
Abstract
Background
Youth with HIV disproportionately experience psychological trauma, but implementation methods for trauma-informed care are lacking.
Methods
To identify potential processes and determinants of trauma-informed care implementation, we conducted process mapping and qualitative interviews and thematically applied the organizational trauma resilience framework to elicit perceived safety, stability, and nurturance in a pediatric HIV clinic.
Results
Forty-three personnel and 8 patient representatives engaged in process mapping; 20 completed qualitative interviews. Clinic culture was described as supportive, cohesive, and equity-focused, but requiring workflow improvements for patient autonomy. Trauma screening, assessment, and interventions were limited/inconsistently applied, with duplicative risk assessments. Support for professional quality of life was limited, despite burnout/attrition reports. Some personnel had trauma-focused training, but ongoing education and culturally responsive policies were needed.
Conclusions
Process mapping presented as a low-burden tool for unveiling gaps and care standards; alongside qualitative interviews, these methods provided practical insights for trauma-informed HIV care.
Plain Language Summary Pre-implementation stage research to guide Trauma-Informed Care for Youth with HIV in the Southern US: A Multi-Method Study
Youth with HIV disproportionately experience psychological trauma, but implementation methods for trauma-informed care (TIC) are lacking. To identify factors that might influence the implementation of TIC, we conducted process mapping (PM) and qualitative interviews in a pediatric HIV clinic and thematically applied the organizational trauma resilience (OTR) framework. Forty-three personnel and 8 patient representatives completed PM, and 20 personnel completed interviews. Clinic culture was described as supportive, cohesive, and equity-focused, but workflow improvements were suggested to elevate patient choice. Trauma screening, assessment, and interventions were limited/inconsistently applied, and risk assessments were duplicative. Support for professional quality of life was limited, despite burnout and attrition. Some personnel had trauma-focused training, but ongoing TIC education was requested as were culturally responsive policies. PM presented as a low-burden tool for unveiling gaps and established care standards. Findings were enriched by qualitative interviews, together providing practical insights for TIC pre-implementation in HIV care.
Keywords
Introduction
Populations experiencing high levels of psychological trauma require trauma-sensitive healthcare services to promote optimal wellness. According to the American Psychiatric Association, trauma refers to lasting social, physical, sexual, mental, or spiritual effects of adverse events, such as catastrophes (eg, natural disasters), personal violations (eg, child abuse and racism), or life-threatening situations (eg, motor vehicle accidents and sexual assault). 1 Social determinants of trauma are structural and social drivers of trauma contributing to worse health outcomes. Some examples of social determinants of trauma include extreme poverty in which someone experiences prolonged housing or food insecurity or repeated exposures to microaggressions and/or discrimination related to race, gender, or sexual orientation, health status, etc. 2 In the case of HIV, the relationship between HIV and trauma is bidirectional so that trauma exposure is connected to increased likelihood for acquiring HIV and worse health outcomes among people with HIV. People with HIV experience disproportionately higher rates of trauma, suffer more severe consequences, and face additional trauma related to their diagnosis and stigmatized serostatus.3,4 These cumulative stressors contribute to rates of post-traumatic stress disorder up to 20 times higher than in the general populations, 5 as well as increased disengagement from HIV care and a higher likelihood of unsuppressed viremia.3,4 Youth with HIV (YWH) experience unique barriers in preventing and addressing trauma and are particularly vulnerable to deleterious neurophysiological changes, given these trauma exposures occur during critical years of brain development. 6
Trauma-informed care (TIC) is a multilevel, evidence-based approach for improving health outcomes across all age groups,7,8 with growing evidence supporting its effectiveness among youth. 8 Generally, TIC interventions are implemented to foster safer care spaces by equipping personnel to realize, recognize, and appropriately respond to trauma, thereby resisting the risk of retraumatization among both patients and personnel. 9 Although TIC has been an underutilized approach in HIV care spaces, some evidence suggests TIC has the potential to attenuate the syndemic relationship between HIV and trauma. 5 , 10 Its implementation has been associated with positive outcomes across multiple groups. For patients, it has led to improvements such as increased resilience and decreased post-traumatic stress symptoms. 7 For providers, benefits include greater compassion satisfaction through reduced burnout, higher training satisfaction, and enhanced knowledge, attitudes, confidence, and readiness to implement TIC.3,7,9,10 At the institutional level, TIC has been linked to increased organizational readiness and the achievement of TIC champions. 7 Despite strong advocacy from HIV care personnel, there is a paucity of documented efforts to integrate TIC in HIV care settings.1,3,11,12 Extant trauma interventions insufficiently focus on people with HIV and have primarily emphasized patient-level outcomes rather than multilevel system change. Moreover, few studies have been conducted in the United States or in pediatric HIV care settings. 13
Furthermore, a dearth of literature explores methods and frameworks for guiding the systematic implementation of TIC. Various forms of data collection have been applied to explore perceived barriers and facilitators of TIC adoption in HIV care settings as well as standards of care relevant to a TIC paradigm.11–14 However, there are limitations to these methods. For example, qualitative methods via one-on-one interviews can be time-consuming for personnel and require resources for monetary incentives as well as transcribing and conducting analyses. 11 Quantitative methods such as surveys12–14 often do not provide opportunities for responses to be clarified or further explored. Interviews and surveys depend on self-reported data and often lack opportunities for personnel to collaboratively develop a cohesive understanding of the current system. As a result, these methods may fail to capture critical practices or conditions relevant to successful implementation. Conversely, approaches that combine subjective and objective assessments through iterative collaboration between implementation researchers and end-users—such as frontline personnel—offer a more holistic means of building a shared understanding of organizational workflows. 15
Therefore, this study explored alternative pre-implementation methods that could foster a shared understanding of factors influencing TIC adoption, while also enhancing implementation efficiency. Two recent HIV studies highlight process mapping (PM) as an underutilized method for visually capturing organizational activities and practices, thereby clarifying context within complex health systems and identifying opportunities for workflow improvement.15,16 Originally developed in engineering and later adopted for quality and process improvement, PM has emerged as a valuable tool for generating shared visual representations of health systems as they currently function, illuminating existing resources, service gaps, and needs prior to implementing interventions.17,18
PM was selected because of its noted efficiency (ie, may be conducted quickly with few resources needed) and promotion of an experiential approach for engaging end users to create a collective understanding of a system and what might be needed for intervention adoption. 15 An additional benefit of PM is its ability to be led by research beneficiaries such as end-users or personnel responsible for implementing the intervention. This participatory approach enables end-users to actively co-define their understanding of the intervention, while also deepening their insight into the project's goals and objectives and fostering forward thinking about future adaptations.
The organizational trauma resilience (OTR) framework is an empirically developed, valid model designed from community-engaged research for operationalizing resilience-focused TIC principles and constructs in care systems. This framework lays out dimensions for measuring the extent to which an organization is perceived to be safe, stable, and nurturing and does so through the dimensions of (1) Culture of Trust and Support; (2) Practices of Inclusivity, Safety, and Wellness; (3) Collaboration and Empowerment; (4) Trauma Responsive Services; (5) Training and Sustaining Trauma Responsiveness/Impact of Provider's Training; and (6) Cultural Responsiveness.19–23 OTR has been applied in a variety of settings to assess fidelity to a TIC paradigm.19–23
Because no literature could be found applying PM to TIC, we sought to integrate best PM practices with a validated TIC framework to apply a novel methodological approach. We complemented PM discussions with personnel qualitative interviews to triangulate findings and compare results between methods.
Methods
Setting and Period
This study was conducted in a pediatric HIV clinic in a Southeastern US region between December 2021 and August 2022. This clinic is situated in a region that is disproportionately impacted by the HIV epidemic and located in an urban academic medical center. This clinic serves approximately 250 children up to the age of 24, with many experiencing high rates of psychological trauma. 23 Holistic services provided include transportation, meals, research activities, psychosocial support, and services to prevent and treat sexually transmitted infections and other medical care from various healthcare professionals. Such capacity and capability are supported primarily by charitable donations, Ryan White HIV/AIDS Program at US Health Resources and Services Administration (HRSA), fee-for-service payment, and research funding from collaborative groups, foundations, and pharmaceutical companies.
Integrating a TIC Framework With Process Mapping and Qualitative Interviews
Given this clinic is in a region with high HIV incidence and strong evidence for disproportionate trauma experiences among people with HIV, there was a stated need for implementation of TIC in this clinic. However, this clinic had not previously engaged in any research related to TIC, which necessitated pre-implementation data collection to guide this implementation. Thus, we sought methods that supported collection of standards of care and processes that might influence implementation. Toward this end, we chose a multimethod approach, including process mapping and qualitative interviews.
PM may be carried out through a 5-phase approach, including preparation, planning, and process identification; data and information gathering; process map generation; analysis; and taking it forward. 17 In this study, we applied the 5-phase PM approach by adhering to all corresponding quality metrics (see Table 1). This included engaging and educating community members or intervention end-users, utilizing standardized mapping symbols, validating the final process maps, and planning how to leverage the insights gained to inform subsequent implementation efforts.
Phases, Quality Criteria, and Activities to Develop Process Map Showing Alignment With Trauma-Informed Care.

Note: Phases and quality metrics from Antonacci et al 17 ; trauma-informed care material informed by Substance Abuse and Mental Health Service Administration Treatment Improvement Protocol (TIP) 57, Organizational Trauma Resilience Assessment (OTRA), and Organizational Trauma Resilience—Patient Reported Experience Measure (OTR-PREM).
Abbreviations: PI: principal investigator; PM: process mapping.
The validated OTR framework 19 was selected as our TIC framework to thematically guide the multimethod approach including PM discussions, qualitative interviews, and analytical methods. The following sections elaborate how we apply the OTR framework to PM discussions with a case clinic.
Nature of the Study
The current study used a multimethod approach that was conducted in 2 stages. Stage I was for process mapping, and stage II was for one-on-one qualitative interviews and data triangulation to unveil areas not covered through stage I.
Stage I: Process Mapping
Table 1 outlines the 5 PM phases, associated quality metrics, and proposed activities to guide the pre-implementation. PM metrics included identifying service areas, educating staff, engaging patient representatives, incorporating diverse perspectives, using standardized symbols, validating maps, and applying findings to improve workflows. The process involved iterative engagement with clinic personnel and patient representatives to explore who, what, and how of clinic operations. A multidisciplinary team leading the project included an epidemiologist, physician scientist, psychologist, and social workers (Supplemental Table 1). All patient-facing staff were invited via email, with follow ups and flexible meeting times to increase participation. To encourage participation, PM meetings were scheduled at times convenient for each participating group. PM discussions were guided by a structured outline, as detailed in Supplemental Table 2.
Phase 1: Preparation, Planning, and Process Identification
Phase 1 began with regular meetings among multiple principal investigators (mPIs), which led to receiving project support from the clinic director. The PI shared broadly with personnel about the significance, principles, and implementation domains of TIC. Plans to engage the community were also presented as part of an established community advisory group, Connect 2 Protect, which comprises researchers, practitioners, people with HIV, and/or those receiving HIV prevention services. Staff discussion group guides were reviewed in the advisory group to gather feedback and inform development. The mPIs communicated with clinic personnel about the intent of the project. The PI met monthly with an NIH-assigned Implementation Science Hub with the University of Alabama at Birmingham Center for AIDS Research24,25 to discuss engagement strategies and plans for the PM meetings.
Supplemental Table 2 shows the semistructured PM discussions developed around OTR dimensions, 19 including: (1) culture of trust and support, probing for clinic culture relative to peer interactions and provider–patient relationships; (2) collaboration and empowerment, examining practices that promote patient-centered care through collective decision making, as well as personnel's sense of empowerment in their roles; (3) trauma responsive services, exploring trauma exposure screenings, post-traumatic stress disorder assessments, and related clinical interventions; (4) practices of inclusivity, safety, and wellness, evaluating efforts to incorporate patient experiences and care preferences into practice, while also promoting a balanced and fulfilling work environment for staff, such as fostering professional wellbeing through greater compassion satisfaction relative to burnout; (5) training and sustaining trauma responsiveness, probing for workforce development efforts; and (6) cultural responsiveness, assessing efforts to promote diversity, equity, and inclusion at the clinic-level for patients and personnel.
Phase 2: Data and Information Gathering
Discussions were held through in-person site visits and virtual meetings, with detailed notes documenting observations, staff interactions, and clinic materials. Responses were organized by the OTR dimensions using a priori developed themes based on SAMHSA's TIP 57 (Supplemental Table 2). Analysts trained in qualitative research and trauma-informed HIV care organized findings in real time and after each meeting to update the visual map. Once the discussions concluded, the final map was validated by clinic staff. Meals and snacks were provided during in-person meetings to encourage participation.
Patient representatives were engaged through a community advisory group with established ties to local HIV providers. Recruited via verbal and electronic invitations, members participated in an experiential activity to provide feedback on clinic workflows. After a presentation on TIC principles, the group reviewed a list of appointment-related services and asked to prioritize their preferred care sequence. They then compared this ideal workflow to the clinic's actual process, offering suggestions to make services more patient-centered and choice-driven.
Introductory meetings clarified roles and responsibilities across phases of care (see Supplemental Table 1 for guiding topics and prompts). Follow-up sessions were used to engage providers in service-specific small groups—such as registration, nursing, physicians, psychosocial services, research, and pharmacy—to explore team workflows and shared standards of care related to the OTR domains.
Introductory personnel meetings focused on fleshing out who is responsible for each phase of care and what type of care is provided. See Supplemental Table 1 for a list of topics, questions, and prompts applied during meetings. Follow-up group meetings focused on gaining a deeper understanding of how care is provided. For this portion, providers were engaged in small groups by service so that personnel at each service area could explore their team workflows and shared standards of care related to the OTR dimensions.
Phase 3: Process Map Generation
Study PIs reviewed all notes from staff and patient discussion groups and created an initial process map. Standardized PM symbols and structures found in the literature were utilized to construct the map esthetically.26–28 The map was visually designed to show patient care flow for each visit, beginning from intake following an external HIV diagnosis, and the remainder to demonstrate the flow by which patients receive routine care beginning on their first visit, with some patients receiving behavioral health services and/or research activities throughout their care experience. Specific symbols (eg, gray shadow) were used to depict first visits versus all follow-up visits, with all visits following a similar flow of care provision.
Study PIs reviewed discussion notes to develop an initial process map using standardized symbols from the literature. The map illustrated patient care flow, starting from intake after an external HIV diagnosis through routine visits, including behavioral health and research activities when applicable. Visual cues (eg, gray shadows) distinguished first visits from follow ups, which followed a consistent care pathway.
Phase 4: Analysis
To analyze findings from PM activities relative to OTR dimensions, data was organized in real time according to the a priori OTR theme document and iteratively applied to the map during and immediately following each discussion group, to ensure changes were made based on the integration of group member feedback. Data were organized by reviewing thick notes from discussion group meetings and organizing discussion points by the OTR dimensions in the theme document (see Supplemental Table 2). Once data were used to inform a draft map, this draft was utilized visually to conduct validation checks for accuracy with a member of each service area as well as the patient representative group.
Phase 5: Taking It Forward
Results from PM discussions were applied to develop an overarching plan for moving TIC pre-implementation forward in the case clinic setting. Findings helped to generate a list of action items: an implementation action plan with timelines, identify individuals who might be responsible for actions, and tailor a one-on-one interview guide to be utilized in future interviews to explore TIC dimensions that presented as too sensitive to be assessed in group discussion format, including: culture of trust and support; collaboration and empowerment, and further probe into cultural responsiveness. Final PM findings were shared clinic-wide with personnel to generate recommendations for long-term actions (eg, general policies and procedures to be refined in the clinic) and short-term actions (eg, best methods for equitably creating a steering committee).
Stage II: Qualitative Interviews, Statistical Analysis, and Data Triangulation
Once PM data had been analyzed and reviewed, authors discussed results and OTR framework areas that were not well represented or elicited as part of PM activities to plan qualitative one-on-one interviews with clinic personnel. All clinic and ancillary personnel were invited to participate, and the study relied on a convenience sample. There was no exclusion criteria. The interview guide was based on domains and constructs from the Consolidated Framework for Implementation Research 2.0 to assess for perceived barriers and facilitators to TIC implementation.
Generally, qualitative interviews were audio recorded, transcribed verbatim, and analyzed by a team of 3 researchers through 4 cycles of coding conducted separately from the PM results. We aimed for an a priori sample size of at least 20 participants before we began coding to determine data saturation. An in-depth description of interview methods and the analytical approach can be found elsewhere. 29 In short, data were analyzed thematically using the Consolidated Framework for Implementation Research (CFIR) CFIR 2.0, via 4 cycles of coding by researchers who were external to the clinic environment. All 3 coders were cisgender female, with a mixed racial composition. For the first cycle of coding, coders independently labeled each transcript by CFIR domains into an Excel spreadsheet with example quotes broken into barriers and facilitators. Based on these results, coders agreed data saturation had been reached and agreed no more interviews were needed. Second-cycle coding entailed that initial barriers and facilitators were organized by CFIR domain and construct to design a codebook. Third cycle coding focused on consensus building around appropriate quotes by construct and terms to differentiate definitions for constructs in the codebook. The fourth cycle occurred as final codes were described as exclusive from one another in narrative form in a Word document. An additional fifth cycle of analysis occurred with authors reviewing findings from both PM and interviews to triangulate results between the methods by looking for similarities and differences in findings according to the subdimensions of the OTR. To compare findings, which are presented in Table 2, output summaries from each approach were reviewed and discussed to generate a list of findings by OTR construct.
Results by Research Method Organized by Dimensions From the Organizational Trauma Resilience Framework, With Sample Quotes From Interviews.

Note: The OTR framework expresses 6 dimensions: (1) culture of trust and support; (2) collaboration and empowerment; (3) trauma responsive services; (4) practices of inclusivity, safety, and wellness; (5) training and sustaining trauma responsiveness; and (6) cultural responsiveness. We present findings related to each in the following subsections.
Abbreviations: ART, antiretroviral therapy; TIC, trauma-informed care.
Ethical Considerations
Though PM data may be collected generally as part of program evaluation, activities conducted for the current case clinic were approved and connected as part of a larger research study as ceded by the primary institution for which data were collected to Meharry Medical College (21-07-1105) and University of Memphis (PRO-FY2022-201). The Revised Standards for Quality Improvement Reporting Excellence (SQUIRE) 2.0 checklist was followed as a framework for reporting PM findings as part of healthcare quality improvement (see Supplemental Table 3).
Results
Sample
The study participants consisted of research personnel, clinical personnel, and patient representatives (Supplemental Table 1). The clinic personnel included administrative roles (eg, Director of HIV Program), patient-facing roles (eg, physicians, advanced practice providers [APPs], nurses, psychiatrist, psychologist, and pharmacists), and other psychosocial staff (eg, Chaplain, music therapist, and social workers). The patient representatives were mainly same-gender-loving young individuals of color at risk or living with HIV. There were 43 personnel (Supplemental Table 1) and 8 patient representatives from the clinic who participated in the PM. The final process map is depicted in Figure 1 and shows who were involved in the clinic process, what type of care was provided, and how it was provided. The overall time spent in PM activities was around 12 h. Subsequently, qualitative interviews were conducted with 20 clinic personnel. Participants were primarily female (90%) and had a median age of 48 (interquartile range [IQR]: 42-54). Their racial/ethnic backgrounds included 40% Black, 40% White, one Asian, and one Native American/Hawaiian.

Process Map of Trauma-Informed Care in a Pediatric HIV Clinic. Note: Example of a process map of a patient experience interfacing with a pediatric HIV clinic system. Gray diamonds indicate decision points in which one service is utilized to determine the best next steps for patients that are tailored to their specific needs. Green triangles indicate current practice that is aligned with an organizational trauma-resilience framework of trauma-informed care. Green font indicates a practice identified that could benefit from increases in OTR practices or conditions. Blue font indicates a practice promoting trauma responsive services.
OTR Framework Results
Findings from the PM discussions and qualitative interviews are presented by OTR dimensions. Table 2 presents a summary of these results by research method with a sample quote from interviews.
Culture of Trust and Support
Both PM discussions and interviews with clinic personnel indicated a positive view of the clinic culture, described as patient-centered, equity-focused, and collaborative. Staff felt prepared to appropriately respond to patient trauma due to strong team interactions and mental health team involvement. Many described the clinic environment as familial, emphasizing mutual support. One person explained, “I think honestly we have a culture for acceptance with that. We have an awareness of the experience of our patients and the importance that trauma plays in their lives” (Transcript 5).
However, interviews unveiled that some of the staff felt disconnected from the larger hospital setting and desired more leadership support. One staff member stated, “I think [clinic administrator] has stated support […] of this, but I'm not sure that… I think there's too many other things competing for [them] to show the instrumental support that's needed. And by that, I mean like blocking time and bringing it up as a priority and advocating for it. Haven't seen that necessarily […] [they are] not against it, let's put it that way, but I don't know that [they have] the capacity right now to support it in the way that is needed” (Transcript 3).
Collaboration and Empowerment
Findings from PM discussions and interviews with both personnel and patients differed regarding collaboration and empowerment, with interviews providing deeper explanations. One discrepancy emerged about access to patient information. PM discussions indicated difficulty accessing patient assessments, whereas interviewees reported visibility of the electronic medical record across teams and for families. Moreover, PM discussions indicated that patients had significant control over their care decisions, such as choosing psychosocial services, administration of sexually transmitted infection swabs, vaccines, and selection of antiretroviral therapy at initiation. Conversely, interviewees expressed that patients could be more intentionally engaged to provide feedback, with one person stating, “We have a community advisory, but it's really just for research. And so, we don't really involve patients, or we have not asked, I should say. They can certainly provide feedback, but they're not brought to the table …” (Transcript 5). Overall, the clinic was reviewed positively for cohesive communication, peer support, and collaborative crisis response.
Trauma Responsive Services
Both PM and interviews consistently elicited information on the levels and types of trauma responsive services relative to screenings, assessments, approaches, interventions, and general workflow. All patients were reportedly connected with a clinical social worker who provided case management and psychosocial support, including bi-annual psychosocial assessments and annual Adverse Childhood Experience (ACE) screeners. 30 Those expressing or demonstrating need for mental healthcare in medical appointments or bi-annual nursing screening assessments were referred to the psychologist, who assessed mental health symptoms utilizing validated instruments. Annual ACE questionnaires were administered within 6 months of patients initiating care, often during the second visit to allow rapport-building and psychoeducation on childhood adversity. However, personnel reported inconsistent administration of the questionnaires due to limited staff resources and patient and personnel discomfort with sensitive questions, along with a lack of structured protocols for repeated screenings and information-sharing. Clinic nurses administered brief depression screener 31 and suicide risk screener 32 every 6 months, but no other routine trauma assessments systematically occurred.
Multiple providers across service categories conducted informal risk assessments of new patients during initial engagement, addressing domestic violence risk and/or suicidal or homicidal ideation. Several personnel of different positions dedicated extensive time in initial visits for formal and informal psychosocial assessments. Advanced practice providers and physicians highlighted the need for easier access to information on trauma history, mental health, and social determinants of health from these assessments. Additionally, individuals needing psychotropic medication management were referred to the consulting psychiatrist holding biweekly clinics. Research assistants regularly completed mental health questionnaires for research purposes, but results were not available in clinical electronic medical record.
Routine patient care occurred every 3 months, involving medical exam, lab work, psychosocial support, or research participation, if applicable. Community outreach staff utilized motivational interviewing to explore care barriers, 33 to provide education, and to de-stigmatize HIV in various community settings. While only the psychologist provided trauma-specific patient interventions, social workers expressed enthusiastic support for TIC implementation, with some having relevant trainings.
PM discussions with the patient representative group generated recommendations to improve trauma-responsiveness, including offering a menu of options for the order of services, limiting the number of provider encounters, and assigning navigators to escort patients during their initial visit. Interview findings were consistent with the sentiment that patient choice could be further built into workflow, stating “I think we could systematically assess patients for trauma and effects. I think we could listen to patients in terms of their preferences a little bit better. And I think related to that, change some procedures again with patient registration, with blood draws, assessment/triage, and integrate more choices into care. I think those are things we can do more quickly within the next year, as opposed to the larger issues, which are more about burnout and … provider support. I think those are larger issues that might take some more time” (Transcript 5).
Practices of Inclusivity, Safety, and Wellness
Limited efforts were identified as having been intentionally designed to gather and integrate personnel or patient experiences or promote professional quality of life. Staff described the hospital-wide satisfaction survey for patients but were uncertain about data usage or distribution. Similarly, employee satisfaction surveys were institution-wide, with no clinic-specific processes for assessing personnel satisfaction. Although informal patient verbal feedback prompted minor adjustments (eg, shortening patient general health screener), systematic patient feedback was not routinely gathered or integrated into clinic processes, as indicated by the PM. Moreover, staff valued voluntary patient input, noting a willingness to implement recurring suggestions. One person stated, “we get great feedback from our patients of how we should best navigate our clinic, or what could we do different that would help our patients. And we always recognize what they're saying and anything that's especially repeated by several different patients, like how can we make this better? So, that's why I was saying for every change, going back and tweaking those policies year in and year out to make it best for the patient and fit their needs” (Transcript 5). Overall, participants emphasized the importance of routinely and confidentially collecting patient feedback through annual satisfaction survey to guide clinic programming.
Training and Sustaining Trauma Responsiveness
Regarding workforce development, PM results indicated that numerous security guards and nursing administrators received Crisis Prevention and Intervention training every 1.5 years, to assist when a patient becomes escalated behaviorally. Providers reported independently pursuing professional development related to TIC, as no clinic-level group trainings were currently offered. They stated that leaders would have to prioritize such trainings and coordinate logistics to implement them effectively. Some personnel suggested expanding the social workers’ roles beyond case management to include more therapeutic modalities, highlighting reimbursement potential and enhanced mental health support.
Initiatives to promote professional quality of life were perceived to be limited, and examples primarily consisted of occasional institutional offerings like gifts or snacks, which were appreciated but insufficient and not specific to the clinic. Staff burnout and high levels of turnover were common topics, as was the need for more self-care training and institutional- and clinic-level initiatives to prevent burnout. Interview results corroborated that clinic personnel felt it was important to expand trauma training to better assist patients and improve professional quality of life. One person stated, “I think it [TIC] fits [at our clinic] … So yeah, I think it's extremely important… Because the personnel in the ID Clinic are very embracing of our patients and understand they've been exposed to a variety of circumstances. So, I think we already have that mindset” (Transcript 4). However, another person expressed uncertainty, asking, “What all comes as part of trauma-informed care?” The participant later indicated if they were advised on “What will be needed as in additional screenings […] it should be a good fit.” (Transcript 9).
Cultural Responsiveness
When asked about culturally responsive policies and procedures, personnel reported not currently having such policies or procedures in place. However, they reported the larger institutional system provides annual basic education about legal protections against discrimination, bias-awareness training, and opportunities to participate in group discussions and book clubs on culturally relevant topics. Personnel emphasized the importance of recognizing cultural differences in patient perspectives on experiences and treatment needs, underscoring concern about maintaining a destigmatizing environment. One person highlighted the lasting impact of stigma-related trauma on young people's daily lives, remarking, “The trauma around stigma […] is so impactful every single day to these young people as they grow up” (Transcript 9). Another person described how clinic administrators are responsive to this awareness: “in the hiring process, we also make sure that we're not going to hire anybody that would discriminate against someone…” (Transcript 13).
Discussion
We conducted PM discussion groups followed by one-on-one interviews and summarized results by OTR dimensions to identify current TIC practices and conditions and potential barriers and facilitators of TIC adoption in the pediatric HIV clinic.
Findings From the Case Clinic Mapped Onto OTR Dimensions
While both methods aided in identifying findings relative to Culture of Trust and Support and Collaboration and Empowerment, qualitative interviews elicited more in-depth insights, potentially reducing social desirability bias. For example, the interviews specifically revealed a perceived clinic-hospital disconnect. Different from personnel PM discussions, the patient PM discussions uniquely highlighted expanding patient choice in care flow.
Both methods appeared to effectively aid in identifying standard practices to Trauma Responsive Services, with PM discussion groups potentially presenting as more reliable through consensus. The clinic was consistently found to have limited trauma assessments and services. Although slightly varied, both methods identified patient-centered safety practices relative to the OTR dimension of Practices of Inclusivity, Safety, and Wellness, and pointed out a lack of systematic mechanisms for engaging patients and personnel in decision making or explicitly promoting staff wellness. Only one interview participant described the existence of a clinic-specific patient experience measure.
Additionally, both methods determined Training and Sustaining Trauma Responsiveness as inconsistent, not systematic, or nonmandatory. However, the interviews proved more effective for exploring Cultural Responsiveness, likely due to confidential, individual interactions. A more in-depth review of our findings relative to Cultural Responsiveness may be found in a separate, forthcoming manuscript.
Findings Contextualized
Findings on Culture of Trust and Support and Collaboration and Empowerment align with existing literature, reflecting equity and patient-centered practices compatible with TIC and consistent with what has been observed in other settings, including pediatric care 34 HIV care11,12,35 and other healthcare environments. 36 Additionally, the need for interagency cohesion is similar to other youth-focused care environments. 35
Consistent with other studies, we observed limited Trauma Responsive Services, particularly minimal routine screening for trauma despite broader mental health assessments. This aligns with a recent quantitative study that 80% of community-based HIV organizations in the Southern US provided mental health screenings, with only 43% screening for trauma. 13 These findings underscore the need to enhance existing services to meet the recommendations for universal mental health screenings issued by federal governing body recommendations—SAMHSA and Health Resources and Services Administration (HRSA), with the latter having an executive summary on the importance of addressing trauma as part of HIV care but no concrete requirements or recommendations are included as part of performance measures.37,38
Personnel suggested improving trauma assessment consistency by enhancing utilization of the ACEs questionnaire administration, 39 replacing with a more detailed post-traumatic stress disorder screener or the Positive Childhood Experience measure, 40 alongside leveraging social workers for trauma intervention services. PM findings, relative to trauma responsive services, add to a growing body of knowledge showing need for increased focus on routine conduct of trauma assessments in HIV care settings. There was a discrepancy regarding mechanisms for systematically collecting patient experiences, as one staff mentioned a clinic-specific tool, while most perceived a lack of systematic and confidential efforts for engaging patients or personnel as decision-makers. These mixed results are consistent with related literature; for example, findings from a quantitative survey indicated that 55% of HSOs in the region report having mechanisms for engaging clients as organizational decision-makers. 13 However, this concept is not clearly operationalized, and this lack of specificity raises important methodological questions about what constitutes systematic engagement. 13 The vagueness of the item phrasing, without specificity to show what those mechanisms are, and if results are integrated system-wide or among a small group of people, suggests potential issues with external validity. Importantly, PM helped us clarify this topic and highlight specificities of this concept to tease out what was perception (ie, personnel believe the environment is open enough that participants feel comfortable sharing when desired) versus if there were actually systematic, ongoing, and confidential mechanisms for collecting patient experiences and response to those observed. This methodological difference underscores the lack of attention to the community-engaged research continuum. 41 Thus, systematic and confidential efforts are needed to reach the demand, issued by the US Department of Health and Human Services (2023) for 30% of HIV care programs being community-designed by 2030. 42 Without attention to these methodological differences, the field could erroneously believe this is occurring and question its effectiveness, while it is not yet occurring to fidelity. Services designed without sufficient end-user engagement can lead to challenges in care. Without these efforts, there is no consistent mechanism for monitoring if all people feel safe in care institutions. Moreover, the need to elevate personnel voices in HIV clinics is particularly salient given the high rates of burnout and turnover. This was discussed in the case clinic and is consistent with extant literature.13,43
Observations in Training and Sustaining Trauma Responsiveness in the clinic mirrored a quantitative study, which showed only 44% of sampled community-based HIV organizations provided TIC training. 13 Additionally, despite 97% of the clinic patient population being racial minorities, PM failed to aid in identifying any specific clinic-based cultural responsiveness practices. This observed finding is important, as literature indicates that racial trauma is often overlooked during trauma screenings, 44 assessments, 45 interventions, 46 and as part of research.46–48 However, anti-Black racism is a documented driver of health inequities, 46 with youth of color reporting more racial trauma and having an increased likelihood for experiencing it than non-Black peers. Black youth with HIV, who bear a disproportionate trauma burden, could benefit from interventions to ameliorate racial trauma sequelae. Future research should explore specific antiracism communication practices that best promote health equity among patients and providers in the HIV clinic setting. 47
Transferability, Replicability, and Limitations
We have shared the tools we developed for this study so that future TIC champions could apply them, if helpful. Table 1 summarizes PM activities linked to quality criteria that are adaptable to various care settings, with Supplemental Table 1 providing essential TIC-specific discussion topics. Table 2 summarizes findings from the case clinic and draws comparisons between the 2 methods, showing areas where the PM method produced results similar to and different from standard qualitative interviewing. Table 3 provides recommendations for taking it forward following TIC-focused PM; these are action-focused implementation activities that align with OTR framework.
Organizational Trauma Resilience (OTR) Dimensions, Associated Activities, and Recommendations.
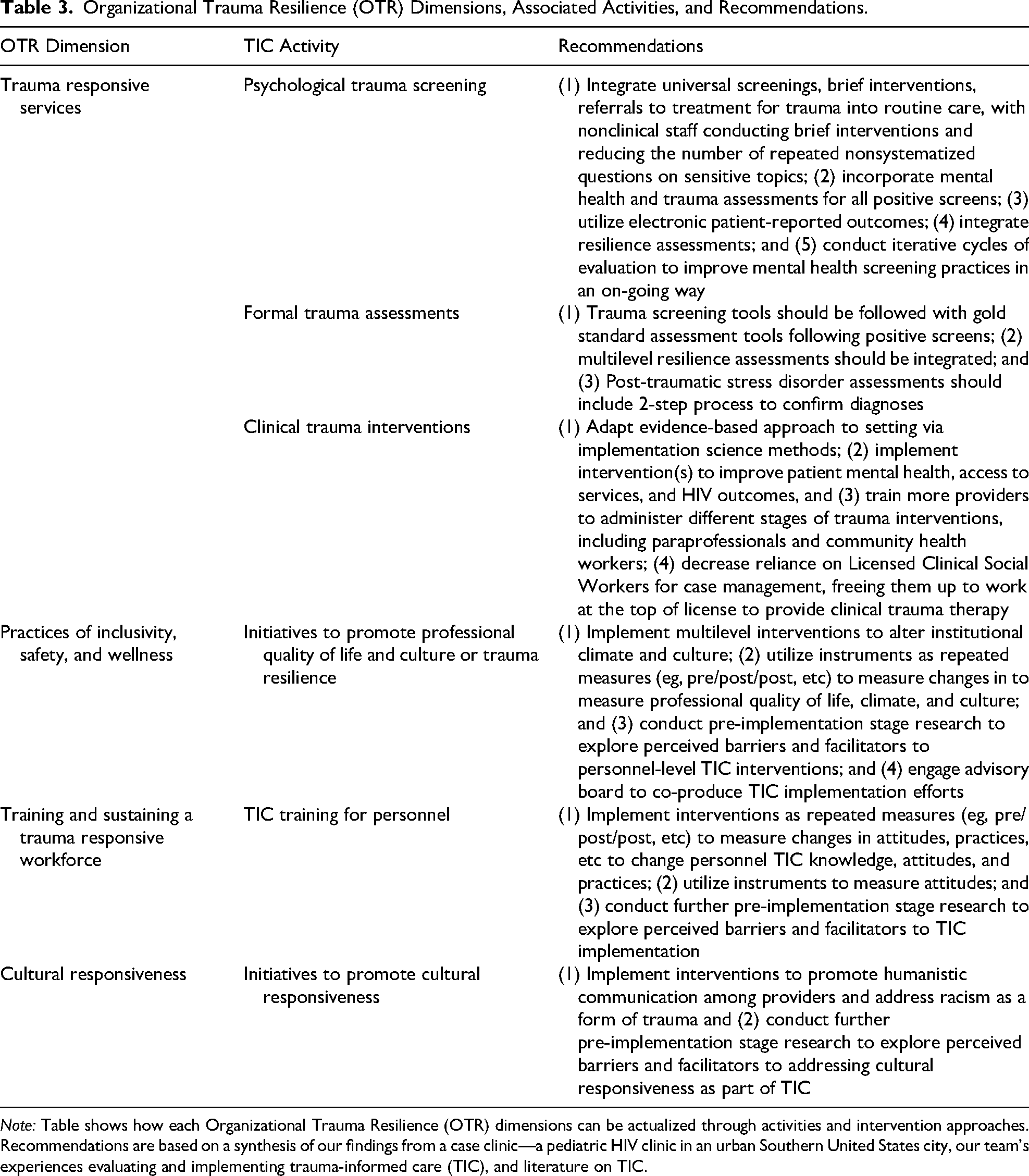
Note: Table shows how each Organizational Trauma Resilience (OTR) dimensions can be actualized through activities and intervention approaches. Recommendations are based on a synthesis of our findings from a case clinic—a pediatric HIV clinic in an urban Southern United States city, our team's experiences evaluating and implementing trauma-informed care (TIC), and literature on TIC.
We have drawn comparisons of our findings from the multimethod approach with those of other methods to underscore several important strengths and limitations of this method. The PM method proved to (1) probe most dimensions of OTR; (2) promote a collaborative and shared understanding of standard of care related to TIC, which one-on-one interviews do not accomplish; (3) engage diverse participants for greater triangulation (compared with the smaller samples of primarily clinic personnel only for interviews); (4) enable fluid discussion of topics, whereas interviews do not promote this participatory component, and surveys do not provide a reflexive platform in which further details may be explored or clarified; (5) enhance experiential cohesion on topics that one-on-one interviews and surveys would not satisfy; (6) present clear visual summaries; (7) offer efficient and cost-effective administration (PM activities took about 12 h to complete, compared to approximately 95 h in key informant interviews versus); 49 and (8) serve as a quality improvement tool without IRB requirements of interviews.
Several limitations presented for this study. Initial mixed-group PM discussions seemed to dissuade candid discussions, likely due to power differentials. Later PM discussions, grouped by job roles, seemed to promote more fluid dialogue. Because of these group discussion limitations, certain topics requiring more confidential settings, including the OTR dimensions of Culture of Trust and Support and Collaboration and Empowerment, were not explored using these methods, and the group dynamics could have contributed to potential participant bias, specifically self-selection bias. However, we believe the follow-up qualitative interviews allowed for triangulation of PM findings, potentially reducing social desirability bias. In our case, it appeared advantageous that PM results could be utilized to inform the key informant interview guide as a follow-up method. Finally, results are limited by the single-site design, which constricts generalizability, even though the TIC PM method is hypothesized to be generally applicable for use in other Ryan White-funded clinics.
Conclusions
We conducted a multimethod study with a pediatric HIV clinic to clarify health system complexities and identify barriers and facilitators to implementing TIC. PM discussion groups effectively mapped many dimensions of OTR, and interviews provided deeper insights while potentially reducing social desirability bias. Although some limitations presented, PM discussions allowed us to foster a collaborative consensus and shared understanding of how the clinic relates to TIC and important considerations for its implementation. The PM process can be an important first step to build cohesion and support for TIC implementation in healthcare settings while generating a context-driven guide for further topics to probe via follow-up research activities (ie, findings from the PM appeared to enhance the content of follow-up interviews). Future research should expand the multimethod approach to multiple sites. Additionally, personnel in the case clinic could consider building on study findings by implementing TIC via action steps laid out in Table 3. Some of these activities include training clinic and hospital personnel on trauma response and cultural responsiveness, integrating universal trauma exposure and effect screenings, providing trauma-specialized interventions, and measuring personnel and patient outcomes over time to assess the impact of TIC.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251382269 - Supplemental material for Pre-implementation Stage Research to Guide Trauma-Informed Care for Youth With HIV in the Southern US: A Multimethod Study
Supplemental material, sj-docx-1-jia-10.1177_23259582251382269 for Pre-implementation Stage Research to Guide Trauma-Informed Care for Youth With HIV in the Southern US: A Multimethod Study by Leslie Lauren Brown, Megan Leigh Wilkins, Latrice Crystal Pichon, Jamie Linn Stewart, Robert Kenneth Douglas McLean, Jessica McDermott Sales, Carolyn Marie Audet, Samantha Veronica Hill and April Christine Pettit in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251382269 - Supplemental material for Pre-implementation Stage Research to Guide Trauma-Informed Care for Youth With HIV in the Southern US: A Multimethod Study
Supplemental material, sj-docx-2-jia-10.1177_23259582251382269 for Pre-implementation Stage Research to Guide Trauma-Informed Care for Youth With HIV in the Southern US: A Multimethod Study by Leslie Lauren Brown, Megan Leigh Wilkins, Latrice Crystal Pichon, Jamie Linn Stewart, Robert Kenneth Douglas McLean, Jessica McDermott Sales, Carolyn Marie Audet, Samantha Veronica Hill and April Christine Pettit in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582251382269 - Supplemental material for Pre-implementation Stage Research to Guide Trauma-Informed Care for Youth With HIV in the Southern US: A Multimethod Study
Supplemental material, sj-docx-3-jia-10.1177_23259582251382269 for Pre-implementation Stage Research to Guide Trauma-Informed Care for Youth With HIV in the Southern US: A Multimethod Study by Leslie Lauren Brown, Megan Leigh Wilkins, Latrice Crystal Pichon, Jamie Linn Stewart, Robert Kenneth Douglas McLean, Jessica McDermott Sales, Carolyn Marie Audet, Samantha Veronica Hill and April Christine Pettit in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Abbreviations
Acknowledgments
Headliners Memphis, Connect to Protect Memphis (C2P), UAB Implementation Science Hub, Tennessee Center for AIDS Research P30AI110527, and Winston Gu for his support and assistance in technical aspects of writing.
ORCID iDs
Ethics Approval and Informed Consent Statement
Ethics approval was provided by Meharry Medical College Institutional Review Board (21-07-1105) and University of Memphis (PRO-FY2022-201), with St. Jude ceding to Meharry as IRB of record and in accordance with the Declaration of Helsinki. All methods were carried out in accordance with these IRB guidelines and regulations. The Meharry Medical College Institutional Review Board (21-07-1105) deemed process map activities did not meet the criteria for research and waived the need for informed consent from subjects.
Authors’ Contributions
Authors contributed the following: LLB, MLW, LCP, JLS, JMS, SVH, ACP, and the UAB IS hub conceived the article. LLB wrote the first draft. LLB, MLW, LCP, JLS, RKDM, and ACP edited the PM figure; LLB, MLW, LCP, JLS, RKDM, JMS, CMA, SVH, and ACP edited the drafts and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by a supplement to the Tennessee Center for AIDS Research through the National Institute of Allergy and Infectious Diseases P30AI110527. LLB acknowledges salary support from K01MH131471-01A1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Material
Data sharing is available for this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.