
Abstract
People with a previous HIV diagnosis (PWHDx) who are out of care (OOC) (PWHDx OOC) represent a significant but often overlooked population in the United States, accounting for nearly half of new HIV transmissions annually. Emergency departments (EDs), frequently accessed by PWHDx OOC for unscheduled care, are uniquely positioned to identify and re-engage these individuals in HIV care. While ED-based HIV efforts have traditionally focused on diagnosing new infections, this paper reviews and evaluates 3 models EDs can implement to identify PWHDx OOC: routine HIV screening, health information exchange, and electronic health record alerts. We describe each model using examples from the literature, assessing their feasibility, scalability, and effectiveness in identifying patients and determining care status. By synthesizing current approaches, this paper highlights practical and policy-relevant pathways for expanding ED-based HIV services beyond diagnosis, offering concrete guidance for healthcare systems aiming to meet the national “Ending the HIV Epidemic” goals.
Keywords
Introduction
In 2019, the United States (US) Department of Health and Human Services announced a plan for Ending the HIV Epidemic (EHE) with a goal to reduce new HIV infections in the US by 90% by 2030.
1
The EHE initiative identifies 4 key strategies: (1) “
The EHE plan includes re-engagement to care for people with a previous HIV diagnosis (PWHDx) who are out of care (OOC) (PWHDx OOC) as one of its strategies under its second pillar, “Treat,” underscoring the importance of efforts in this area. Re-engagement encompasses a variety of strategies, including data to care (D2C), linkage to care, and case management, and is vital to preventing new infections. 2 Of the 1,018,000 PWHDx in the US, it is estimated that 470,000 (46%) are OOC. 3 Because of low adherence to ART and low rates of viral suppression, PWHDx OOC are responsible for approximately 50% of new HIV transmissions annually.4,5 Although many PWHDx are not engaged in routine HIV care, they often receive unscheduled care in emergency departments (EDs), making EDs a prime location for the identification and linkage of PWHDx OOC.6,7,8
Over the past 20 years, US EDs have played an important role in EHE efforts,9,10,11 primarily through the implementation of screening programs intended to identify undiagnosed PWH. More recently, EDs have expanded services to address EHE strategies beyond “Diagnosis,” including integrating HIV prevention services for HIV negative patients at increased risk for acquiring future infection,12,13,14 identifying acute HIV infection, 15 providing same day antiretroviral treatment (ART) for patients newly diagnosed with HIV infection,11,16-18 and identifying and linking PWHDx OOC. 19
Understanding how EDs can best identify PWHDx OOC, implement re-engagement to care strategies, and evaluate the outcomes of these services, are important areas for implementation science research which may influence EHE policy. While linkage to care, initiation of ART, and achieving and maintaining viral suppression are clinically important outcomes, this discussion will focus on ED-based strategies to identify PWHDx OOC as the first step in the re-engagement to care cascade. Using examples reported in the literature, we describe 3 models used by EDs, including the: (1) routine screening model; (2) health information exchange model; and (3) electronic health record (EHR)-based alert model. Though implemented using different strategies, all models first identified the population of ED PWHDx and second determined their care status to be either in care or OOC (Figure 1). In addition to describing these models, the strengths and weaknesses of each approach will be discussed, as well as additional considerations related to testing, care status assessment, linkage to care, and rapid treatment with ART.

Emergency Department Strategies to Identify and Determine Care Status of People Living With HIV.
Routine HIV Screening (RHS)
Since 2006, the Centers for Disease Control and Prevention (CDC) has recommended the integration of routine, universal (non-targeted) HIV screening (RHS) in the ED setting. 20 These expanded recommendations were intended to diagnose new cases of HIV in eligible patients who do not opt-out and who have not been previously diagnosed. In fact, protocols often have explicit criteria excluding PWHDx from screening, with conventional thinking that repeat testing lacks clinical value and adds unnecessary cost. How frequently ED HIV screening programs test PWHDx is dependent on the specifics of the screening policies, such as the fidelity of consent processes and exclusion criteria set by the program. For example, some health care systems have no screening rule out method in place to prevent PWHDx from being re-tested, while other health care systems may set screening algorithms to exclude PWHDx who are known to the system based on previous lab results or medical history. Despite these exclusions, ED-based HIV screening programs often uncover PWHDx through unintentional repeat testing. Importantly, many of these patients are found to be OOC and require linkage to HIV services and treatment. In fact, HIV screening programs often identify more PWHDx OOC through repeat testing than they do new diagnoses.16,21,22
We highlight 3 examples of ED-based HIV screening programs and the unintended identification of PWHDx (Table 1). At the Harris Health System (Harris County, TX), an HIV screening test was automatically ordered if blood was drawn or an IV was placed for ED patients ≥16 years of age who did not opt out. 21 No exclusion criteria for known HIV status were used. Between 2009 and 2012, the program performed 202,767 HIV tests with 2843 confirmed and de-duplicated positives (1.4% positivity). Among the final study cohort (n = 2723), patients newly-diagnosed with HIV (n = 655) made up 24% of patients with a positive test while PWHDx (n = 2068) made up 76% of patients with a positive test. Of the 2068 PWHDx re-identified through screening, 41% were in care (n = 854) while 59% were OOC (n = 1214). Overall, 45% of patients testing positive in this routine HIV screening program were OOC (n = 1214/2723).
Emergency Department HIV Screening Program and Unintentional Identification of PWHDx.

Flash, C.A., et al., J Acquir Immune Defic Syndr, 2015. 69 Suppl 1(0 1). 21
White, D.A.E., et al. Open Forum Infect Dis, 2023. 10(7). 16
Maldonado, S.D., et al; AIDS Patient Care STDS, 2022. 36(2). 22
At 2 EDs within the Alameda Health System (Alameda County, CA), an HIV screening test was automatically ordered when blood-based laboratory tests were ordered for patients ≥18 years of age who did not opt out. 16 Patients were excluded from HIV testing if they were identified as HIV positive (based on the results of a previously reactive HIV antigen/antibody test, detectable HIV viral load, or “HIV” in past medical history field). Between July 2021 and June 2022, the EDs performed 10,606 HIV tests with 152 confirmed and de-duplicated positive results (1.4% positivity). Patients newly diagnosed with HIV (n = 36) made up 24% of those with a positive test while PWHDx (n = 116) made up 76% of those with a positive test. Of the 116 PWHDx re-identified through screening, 51% were in care (n = 59) while 49% were OOC (n = 57). Overall, 38% of patients testing positive in this RHS program were OOC (n = 57/152), again demonstrating the utility of this approach in identification of PWHDx who require linkage to care.
At the University Hospital ED (Newark, NJ), an HIV screening test was automatically ordered for patients unless they opted out or had been tested in the past 12 months. 22 Retrospective chart review was performed for patients ≥18 years of age who tested positive between January 2015 and November 2018. Among the 438 patients with positive HIV tests, 25% were newly diagnosed (n = 111) and 74% were PWHDx (n = 326) (data missing for one patient). Of the PWHDx, 68% were in care (n = 222) and 32% (104) were OOC (n = 104). Overall, 24% of patients testing HIV positive through screening were OOC (104/438).
In all 3 of these ED-based, routine, opt-out HIV screening programs, the proportion of patients identified with a new HIV diagnosis was approximately 25% of the total population testing HIV positive and was similar or considerably lower than the proportion of patients identified as PWHDx OOC, and this was true regardless of whether criteria excluding repeat testing for PWHDx were in place. Thus, in addition to identifying newly diagnosed HIV, ED-based RHS programs play an important role (albeit an unintentional one) in identifying large numbers of PWHDx OOC.
Health Information Exchange (HIE)
A second model for identifying ED PWHDx OOC is the use of a HIE.23,24 A HIE is a 2-way health information-sharing platform that utilizes data gathered for HIV surveillance by health departments for real-time use in clinical settings. 23 For example, an HIV surveillance database, filtered using structured criteria to generate a list of PWHDx believed to be OOC, is made available to clinical staff to promote re-linkage efforts.
We highlight 2 examples from the literature of EDs that participated in HIEs to identify PWHDx OOC. In 2017, the Grady Health System (Atlanta, GA), in partnership with Georgia Department of Public Health, implemented the Georgia Public Health Information Exchange (GPHIE) program. 23 Using routinely collected surveillance data, an OOC watch list for all PWHDx without CD4 or viral load testing in the previous 14 months was generated and updated regularly. This OOC watch list was cross-referenced in real time and matched with patients as they registered for care in the Grady ED, generating a clinical alert for the ED social worker to engage with the patient, ascertain care needs, and provide linkage support. Over a 1-year study period, 166 ED patients generated an alert, of which 147 were OOC (89%).
The Louisiana Public Health Information Exchange (LaPHIE) is another example of the use of an HIV HIE applied in the clinical setting. In the LaPHIE, a statewide HIV surveillance database of PWHDx OOC, defined as those who have never entered care or those without a CD4 or viral load in >12 months, was linked with the registration and EMR system of an integrated health network system comprised of 7 safety-net hospitals, including EDs. 24 In this program, if a patient in the OOC database registered for care in the ED, an alert was triggered within the clinician workflow, notifying staff of a patient's specific HIV-related care needs, including need for HIV treatment and linkage. Although data specific to ED outcomes were not reported, over a 2-year period, the LaPHIE identified 345 PWHDx OOC within the health care system.
Electronic Health Record Alerts (EHRa)
The third model for identifying ED PWHDx is the use of the EHR to alert staff when a PWH is registered in the ED.25,26 With this model, EHR-based algorithms query medical records for ED patients to identify those who are PWHDx. Staff are alerted by the EHR and work to determine any HIV-related linkage and treatment needs.
We report 2 examples of ED programs which utilize EHRa (Table 2). In the first, Ruffner et al describe an EHRa model used alongside an ED HIV screening program to systematically identify PWHDx who may need HIV-related services. 25 The EHR was modified to search the records of all ED patients for non-negative HIV test results, an HIV diagnosis, or HIV in the problem list. If any of these criteria were present, existing program staff (which included health promotion professionals) were alerted via text and an EHR inbox notification (ie, EPIC in-basket). Staff, upon receiving notification (and if patients were still in the ED) reviewed the medical record and evaluated the patient's need for additional testing and linkage to care. In a 1-year period, 104 PWHDx OOC were identified and 32% were linked to care.
Electronic Health Record Alerts to Identify PWHDx.

Ruffner, A.H., et al., Am J Emerg Med, 2020. 38(9). 25
Ridgway, J.P., et al., J Public Health Manag Pract, 2019. 25(3): p. 270-273. 26
At the University of Chicago, a similar EHR model to identify PWHDx was implemented in both the ED and inpatient settings. 26 Program staff accessed a daily report of registered patients identified as PWHDx using the following criteria: laboratory evidence of positive HIV antibody test or detectable HIV viral load; “HIV infection” listed in the past medical history or problem list; and/or prescription for ART (excluding for PrEP). Staff then used a combination of laboratory data, patient self-report, and information obtained from a Department of Public Health HIV surveillance database to determine care status. A trained HIV navigator met with patients in person (ED or inpatient) or over the phone (after ED visit) and assisted with linkage to HIV care and additional supportive services, as necessary. Over 14 months, this model identified 393 PWHDx, of which 56 (14%) were OOC. In comparison, a parallel HIV screening program identified 17 patients with a new diagnosis of HIV infection during this time.
Each of these 3 models has strengths and weaknesses with regards to identifying and determining care status which are important to consider. Table 3 summarizes the strengths and weaknesses of each model which are discussed in detail below.
Summary of Emergency Department Strategies to Identify Out-of-Care People Living with HIV: Strengths & Weaknesses.
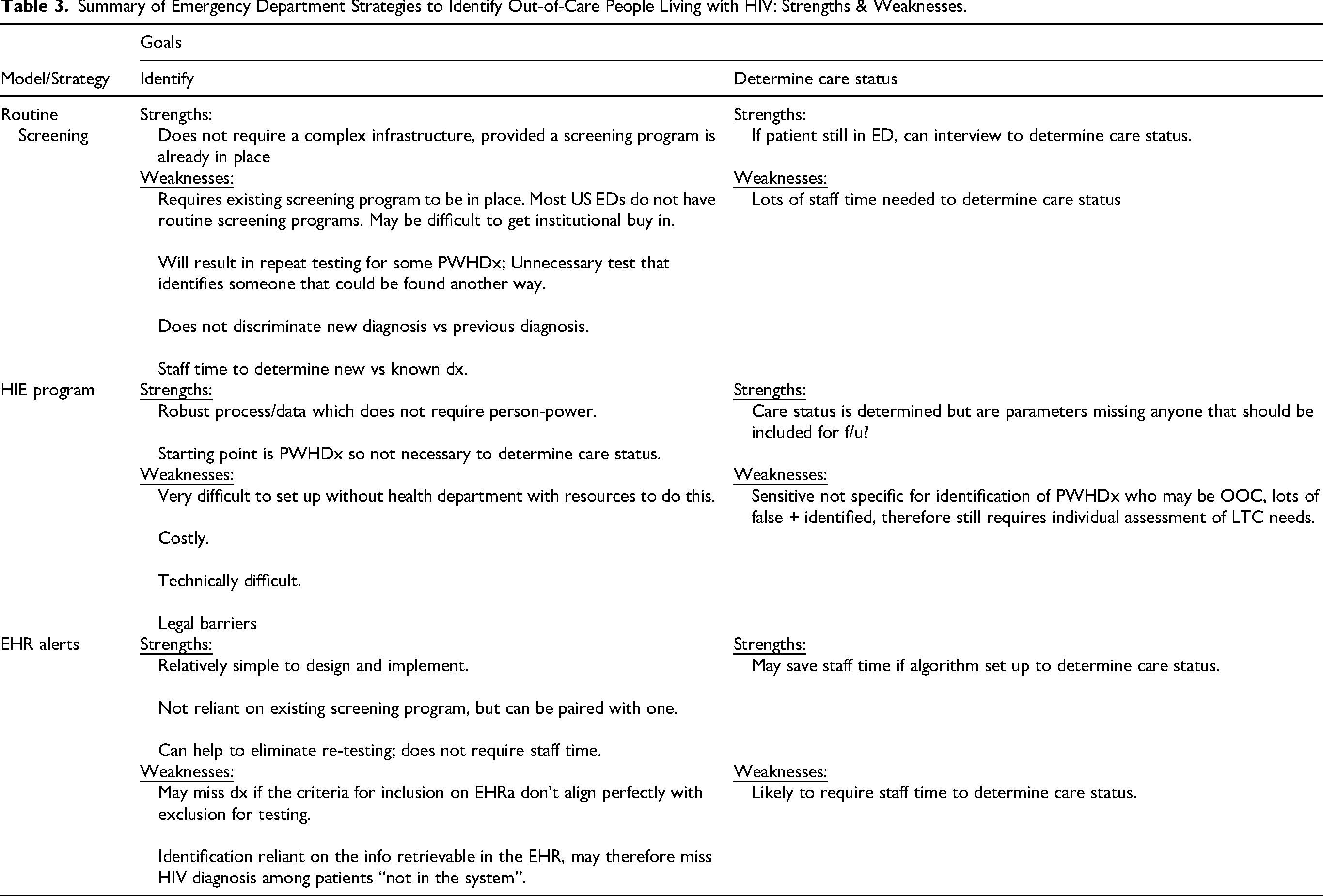
RHS: Strengths & Weaknesses
One strength of RHS as a strategy to identify and link PWHDx OOC is that, in EDs where RHS is already in place, existing linkage pathways and navigator staff who assist newly diagnosed PWH can be leveraged to provide these same services for PWHDx OOC. 6 Additionally, many ED RHS programs utilize EHR algorithms to automatically assess eligibility for screening and these can be used to generate real-time notifications for those patients excluded by these algorithms (because they are known to the health care system as PWHDx), allowing existing RHS programs to immediately implement adjunct EHRa programs to systematically identify PWHDx. In this scenario, only PWHDx not already known to the health care system and who do not opt out would be repeat tested and could then be assessed for linkage needs. Admittedly, some PWHDx would still be re-tested in this model, given the fractured healthcare information systems in the US where PWHDx may appear as “new” cases in another healthcare system.
Unfortunately, most US EDs still do not provide RHS, despite recommendations calling for widespread implementation by the CDC and others for over 20 years.27,28 Some EDs have instead opted for targeted screening, which has found support in the literature and may be a better fit in certain settings. 29 Although challenges to implementing ED-based RHS remain, integration into standard ED processes has been greatly facilitated by the near-universal adoption of EHR systems and laboratory technologies which can automate screening and provide efficient, cost-effective rapid test results. These advancements minimize barriers to implementation and should allow adoption of RHS to more EDs.11,30 Additionally, targeting EDs in EHE priority jurisdictions with teaching hospital affiliations may prove to be an efficient strategy for expanding RHS to a limited number of EDs with the greatest impact.31,32
RHS models require repeat testing (of patients not known to the health care system) to identify PWHDx, which may be viewed as costly, redundant, and unnecessary. The actual monetary costs incurred by a hospital to perform repeat testing for ED PWHDx, however, is relatively small. For example, if all PWHDx registered for care (estimated HIV prevalence of 0.6%) in an average sized ED (35,000 visits/year) were retested, this equates to only a few hundred tests annually, negligible when put into context of screening programs that may perform tens of thousands of tests. 33 This is especially important because repeat testing of PWHDx can be used as the springboard for re-engaging those in need. 21 Furthermore, the added benefit of identifying and linking to care PWHDx OOC, in the form of a reduction in ED readmissions and an increase in ED throughput, should quickly outweigh the cost of re-testing PWHDx.7,34
In RHS programs, determining whether each positive test represents a newly diagnosed PWH or a PWHDx who is in care or OOC, requires a clinical assessment. This typically involves collaboration between the treating physician and a patient navigator, who either obtains this information from the patient, chart review, or the health department. This can be time-consuming, costly, and require case management, which often spans several days to weeks. A simple laboratory method could be employed to ascertain the care status of PWHDx and reduce the need for manual intervention. This involves conducting a qualitative viral load test following each reactive HIV test, the outcome used by staff to determine whether the patient is likely receiving care (indicated by an undetectable viral load) or potentially not in care (indicated by a detectable viral load).
Lastly, while RHS programs have been shown to identify many PWHDx in EDs, most programs test fewer than 35% of age-eligible patients. As a result, relying solely on RHS in EDs would likely miss a large number of OOC PWHDx.35-38
HIE: Strengths & Weaknesses
The primary strength of the HIE model lies in its use of comprehensive HIV surveillance data from local and state health departments, which is considered the gold standard for infectious disease data. Though not without its challenges, the HIE model signifies a vital partnership between health departments and clinical care systems, and once established, it serves as an effective strategy for identifying PWHDx OOC.
Because the very basis of a surveillance-based HIE process is the identification of PWHDx OOC, care status determination is largely automated, a major strength of this model. However, HIEs are designed to be highly sensitive, generating few false negatives (PWHDx who are OOC being missed), but they lack specificity, and thus generate false positives (patient flagged as PWHDx OOC but who are actually in care). Even with robust HIE models, confirming OOC status and linking those in need to HIV care requires intensive investigation and support by dedicated staff.
Thus, one of the major strengths of the HIE approach—automated care status determination—may also be a potential weakness. If any of the parameters set for care status determination are missing or too stringent, PWHDx who are indeed OOC might be missed and/or PWHDx flagged as OOC may actually be in care. For example, in an attempt to avoid over-estimation of PWHDx OOC, the GaPHIE system increased the period for lab look-ups from 12 months used by their predecessors in LaPHIE to 14 months. Nonetheless, confirmation of care status will still be required, but for a smaller number of patients compared to RHS.
The other major weakness of the HIE model is that a strong data infrastructure must be in place at the health department. The setup for HIE is both time- and resource-intensive and few health departments have implemented HIEs in their jurisdictions. First, health departments must maintain databases, ensuring that data are up-to-date and accurate. Second, data-sharing infrastructure must be developed and implemented, which requires complex data sharing procedures, legislative compliance, and configuration with hospital-based electronic record systems, all of which necessitate substantial up-front capital, expertise, and ongoing support. Unfortunately, many health departments and hospital systems do not have the required resources to implement and sustain this model. The now defunct LaPHIE provides an unfortunate example of what happens when resources to maintain this infrastructure are not sustained.
EHRa: Strengths & Weaknesses
The EHRa approach has several strengths. Used primarily as an automated tool to identify ED PWHDx, it is relatively simple to design and implement, is not reliant on an existing screening program, can be tailored to a site's unique characteristics and available data, and does not rely on clinicians to remember to ask patients about their HIV status and make individual referrals.
The EHRa has the ability to rapidly identify nearly all ED PWHDx, minimizing the number of missed opportunities for re-engaging those who are OOC. However, the ability of an EHRa to identify PWHDx relies on prior testing and past medical history data being retrievable and accurate and is usually restricted to information available within a health care system's database. PWHDx new to a system, or whose past medical history field is not updated, or who do not have an HIV test on record, will not be identified.
The 2 examples of EHRa that we describe identified ED PWHDx but did not determine their care status as in care or OOC, a step that must be performed by additional staff. The burden on staff to determine care status could be reduced by more advanced EHR systems that incorporate HIV clinic visit history, detectable viral loads, and other clinical indicators such as ART prescription completion. 39 To the extent that the EHRa model includes an estimation of care status, this can be a major strength, as it would save staff time on this task. However, if the parameters for determining OOC are inaccurate, there is potential to misclassify PWHDx who actually need linkage services. Thus, while a potential weakness of this strategy might be that staff time is required to determine care status, this could be a strength to the extent that a dedicated HIV navigator will more accurately identify a patient's need for linkage to care than an algorithm.
Regardless of whether an EHRa automatically stratifies PWHDx by care status, some dependence on staff is necessary to engage with patients and assist with linkage efforts, which requires funding to sustain. Deploying ED navigators to deliver a range of HIV-related services—such as prevention assessments, counseling, and linkage to care for both newly diagnosed individuals and those PWHDx—may represent an efficient use of resources.
Other Considerations
Defining and Determining OOC
Characterizing PWHDx status as OOC necessitates an accepted definition and a method for obtaining the information to make this determination. Definitions of OOC and the strategies employed for characterizing care status, however, vary across programs. Programs may perform chart review of the patient's medical record, query local health department records for D2C surveillance information, interview patients, or use a combination of these approaches. Surrogate laboratory data used to classify PWHDx OOC often includes review of HIV-related tests. For example, patients without an HIV viral load or CD4 test within the previous 12 months implies the patient is not engaged in HIV care. Alternatively, patients with detectable HIV viral loads within the past year may indicate that they have seen a care provider but are not taking ART. Although helpful in assessing the likelihood that PWHDx are OOC, relying on D2C, and other surrogate markers of retention, may be inaccurate.40,41 Regardless of the initial strategies used, a direct interaction between a clinician or navigator and the PWHDx is required to assess whether a patient needs to be relinked to HIV care.
Additional Testing Needs
Although PWHDx OOC do not need additional testing during their ED visit to receive navigation resources, baseline and HIV-related testing may be justified for select patients. Confirming the HIV diagnosis may be needed for patients relocating from a different health care system and enrolling in insurance programs, and obtaining baseline CD4, viral load, renal function, hepatitis serologies, and HIV genotype testing may facilitate ART and are often requested by treating HIV clinicians.
Rapid Initiation of ART (Rapid Start)
Rapid ART, defined as initiating ART as soon as possible after an HIV diagnosis is made, has been shown to improve linkage to and retention in care, reduce time to viral suppression, decrease viral transmission, and improve morbidity and mortality.18,42-46 Health departments often set time to ART benchmarks of 3, 5, or 7 days for clinics within their jurisdiction that provide HIV care. Recent evidence shows that initiating rapid ART in the ED for newly diagnosed PWH is feasible, well-tolerated, safe, and plays a key role in facilitating linkage to care. 16
We believe that ED PWHDx OOC would experience similar benefits from rapid ART as those who are newly diagnosed. Because PWHDx OOC often have ART use history 16 and because treatment-experienced patients may be at higher risk for the development of ART resistance, referral to an HIV specialist for clinical evaluation prior to treatment is often recommended. 47 Future ED rapid ART treatment protocols should consider strategies to facilitate restarting ART among treatment-experienced patients who are OOC, including straightforward workflows and real-time access to specialist consultation to assist in the safe re-initiation of treatment.48,49 For patients with prior ART use, clinic-based protocols may be adapted for ED use in which a reinforced regimen is empirically started and coupled with viral resistance testing.47,50
Linkage to Care Challenges
Linkage to care for ED PWHDx is resource-intensive, time-consuming, and best when supported by separately-funded HIV navigators who work in parallel with ED clinical staff. Although expanding the role of existing internal staff (ie, social workers, case managers) may be considered, it is unrealistic to expect emergency physicians to perform these services.
Compared with ED PWH who are newly diagnosed, ED PWHDx OOC have lower linkage to care rates and require more extensive outreach and navigation resources. 22 These differences may be attributable to the significant barriers impeding re-engagement efforts faced by ED PWHDx OOC, including housing insecurity, limited transportation, substance use disorders, mental health illnesses, stigma, and denial.19,23,51 These complex challenges mean navigators often provide services over longer periods of time, simultaneously addressing patients’ social determinants of health, often through coordination between social services agencies, street medicine teams, insurance enrollment providers, local health jurisdictions, and substance use and mental health specialists. 11
An important aspect of patient navigation for linkage to care includes tracking and monitoring each patient's status throughout the care cascade. To the extent that support for navigation is externally funded, intensive data reporting is expected. And even when this is not the case, there will be requirements for reporting to local health departments for surveillance purposes. Staff performing patient navigation duties need support in database development and report-building to perform these duties optimally. Understanding the care continuum differences for ED PWHDx compared to those who are newly diagnosed, in terms of linkage attempts, time to ART, time to viral suppression, and retention in care, are important metrics that require monitoring to inform interventions for closing care continuum gaps.
Directions for Future Research
EDs can play an important role in the identification of PWHDx OOC, potentially re-linking this population to care. Ultimately, health systems will have to determine which strategies are most efficient, feasible, and sustainable. Future research could help to inform these decisions.
Current research and clinical experience tells us that although many PWHDx may not engage in routine HIV care, they often receive unscheduled, episodic care in EDs. Epidemiologic studies are needed to better determine the scope of utilization by PWHDx OOC in US EDs. This is a necessary first step to allocate the appropriate resources to identify ED PWHDx, assess their care status, and provide the resources to link them back to care, when necessary.
Determining optimal methods for identifying and assessing care status are also needed, including comparisons between models. The accuracy of specific models, such as the EHRa model, to not only correctly identify an ED patient as HIV positive but to further characterize them as in care or OOC using data retrievable from the EMR, such as HIV clinic visits, HIV-related lab tests, and pharmacy records to confirm recent receipt of ART prescriptions, requires evaluation. It would be helpful to see data both from sites using EHRa in tandem with RHS, as well as those using EHRa in the absence of RHS. Important questions include how to set up an EHRa optimally and what logistics are involved, as well as an assessment of whether PWHDx are being missed by being excluded from RHS under the assumption that they will be captured by EHRa.
To ensure clinicians interested in expanding their HIV-related services to re-engage PWHDx, it is essential to make the logistics of how EDs identify and link PWHDx to care accessible. Too often, publications prioritize a standardized structure for submissions, which does not afford the space for detailed descriptions of how programs are set up. This leaves those looking to implement a program without nuanced details of how to actually do it. This area of inquiry is therefore well suited to implementation science research, which supports the inclusion of program descriptions in publications. 52 Expanding existing online toolkits (which were originally designed to facilitate the integration of RHS into EDs) to include best practice strategies to identify PWHDx OOC is recommended and may help reach a wider audience. 53 Technical assistance programs should highlight the importance of the ED as an important clinical venue for the identification and re-linkage to care of PWHDx. 54 Lastly, more data is needed on ED PWH who are newly diagnosed compared to PWHDx and for PWHDx who are in care compared to those who are OOC. Understanding how these populations differ from each other may help inform re-engagement strategies.
Recommendations for Models Moving Forward
While this paper has focused on ED-based strategies for identifying PWHDx OOC, it is important to remember that this work doesn’t exist within a vacuum, but rather, exists within a larger framework of efforts to identify all PWH, including those who are PWHDx and those who are unaware of their diagnosis. To that end, we want to emphasize that no strategy for identifying PWH should be thought of as existing optimally when implemented independently. Rather, we acknowledge that organizations will likely need multiple approaches, including strategies to identify HIV among those previously undiagnosed and strategies to identify PWHDx who may be OOC.
Regarding the identification of PWHDx, we believe the EHRa model to be the most efficient, feasible, and generalizable model, which can be easily replicated and tailored for use in most US EDs. This is because the EHRa model does not require an existing HIV screening program to be in place, does not rely on external data or partnerships with health departments, and can leverage basic EHR technology to automatically identify PWHDx, even providing additional information used to suggest that a PWHDx may be OOC.
Conclusion
In the US, there are nearly 500,000 PWHDx OOC, 3 times the number of patients with HIV who are unaware of their diagnosis. 55 Re-engaging these individuals to care and treatment is vital to EHE efforts, as they often have unsuppressed viral loads and account for a majority of HIV transmissions.4,5 Given the high ED utilization by PWH, the ED represents a strategic setting for the systematic identification of PWHDx, assessment of their treatment needs, and re-engagement to care. A variety of models, including RHS, EHRa, and HIE, can serve as a foundation for the development of institution-specific programs, but will require sustained public health investment and partnership.
Footnotes
Acknowledgments
The authors would like to acknowledge the invaluable review and input provided by colleagues at Gilead Sciences Inc.: Monique Rucker, Jamie Mignano, and Hilary Armstrong.
Author Contributions
BH/DW: study concept and design, drafting of the manuscript, critical revision of the manuscript for important intellectual content, and acquisition of funding. NG: critical revision of the manuscript for important intellectual content.
Declaration of Conflicting Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Consulting fees were paid to BH and DW by Gilead Sciences Inc. to develop this manuscript. DW/BH retained final control over the content.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Gilead Sciences Inc.