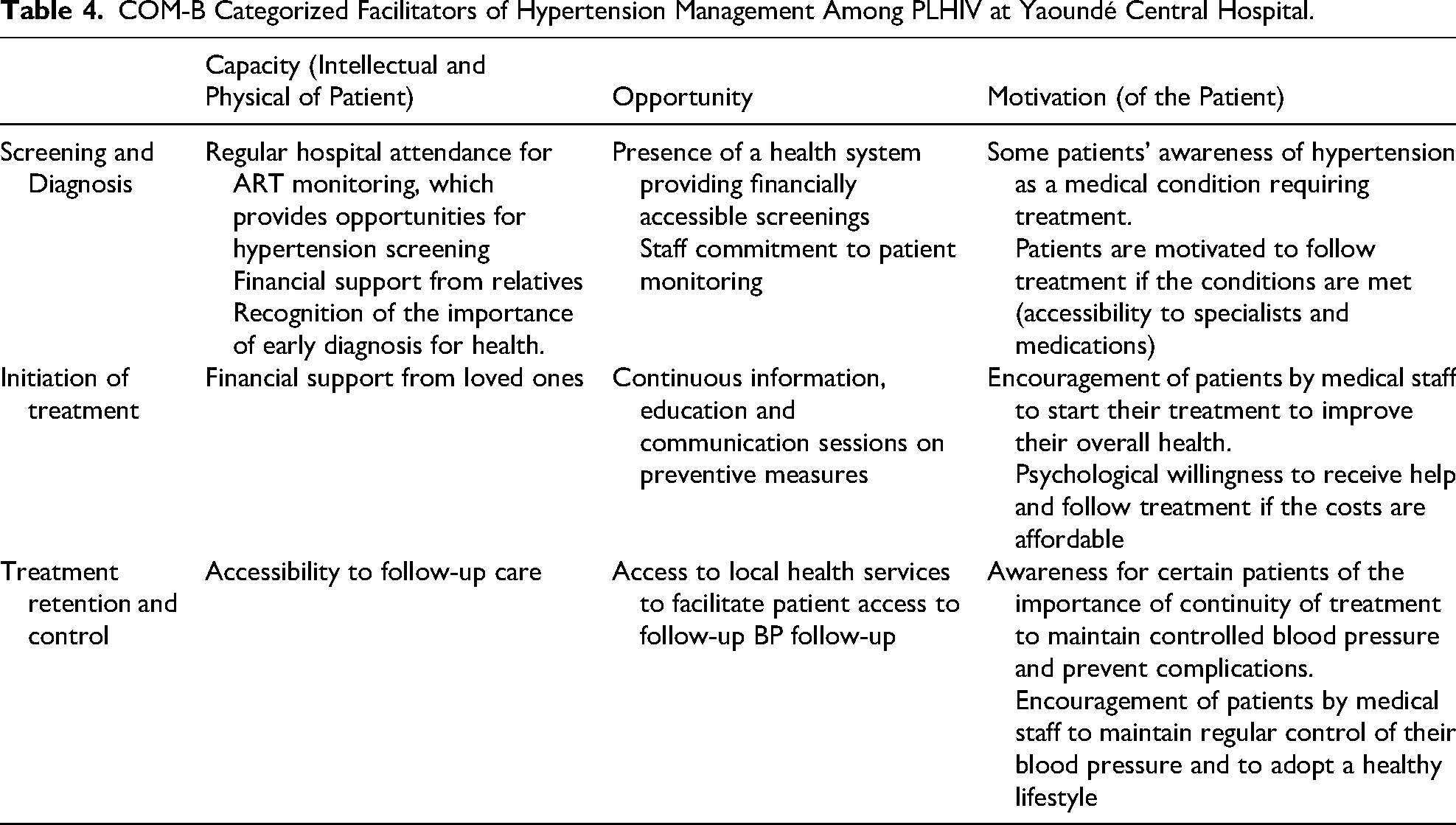
Opportunity-related facilitators involve the implementation of daily awareness sessions on noncommunicable diseases, the provision of free medical consultations, collaboration between the cardiology and HIV prevention units, and the multifaceted support provided by the families of PLHIV. Motivation-related facilitators refer to conscious or unconscious cognitive processes that reinforce positive health behaviors among PLHIV.
The facilitators identified across different levels of the hypertension prevention cascade are as follows.
Screening and Diagnosis
PLHIV regularly attend the day hospital for their routine ART follow-up visits. This regular contact with the health system, combined with an ongoing awareness program and the commitment of the service's leadership to integrate HTN screening into routine care, creates valuable opportunities for each PLHIV to know their blood pressure status. Additional facilitators include the knowledge of hypertension among both healthcare staff and some patients, the availability of a health system that offers screening services, the affordability of consultations, strong staff engagement in patient monitoring, and the support provided by family members to ensure consistent attendance at ART follow-up visits. Female, 54 years old: I came to renew my prescription,” or again, “It was here at the day hospital. I came here. I didn’t come for blood pressure. It was to renew my other issue.” And again: “You see, when they come to do that… that thing there, (blood pressure monitor), that's when they discovered that I was hypertensive. Female, 35 years old: Yes, when I came back last week, I told my children, even my husband, that we must reduce salt and avoid hypertension. Male, 34 years old, psychosocial agent: “So every time they come, if in a week someone comes five times to see the doctor, we check them five times,” reported a psychosocial agent. Female, 41 years old: Yes, I keep track of all that because of my daughter, my little girl. I don’t take my health lightly, I really don’t. Some patients are aware that hypertension is a medical condition requiring treatment, which reflects their willingness to proactively manage their health.
Facilitators of Hypertension Treatment Initiation Among PLHIV
Patients receive financial support from their relatives to initiate hypertension treatment, which enables them to afford necessary medications and consultations. This family support acts as a crucial enabler in accessing care.
Facilitators of Retention in Hypertension Treatment Among PLHIV
Accessibility to follow-up care and proximity of local health facilities facilitate treatment retention for several patients. This ease of access allows for regular monitoring, especially for those who prioritize their health despite daily constraints.
Discussion
This qualitative study explored the barriers and facilitators related to HTA prevention among PLHIV followed up at the day-care unit of the Yaoundé Central Hospital, using the COM-B behavioral framework and thematic analysis. We identified key factors of capability, opportunity, and motivation that hinder or promote screening, treatment initiation, and retention in care. Addressing these multifaceted determinants is essential to improve cardiovascular outcomes among aging PLHIV, who are increasingly exposed to non-communicable diseases (NCDs).50,51
Limited knowledge of HTN emerged as a major barrier among the PLHIV interviewed. More than 50% of them lacked a comprehensive understanding of what blood pressure means and were unaware of the health implications of elevated blood pressure. This reflects weak prevention and awareness efforts around NCDs among PLHIV diagnosed in the “day care” unit of Yaoundé Central Hospital. The burden of HTN among PLHIV is well documented in Africa. However, its prevention remains a major challenge in countries where national guidelines do not incorporate combined HIV and HTN prevention strategies. This is the case in Tanzania, Ethiopia, and Cameroon all low-income countries where several studies have reported that PLHIV lack adequate knowledge about HTN prevention.52–55 Similarly, a study in Kenya showed that PLHIV may die from unmanaged hypertension due to lack of information. 56
Physical limitations identified in this study as barriers represent relatively new findings, though they are logically consistent. For instance, a person with visual impairments may struggle to read their blood pressure values and perform self-monitoring at home. A systematic review analyzing results from 14 studies worldwide indicated that PLHIV with physical disabilities face greater challenges in accessing HTN prevention services, as their attention is often focused on HIV management and physical constraints. Finally, frequent breakdowns of blood pressure equipment, reported by psychosocial support workers in this study, are consistent with previously identified barriers to HIV/HTN integration in Uganda and Tanzania.52,55,57
This study highlights major structural and logistical barriers compromising access to hypertension (HTN) care among people living with HIV (PLHIV) in an integrated care context. Our findings reveal that the prolonged absence of functional blood pressure monitoring devices—often due to a lack of funding for maintenance—contributed to a significant number of missed hypertension screening opportunities during routine antiretroviral therapy (ART) visits. This observation aligns with findings from several African countries, which emphasize the detrimental impact of malfunctioning equipment on the continuity of integrated HIV-HTN care.52,53,57
In addition, the high cost of antihypertensive medications and diagnostic tests constitute a major financial barrier. The shift from free HIV treatment to fee-based HTN management creates a perceived inequity among patients, strongly discouraging both initiation and adherence to anti-hypertensive therapy. This abrupt transition between subsidized and non-subsidized care has also been documented in similar contexts, particularly in Uganda, where it contributes to significantly reduced retention in care for comorbid conditions.58,59
Furthermore, the shortage of specialists, particularly cardiologists, and the long waiting times in referral hospitals exacerbate access inequalities. Participants reported canceled or postponed appointments due to overwhelmed services, a phenomenon that reflects systemic limitations in many sub-Saharan African health systems in managing the dual burden of NCDs. 60 These delays result in interruptions in regular medical follow-up, with potentially serious clinical implications.
Cultural norms and psychosocial vulnerabilities emerged as significant barriers to biomedical engagement in hypertension care among PLHIV. Many participants reported turning to informal or faith-based remedies so-called “street cures” or prayer under the belief that these could cure hypertension. This reliance on alternative healing pathways has also been documented in Tanzania, where patients disengage from biomedical care due to perceptions of high cost, limited access, or mistrust of formal health systems. 59 Such health-seeking behaviors highlight the enduring influence of cultural belief systems in shaping patient choices, particularly in settings where chronic disease care is perceived as inaccessible or unfamiliar.
In addition, fear of medication side effects such as a persistent cough attributed to antihypertensive therapy led several patients to discontinue treatment prematurely. This finding aligns with prior research in sub-Saharan Africa, where adverse drug reactions are a common reason for poor adherence among patients managing dual chronic conditions. 61 Furthermore, psychosocial stressors such as intra-family conflict, social isolation, and economic insecurity further eroded the emotional and cognitive capacity of individuals to sustain adherence to long-term hypertension treatment.
These findings underscore the interplay between automatic and reflective motivational processes, as conceptualized in the COM-B model. 62 Emotional responses (eg, fear, hopelessness) and culturally anchored beliefs (eg, spiritual healing) often override rational intentions to adhere to biomedical care, thereby impeding sustained behavioral change. Interventions seeking to improve hypertension control among PLHIV should therefore go beyond clinical algorithms to address psychosocial readiness, build trust, and engage with patients’ cultural and emotional contexts through tailored counseling and peer-led support.
Beyond the barriers, this study identified several enablers that supported the effective management of HTN within HIV care settings. First, the presence of multidisciplinary teams including psychosocial workers, case managers, nurses, and general practitioners created structured and continuous learning opportunities for PLHIV to understand and monitor blood pressure. Similar facilitators have been documented in Tanzania, where targeted training of healthcare workers on NCDs improved early detection and referral when diagnostic equipment was available. 63 The gradual integration of routine blood pressure screening into the HIV care continuum also fostered psychological capability, as patients became increasingly familiar with the process, reducing anxiety and promoting confidence in engaging with HTN services.
Second, environmental and social opportunities were reinforced by strategic service design. Daily health education sessions on NCDs, the availability of free consultations, and the physical proximity between HIV and cardiology services enabled access to HTN care without requiring additional clinic visits. This “one-stop” integration mirrors findings from Uganda, where streamlined service delivery reduced transportation costs and logistical burdens, thereby improving retention.50,64,65 Moreover, family financial support It's my son, he helps me a lot emerged as a form of social opportunity, enabling medication adherence and access to diagnostic tests in the absence of public subsidies.
Motivational factors were also enhanced through targeted information, education, and communication (IEC) interventions conducted while patients waited for their antiretroviral consultations. These sessions strengthened reflective motivation by deepening understanding of the risks associated with uncontrolled hypertension and the benefits of early intervention. Similar results were reported in Tanzania, where counselling on lifestyle changes and adherence support contributed significantly to effective HTN management. 66 As awareness grew and patients realized that manageable adjustments in diet and behavior could prevent serious complications, intrinsic motivation was reinforced an outcome consistent with the COM-B framework, which emphasizes the importance of both automatic and reflective processes in sustaining health-related behaviors. 62
Drawing on these findings, we propose 3 programmatic priorities to optimize HTN-HIV service integration: (1) fully integrate HTN screening, prescription, and follow-up within HIV clinics; (2) subsidize antihypertensive medications and diagnostic procedures to prevent care discontinuity when shifting from free to fee-based services; and (3) invest in workforce training, reliable equipment maintenance, and peer-led education programs to build both capacity and motivation. These strategies correspond to COM-B informed intervention functions education, enablement, environmental restructuring, and modeling that have proven effective in other NCD integration initiatives. 62
Conclusion
In conclusion, this content analysis highlights the prevalence of hypertension among people living with HIV (PLHIV) and reveals the significant challenges they face at various stages of the hypertension care cascade. Our results emphasize that many PLHIV face significant barriers to effective hypertension management, including a lack of knowledge about hypertension, limited access to affordable medications, insufficient healthcare infrastructure, and reduced availability of specialized care. Moreover, socio-economic factors such as financial strain and the preference for traditional treatments further complicate the management of hypertension in this population.
However, several facilitating factors have been identified that could improve hypertension care for PLHIV. These include the integration of hypertension screening into routine HIV care, the motivation of patients who regularly attend ART follow-up consultations, and the importance of accessible healthcare services. The study also highlighted the need for better coordination between HIV and hypertension care, as well as more comprehensive hypertension treatment protocols tailored to the specific needs of PLHIV.
Considering these findings, it is evident that hypertension care in the context of HIV requires a multifaceted approach. Strengthening health systems, including providing necessary resources, training healthcare providers, and developing clear, context-specific treatment protocols, is crucial. Furthermore, policies that promote access to affordable antihypertensive treatments and encourage community engagement in health promotion efforts are essential to improving outcomes. Collaboration between healthcare providers, patients, and community stakeholders will be key to ensuring that hypertension care is effectively integrated into HIV care and that PLHIV receive optimal care for both conditions.
In summary, the management of hypertension in PLHIV requires comprehensive strategies that combine improvements in the healthcare system, patient education, and targeted interventions, with a focus on addressing the social and structural factors that hinder access to and adherence to hypertension care.
Limitations
This study offers valuable contextual insights into the behavioral determinants of hypertension management among PLHIV in Cameroon. However, several limitations must be acknowledged to frame the interpretation and applicability of the findings. First, the research was conducted in a single urban HIV clinic, which may limit the transferability of the results to other settings, particularly rural or under-resourced areas. Second, while the sample was purposefully diversified to capture a range of experiences—including 12 in-depth interviews (9 PLHIV, 2 physicians, and 1 administrator) and a focus group discussion with 3 psychosocial workers, the small sample size inherent to qualitative research restricts generalizability. Moreover, reliance on self-reported data introduces potential biases, including social desirability and recall inaccuracies.
To mitigate these issues, we employed several strategies: interviews were conducted by trained independent interviewers in a confidential setting to minimize interviewer bias and encourage openness; data collection continued until thematic saturation was achieved, ensuring robustness of the findings; and triangulation across participant categories (patients, clinicians, psychosocial staff, and administrators) enhanced the credibility of the interpretations. Finally, although qualitative designs do not aim for statistical representativeness, they allow for a deep exploration of lived experiences at a specific time point. While this temporal snapshot is a limitation in terms of anticipating future developments, it remains appropriate for the exploration and inductive nature of the study. Future research should build on these findings through longitudinal or mixed methods approaches across diverse settings to confirm and expand the transferability of the insights.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251383981 - Supplemental material for Barriers and Facilitators of Hypertension Care Among PLHIV at Yaoundé Central Hospital, Cameroon. Qualitative Research 2024
Supplemental material, sj-docx-1-jia-10.1177_23259582251383981 for Barriers and Facilitators of Hypertension Care Among PLHIV at Yaoundé Central Hospital, Cameroon. Qualitative Research 2024 by Francis Duhamel Nang Nang, Liliane Kuate Mfeukeu, Rita Marie Ifoue, André Pascal Kengne, Paul Junior Cheubo, Jean Pierre Junior Tchitetchoun, François Anicet Onana, Fabrice Djouma Nembot, Anastase Dzudie, Siméon Pierre Choukem and Charles Kouanfack in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251383981 - Supplemental material for Barriers and Facilitators of Hypertension Care Among PLHIV at Yaoundé Central Hospital, Cameroon. Qualitative Research 2024
Supplemental material, sj-docx-2-jia-10.1177_23259582251383981 for Barriers and Facilitators of Hypertension Care Among PLHIV at Yaoundé Central Hospital, Cameroon. Qualitative Research 2024 by Francis Duhamel Nang Nang, Liliane Kuate Mfeukeu, Rita Marie Ifoue, André Pascal Kengne, Paul Junior Cheubo, Jean Pierre Junior Tchitetchoun, François Anicet Onana, Fabrice Djouma Nembot, Anastase Dzudie, Siméon Pierre Choukem and Charles Kouanfack in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
Special thanks to the study participants for their willingness to contribute to the increase of scientific knowledge. We also extend our profound appreciation to the dedicated research assistants whose unwavering commitment played a pivotal role in bringing this significant work to fruition.
Ethics Approval and Informed Consent Statements
Administrative authorization was granted by the Director of the Central Hospital of Yaoundé (N02023/265/AR/MINSANTE/SG/DHCY/UAF) on May 8, 2023, prior to the commencement of data collection. This study was approved by the Ethics Committee of the Regional Ethics Committee for Human Health Research in the Central Region (N000633/CRERSHC/2023) on August 8, 2023. All participants provided written informed consent prior to enrollment in the study.
Ethical Considerations
In order ensure the protection of those involved in the research and to ensure the dissemination of results, in all equity, ethics is a priority in our study. In addition to the ethical clearance obtained from the Regional Ethics Committee for Human Health Research in the Centre Region (CRERSH-CE)” and the administrative authorization of the Directors of the various health facilities, this study was carried out in strict compliance with the fundamental principles of medical research, in particular:
Potential Risks/Ethical Issues
The potential risks that may arise from the implementation of this study concern the psychological aspect. In addition to the burden experienced by the HIV patient, the announcement of the diagnosis of Hypertension could also influence the patient's psychological wellbeing.
Risks and minimization measures.
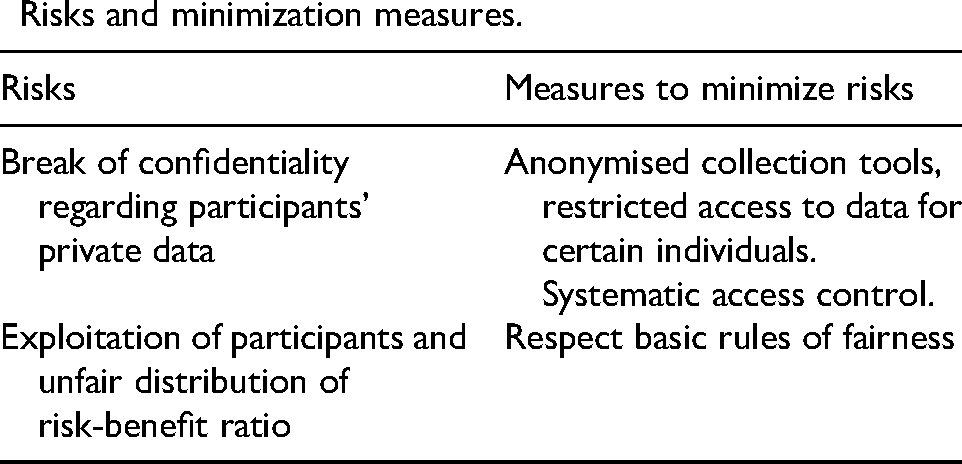
| Risks | Measures to minimize risks |
|---|---|
| Break of confidentiality regarding participants' private data | Anonymised collection tools, restricted access to data for certain individuals. Systematic access control. |
| Exploitation of participants and unfair distribution of risk-benefit ratio | Respect basic rules of fairness |
Ethical Regulations Applicable to This Study
National
- Circular letter N0 D36-13/LC/MINSANTE/SG/DROS/YC relating to the implementation of operational health research in Cameroon.
- ORDER No: 00977/A/MINSANTE/SESP/SG/DROS of April 18, 2012, on the creation, organization, and functioning of Research Ethics Committees for Human Health within structures under the authority of the Ministry in charge of Public Health.
International
- The Nuremberg Code.
- Declaration of Helsinki, 2013
Authors’ Contributions
Conceptualization, methodology: NANG NANG Francis Duhamel, Liliane KUATE MFEUKEU,Rita Marie IFOUE.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
All materials not included in this article are freely available from the authors on reasonable request.
Social Value/Benefit
The social value/benefit of such a study is multifaceted. Firstly, participants in the study will have access to information on the prevention of hypertension and cardiovascular disease, as well as methods and strategies for the management of hypertension. Secondly, the study can lead to improved healthcare outcomes for PLHIV by identifying barriers and facilitators to hypertension care steps. This could enhance screening rates, timely diagnosis, treatment initiation, retention in care, and better blood pressure control among PLHIV. Additionally, by addressing hypertension care in this population, the study may contribute to the overall health and well-being of PLHIV, reducing the risk of cardiovascular diseases and improving their quality of life. Moreover, the findings could inform healthcare policies and interventions tailored to the specific needs of PLHIV with hypertension in Cameroon, promoting more effective and targeted healthcare services.
Scientific Validity of the Study
The methodology and data analysis procedures in this study are scientifically valid and sufficient to achieve expected results. The sample, data collection, analysis procedures, and personnel meet scientific criteria. Local socio-cultural and political conditions support the study, with ethical approval obtained from the regional ethics committee.
Supplemental Material
Supplemental material for this article is available online and francduhamenanl@yahoo.com
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.