
Abstract
Background
Human immunodeficiency virus (HIV) cases are rising in Central Asia and Kazakhstan. People living with HIV (PLWH) in Kazakhstan are at heightened risk of severe COVID-19. We conducted a study to evaluate determinants of COVID-19 vaccine uptake among PLWH in Kazakhstan.
Methods
In this cross-sectional study, 196 PLWH were recruited from the Almaty City AIDS Center (July 2022-January 2023). We used logistic regression to evaluate how multilevel factors are associated with COVID-19 vaccine uptake among PLWH in Kazakhstan.
Results
COVID-19 vaccine non-uptake was associated with higher HIV stigma scores (AOR = 1.08, 95%CI:1.02,1.16, P = 0.017), a lower level of education (AOR = 2.53, 95%CI: 1.04,6.17, P = 0.0412), and never receiving the flu vaccine (AOR = 15.64, 95%CI:3.66,66.89, P = 0.0002). Participants with at least mild anxiety symptoms (AOR = 0.15, 95%CI:0.03,0.64, P = 0.0107) and a positive attitude towards vaccination (AOR = 0.79, 95%CI: 0.73,0.86, P < 0.0001) were less likely to remain unvaccinated against COVID-19.
Conclusions
COVID-19 vaccination campaigns should be tailored for PLWH and incorporate stigma reduction interventions within healthcare settings.
Introduction
The human immunodeficiency virus (HIV) epidemic emerged over four decades ago and has remained a persistent global challenge ever since. In 2023, an estimated 39.9 million individuals worldwide were living with HIV (PLWH), with approximately 1.3 million new infections reported during the year—a 39% reduction since 2010. Acquired immunodeficiency syndrome (AIDS)-related illnesses accounted for approximately 630,000 deaths in 2023, representing a 51% decrease since 2010 and a 69% decline from the peak in 2004.1,2 Despite these notable advancements, Central Asia and Eastern Europe, including Kazakhstan, are among the few regions where HIV cases are rising (a 48% increase since 2010).3–5 There were ∼2000 new HIV cases in 2010 in Kazakhstan, according to UNAIDS, and in 2021, there were 3500 new cases, with an estimated total number of PLWH to be 35,000 in Kazakhstan. 3 The HIV epidemic is concentrated among high-risk populations, with prevalence of 8.3% among people who inject drugs, 1.3% among sex workers and 6.9% among men who have sex with men, 2 though some studies suggest under-reporting. 6 PLWH are considered vulnerable to outbreaks of infectious diseases, such as COVID-19.7,8
The COVID-19 pandemic had an adverse effect worldwide disproportionately impacting vulnerable populations, including PLWH. The COVID-19 pandemic has additionally caused disturbances in physical, emotional, and social well-being, and impeded the provision of optimal healthcare and access to HIV treatment. 9 During the COVID-19 pandemic in Kazakhstan, 1,504,370 cases of COVID-19 were registered with 19,072 deaths. 10 PLWH are a population that faces a heightened risk of being infected with and having severe COVID-19.7,9,11 Newly developed COVID-19 vaccines became the main intervention to control the transmission, prevent symptomatic illness, decrease illness severity, and reduce hospitalization and death from COVID-19 among PLWH.12–14 Despite the availability of effective vaccines, the vaccination uptake was low at the start of the vaccination process because of the high level of vaccine hesitancy among populations globally.15–17 New technologies and an accelerated timescale for vaccine development combined with multiple socio-economic factors contributed to the high level of vaccine hesitancy among people globally, especially in Central Asia 18 and in Kazakhstan.19–24 At the beginning of the vaccination campaign in Kazakhstan that started in February 2021 and carried out in stages, the only available vaccine was the vector vaccine, Sputnik V (Gamaleya Research Institute, Moscow, Russia).25–27 Other COVID-19 vaccines such as Sinopharm (BBIBP-CorV), 28 Sinovac (CoronaVac),29,30 the locally produced vaccine (QazCovid-in),31,32 Pfizer-BioNTech COVID-19 Vaccine COMIRNATY,33,34 and other vaccines became available much later during the pandemic.
Rapid introduction of the Sputnik V vaccine before the end of phase 3 of the trial, 25 controversy around transparency of data and procedures, 26 a politicized approach to the distribution of the vaccine, 27 and slow uptake of the vaccine in Russia may be the rationale for high vaccine hesitancy level in Kazakhstan. Global mistrust to Sputnik V 35 also could have worsened the uptake of COVID-19 vaccination of this specific product in Kazakhstan. COVID-19 vaccine hesitancy among PLWH is a public health concern, driven by various factors despite their heightened risk of severe outcomes. It is also important to note that at the start of the vaccination campaign, COVID-19 vaccines were available only at the primary healthcare facilities (policlinics) and then vaccination centers were opened at shopping malls. At the outset of the COVID-19 vaccination campaign, PLWH were confronted with conflicting messages regarding their eligibility for vaccination, as they were initially deemed ineligible for the Sputnik V vaccine. These initial challenges in accessing the COVID-19 vaccine may have increased a negative perception of vaccination against COVID-19, undermined trust in public health authorities and potentially exacerbated HIV-related stigma within the community. To tackle these challenges and to improve COVID-19 vaccine uptake among PLWH, vaccination sites become available at the network of AIDS centers that provide HIV treatment for PLWH in Kazakhstan.
Vaccine hesitancy and acceptance among general population and among PLWH depend on multiple socio-demographic factors such as age, gender, 36 education level, race/ethnicity, health behaviors, perceptions of vaccine safety and effectiveness, history of flu vaccination, substance use, level of anxiety,37–39 and perceived risk of infection and its severity.40–52 Specifically among PLWH, HIV stigma may serve as a barrier to receive healthcare services,53,54 including vaccination against COVID-19. 48 The fear of being identified as HIV-positive or having AIDS may deter individuals from seeking testing, accessing medical care and treatments, and disclosing their HIV status to their loved ones. 55 According to the existing literature, the factors influencing vaccine uptake are similar for general population and PLWH. However, among PLWH, engagement in healthcare services and achieving suppressed viral load are associated with a higher likelihood of receiving the COVID-19 vaccine,43,56 whereas elevated levels of HIV-related stigma48,57 are linked to a decreased likelihood of vaccination.
Due to PLWH's increased risk for adverse outcomes resulting from COVID-19 and unique factors that may be associated with vaccine uptake among this population, we conducted a study to evaluate determinants of COVID-19 vaccine uptake among PLWH in Kazakhstan.
Methods
This cross-sectional study took place in Almaty, the largest city in Kazakhstan, among PLWH. For this study, we used data from the cohort of PLWH who were randomly selected from the Almaty AIDS City Center medical record database and recruited for the study in 2019 (n = 230). 58 Based on systematic reviews, COVID-19 vaccination coverage among PLWH ranged from 44.0% to 90.1%. The sample size was calculated using Epi Info 7.2.6.0. At a 95% confidence level (with a 5% Type I error, P < 0.05), an absolute precision of 5%, and an expected prevalence of the outcome in the exposed group of 60%, the required sample size was at least 194. There were 230 participants who participated in the survey in 2019 and of those 196 agreed to participate between July 2022 and January 2023. There were no significant differences between those who participated in the survey (196) and those who didn’t (34) in terms of socio-demographic characteristics (age, sex, education, and employment) (Supplemental material, Table 4). Participants were eligible if they: (1) were 18 years old or older and (2) had been prescribed antiretroviral therapy (ART) for at least 6 months. PLWH were excluded if they (1) showed evidence of very severe psychiatric or cognitive impairment that would prevent them from understanding study procedures and providing informed consent or (2) were not fluent in Russian. Nurses at the AIDS Center contacted previous participants and invited them to participate in the survey about COVID-19 vaccination. Each participant signed a consent form and received ∼USD$10 compensation for completing a 90-min computerized self-assisted interview in Russian. Questions were translated into English for the manuscript publication.
The WHO EURO Vaccine Communications Working Group defines vaccine hesitancy as the delay in acceptance or refusal of vaccination despite the availability of vaccination services. 59 Our survey was informed by the WHO “3 Cs” model, which highlights three categories of factors that impact vaccination behavior: complacency, convenience, and confidence. In the “3 Cs” model, confidence is defined as trust in the effectiveness, and safety of vaccines and the system that delivers them. 59 Vaccination complacency is based on the perceived risks and severity of vaccine-preventable diseases, which can negatively influence vaccine uptake if the perceived probability and severity of the disease are low. Vaccination convenience is when the vaccination process and access are convenient in terms of physical availability and affordability.
Measures
Dependent Variable
COVID-19 Vaccine Non-Uptake
We used the following question to evaluate uptake: “Have you ever received a COVID-19 vaccine in your life to protect against coronavirus infection?”. We dichotomized response options into two categories: “received at least one dose” and “never received a dose” with the latter representing COVID-19 vaccine non-uptake.
Independent Variables
Socio-Demographic Variables
We collected socio-demographic variables, including age, sex, employment status, and educational level attained.
Substance use, Comorbid Conditions, and Psychosocial Characteristics
We collected information about lifetime injection drug use (yes/no) and hazardous alcohol drinking (assessed via the Alcohol Use Disorders Identification Test (AUDIT)) in the past year. The AUDIT consists of 10 questions related to alcohol use within the past year. A score of 8 or higher is considered hazardous drinking 60 . For our sample Cronbach alpha was α = 0.82.
History of Covid-19
Participants self-reported if they thought they ever had a COVID-19 infection (Yes/No).
Anxiety
The Generalized Anxiety Disorder (GAD-7) is a valid and efficient screening tool for assessing the presence and severity of anxiety in clinical practice and research. 61 GAD-7 categories are calculated by assigning scores of 0, 1, 2, and 3, to the response categories of “not at all,” “several days,” “more than half the days,” and “nearly every day,” respectively. The GAD-7 total score for the seven items ranges from 0 to 21. Scores of 0-4, 5-9, 10-14, and 15-21 represent ranges for no, mild, moderate, and severe anxiety, respectively. We used a cut point of ≥5 for at least mild symptom severity. The Cronbach's alpha in our sample was high α = 0.81.
Factors Specific to People Living With HIV
HIV Stigma
The HIV stigma scale by Reinius M et al consists of 12 items, using a 4-point Likert-type response, ranging from strongly disagree to strongly agree. 62 Scoring is calculated by summing the three items belonging to each of the four subscales, including enacted stigma with the personalized stigma dimension, anticipated stigma with public attitudes, disclosure concerns dimensions, and internalized stigma with negative self-image dimension (subscale range: 3-12). 62 A higher value of the score corresponds to higher level of HIV stigma. The Cronbach's alpha in our sample was α= 0.92.
Adherence to ART
Self-reported adherence was calculated using Wilson et al's 3-question scale 63 : “In the last 30 days, on how many days did you miss at least one dose of any of your HIV medicine?” (write in number of days, 0-30); “In the last 30 days, how well did you do at remembering to take all your prescribed HIV medication?” (excellent, very good, good, fair, poor, very poor); and “In the last 30 days, how often did you take your HIV medication as directed?” (always, almost always, usually, sometimes, rarely, never). In accordance with Wilson et al, each item was transformed to a 0-100 scale, then all items were summed, and an average score was calculated. We applied a cut-off point of 80%, classifying participants with an adherence score <80 as non-adherent and those with a score ≥80 as adherent. For this categorization approach, we followed the methodology described by O'Halloran Leach, E. et al 64 : “3 Cs” model factors and Complacency.
COVID-19-Related Risk Perception
Vaccination complacency is based on perceived risks and severity of vaccine-preventable diseases. Respondents’ perception of the likelihood of being infected (probability of COVID-19) and getting severe COVID-19 (probability of severe COVID-19) was assessed with 5-point Likert-type questions. To assess perceived severity of COVID-19, we used the following question: “In your opinion, how severe would contracting COVID-19 be for you?” (1 - “very mild” to 5 - “very severe”). 65 Higher scores indicated that respondents viewed COVID-19 infection as more severe.
Confidence
COVID-19 Vaccine Attitudes
We used the COVID-19 vaccine hesitancy adapted scale (11 items).66,67 Sample items included questions: “COVID-19 vaccines are important for my health,” “Getting a COVID-19 vaccine is important for the health of others in my community.”
Items were rated on a 5-point Likert scale from “Strongly disagree” to “Strongly agree” from 1 to 5 with a minimal possible value of 11 and a maximum possible value of 55. Higher scores indicated that the respondents held more positive attitudes toward COVID-19 vaccination. Cronbach alpha for our sample was α = 0.92.
Flu Vaccination
We consider flu vaccination uptake as a measure that is related to confidence.49–51
We asked if a participant has ever had an influenza (flu) vaccine with dichotomized response options: Yes and No/ Don't remember / I'm not sure.
Convenience
COVID-19 Vaccination Access
To evaluate the convenience dimension, we used a question about logistic difficulties to vaccination for PLWH: What, in your opinion, are barriers to vaccination against COVID-19 for PLWH? We categorized as having logistic vaccination access problems those participants who indicated at least one of the following barriers: vaccines are not available; vaccination location is far away.
The reporting of this study conforms to the Checklist of items that should be included in reports of cross-sectional study 68 (Supplemental Material: STROBE statement).
Data Analysis
We described the sample using means and standard deviations (SDs) and interquartile range for continuous variables and frequencies and percentages for categorical variables.
We first conducted a bivariate regression analysis to examine which factors were associated with COVID-19 vaccine uptake. Variables that showed significant association with the dependent variable at the level of P ≤ 0.1 were added to a multivariable regression model to evaluate associations between COVID-19 vaccine uptake and our selected variables. To assess collinearity, we examined variance inflation factors (VIFs) for all predictors in the regression model. None of the variables exceeded the commonly accepted threshold for multicollinearity (VIF > 10), indicating that collinearity was not a concern in our analysis. We used SAS 9.4 for all analyses.
Results
Sample Characteristics
Table 1 describes the socio-demographic characteristics of the study population along with the variables included for analysis. The mean age of participants was 44.5 (SD = 10.1, range =25-82) years old and less than half of the sample were women (n = 83, 42.35%). About half of the participants were employed full-time (n = 108, 55.10%). Half of the participants had a graduate or post-graduate degree (completed a bachelor's or higher degree) (n = 105, 53.57%). One-fifth of the participants (n = 40, 20.41%) injected illicit drugs at some point in their life. Hazardous alcohol drinking (score >=8) reported about one-tenth of participants (n = 23, 11.73%). Thirty-seven participants (18.8%) reported a history of COVID-19 infection.
Socio-Demographic Characteristics of Participants by COVID-19 Vaccination Status.

Abbreviations: SD, standard deviation; AUDIT, alcohol use disorders identification test; IQR, interquartile range; GAD-7 generalized anxiety disorder-7; ART, antiretroviral therapy; HIV, human immunodeficiency virus.
Based on T-test; bBased on chi-squared test; cBased on Fisher's test.
In terms of vaccine uptake, less than half of participants received at least one dose of COVID-19 vaccine (n = 87, 44.39%) (Figure 1). Since Sputnik V was the only available vaccine at the beginning of the vaccination program in the country, the majority of participants received Sputnik V vaccination. Somewhat later other vaccines became available including Sinopharm (BBIBP-CorV), 28 Sinovac (CoronaVac),29,30 the locally produced vaccine (QazCovid-in),31,32 and Pfizer-BioNTech COVID-19 Vaccine COMIRNATY33,34 (Figure 2).
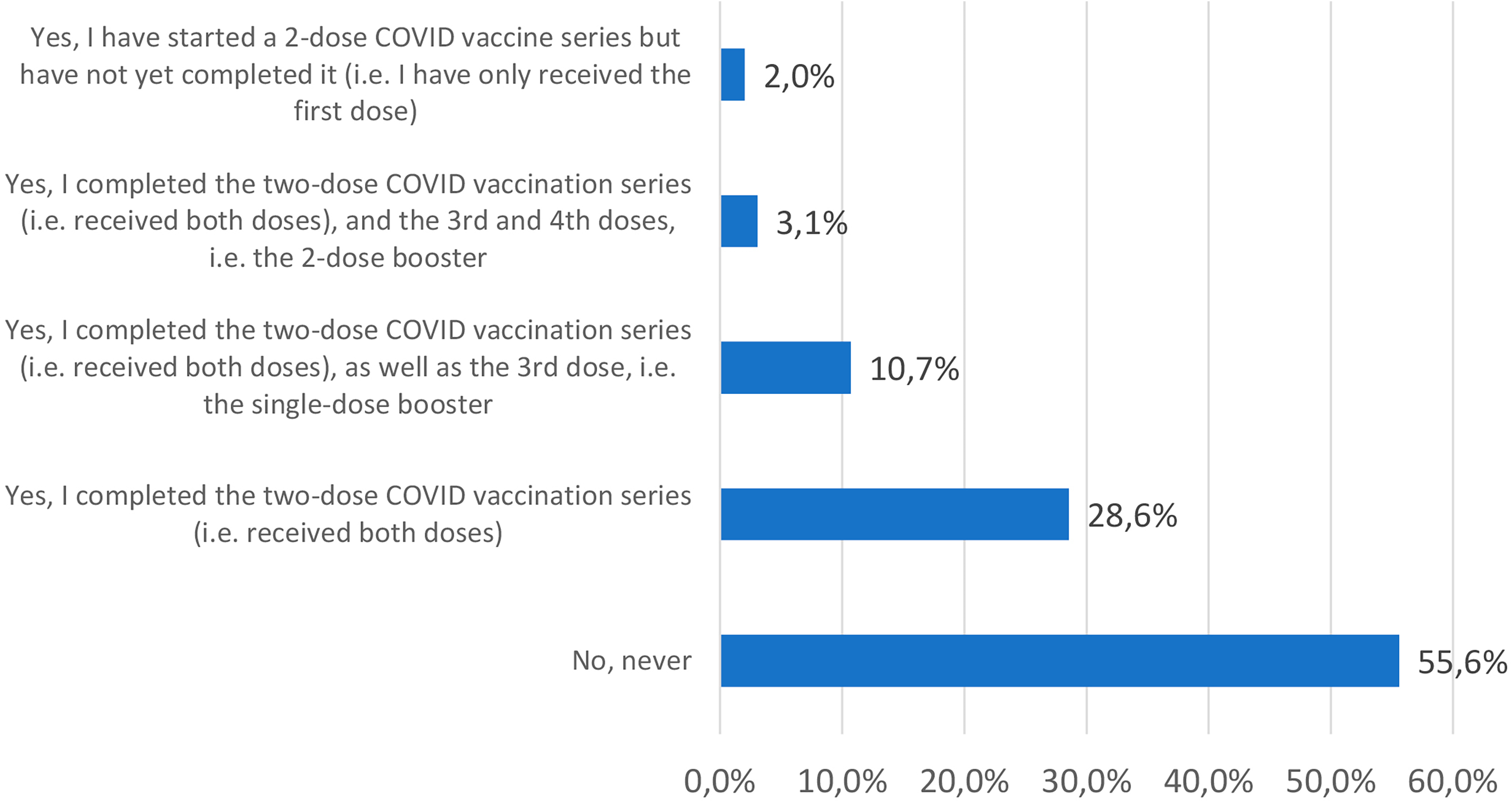
Vaccine uptake among PLWH.

Types of vaccine PLWH received.
Bivariate Analyses
In the bivariate regression analysis (Table 2), we found that for each 1-year increase in age, the odds of COVID-19 non-uptake increased by 3% (OR = 1.03, 95%CI (1.00, 1.06), P = 0.0393) and that older participants had slightly higher odds of not being vaccinated against COVID-19. Those who had a lower level of education (up to high school) compared to those who had at least 2-3 years of college, had higher odds of the COVID-19 vaccine non-uptake (OR = 3.16, 95%CI (1.75, 5.72), P = 0.0001).
Bivariate Association of Multilevel Variables with COVID-19 Vaccine Non-Uptake.

Abbreviations: CI, confidence interval; OR, odds ratio; GAD-7, generalized anxiety disorder-7; HIV, human immunodeficiency virus; ART, antiretroviral therapy.
In comparison with those who were full-time employed, those who work part-time, self-employed, homemakers, retired, and unemployed had higher odds of COVID-19 vaccine non-uptake (OR = 3.10, 95%CI (1.71, 5.61), P = 0.0002).
The odds of COVID-19 vaccine non-uptake were lower among those who had symptoms of at least mild anxiety (GAD-7 score ≥5) in comparison with those who hadn’t (OR = 0.23, 95%CI (0.09, 0.57), P = 0.0016).
Those who had higher HIV stigma score were significantly more likely to remain unvaccinated against COVID-19, with each one-point increase in the stigma score associated with an 11% increase in the odds of COVID-19 vaccine non-uptake(OR = 1.11, 95%CI (1.06, 1.16), P < .0001).
Participants with positive COVID-19 vaccine attitude toward the COVID-19 vaccine (higher attitude scores) were significantly less likely to remain unvaccinated. Specifically, each one-point increase in the positive attitude score was associated with a 21% decrease in the odds of COVID-19 vaccine non-uptake (OR = 0.79, 95%CI (0.74, 0.85), P < .0001). Those participants who had never received flu vaccination also had higher odds of COVID-19 vaccine non-uptake (OR = 24.94, 95%CI (7.33, 84.83), P < .0001 in comparison with those participants who had ever received flu vaccination (Table 2).
Multivariable Analysis
In the multivariable regression analysis (Table 3), we found that participants with lower levels of education (up to high school) compared to those who had at least 2-3 years of college had higher odds of COVID-19 vaccine non-uptake (AOR = 2.53, 95%CI: 1.04, 6.17, P = 0.0412). We found that having at least mild anxiety symptoms (GAD-7 score ≥ 5) was associated with a lower probability of COVID-19 vaccine non-uptake (AOR = 0.15, 95%CI: 0.03, 0.64, P = 0.0107). Participants with higher HIV stigma scores were significantly more likely to remain unvaccinated against COVID-19. Each one-point increase in the stigma score was associated with an 8% increase in the odds of COVID-19 vaccine non-uptake (AOR = 1.08, 95% CI: 1.02-1.16, P = 0.017). Regarding the COVID-19 vaccine confidence scale score, we found that respondents with a positive attitude (higher attitude scores) had lower chances of Covid-19 vaccine non-uptake. Specifically, each one-point increase in the positive attitude score was associated with a 21% decrease in the odds of COVID-19 vaccine non-uptake (AOR = 0.79, 95%CI: 0.73, 0.86, P < .0001). Participants who have never received a flu vaccine had higher odds of COVID-19 vaccine non-uptake (AOR = 15.64, 95%CI: 3.66, 66.89, P = 0.0002) if compare with those who have ever received flu vaccine (Table 3).
Multivariate Association of Multilevel Variables with COVID-19 Vaccine Non-Uptake.

CI, confidence interval; AOR, adjusted odds ratio; GAD-7, generalized anxiety disorder-7; HIV, human immunodeficiency virus.
Discussion
This cross-sectional study investigates the determinants of COVID-19 vaccine uptake among PLWH in Kazakhstan, a population at heightened risk for severe COVID-19 outcomes. Our findings reveal notably low vaccination rates in this group, with less than half having received the COVID-19 vaccine and only one-fifth ever vaccinated against influenza. Key factors associated with vaccine uptake included educational level, mental health, history of vaccination against influenza, vaccine confidence, and HIV stigma. Participants with lower education levels were significantly less likely to receive the COVID-19 vaccine, while those with at least mild anxiety symptoms and a positive attitude toward COVID-19 vaccination were more likely to be vaccinated. Conversely, higher HIV stigma scores were associated with lower vaccination rates. Notably, a history of influenza vaccination was positively correlated with COVID-19 vaccine uptake. These findings underscore the need for targeted interventions to address educational, psychological, and systemic barriers to vaccination in this vulnerable population.
Vaccine hesitancy is a widespread phenomenon that is considered by the WHO as one of the top 10 global threats. 69 Multiple multilevel factors hindered the expansion of vaccination against COVID among the general population and especially among PLWH.70,71 The first available COVID-19 vaccine in Kazakhstan was vector vaccine Sputnik V. However, the rapid development and introduction of Sputnik V before the completion of Phase 3 trials contributed to vaccine hesitancy in Kazakhstan.25–27
We have found that the vaccination rate among our cohort of PLWH is low for two important infections: for COVID-19, with less than half of this population who have received the COVID-19 vaccine; and even lower for flu with only one-fifth of this vulnerable population who have ever received the flu vaccine. According to official data by January 2023, in Kazakhstan 81, 1% of the eligible population for vaccination received the COVID-19 vaccine and 80.1% in Almaty, 72 compared to 44.39% of PLWH in our sample. This reflects a high level of COVID-19 vaccine hesitancy among PLWH in Kazakhstan.
Our analysis revealed that participants with a lower level of education exhibited a significantly lower likelihood of receiving at least one dose of the COVID-19 vaccine. This aligns with the results of several systematic reviews, which have consistently highlighted lower education levels as one of the key determinants of COVID-19 vaccine hesitancy.52,73,74 This could be attributed to the fact that individuals with higher education levels often have greater access to vaccine-related information, enabling them to comprehend the benefits and safety aspects of the COVID-19 vaccine.52,73,74
In our sample, one-tenth of participants had at least mild anxiety symptoms and these participants had higher odds of getting the vaccine against COVID-19. Results from other studies have not found a consistent direction of association of symptoms of anxiety with COVID-19 vaccine hesitancy and uptake.37,38,75 In a 23-country study, vaccine hesitancy was significantly positively correlated with the experience of anxiety in South Korea and the US, but negatively correlated with the experience of anxiety in Canada and Peru. 37 There have been a limited number of studies investigating the relationship between mental health and vaccine hesitancy. The impact of anxiety on vaccine hesitancy varies significantly, with differing associations observed across the 23 countries studied. 37 Future research should explore the role of cultural factors in shaping the relationship between mental health and vaccine hesitancy.
When measuring vaccine confidence, we found that participants with a positive attitude to the COVID-19 vaccine were more likely to be vaccinated against COVID-19. These findings are consistent with the findings of other studies that found evidence of the association of vaccine uptake with a more positive attitude to vaccine, including vaccine efficacy, fewer concerns about vaccine safety and side effects, and trust in the system providing vaccination.52,76–79
Prior history of flu vaccination has emerged as a strongest predictor of COVID-19 vaccine uptake. These results are consistent with results of other studies.52,80 This strong association suggests that prior vaccination experiences may positively influence individuals’ willingness to engage with new vaccines, such as those developed for COVID-19. The promotion of flu vaccines has been shown to impact the uptake of COVID-19 vaccines, highlighting the interconnectedness of vaccination behaviors among different vaccines.80,81
Another important factor that impacts behavior of PLWH is HIV stigma. Participants of the study who had higher HIV stigma score had a lower probability of receiving the COVID-19 vaccine. Our findings are consistent with the results of other studies, including in Georgia, a country that as a post-Soviet country is culturally similar to Kazakhstan.48,82 In the study among PLWH by Zheng et al, one of the two top reasons not to initiate COVID-19 vaccination was disclosure of HIV status. 83 HIV stigma proved to be a barrier for PLWH to receive health care services53,54 because of the fear of being identified as HIV-positive and disclosure of their HIV status to their loved ones. 55
There are several limitations of the study. The cross-sectional study design precludes the establishment of a temporal relationship between dependent and independent variables. Given that vaccine confidence exhibits dynamic characteristics, it is important to note that our study was conducted during a later phase of the pandemic, after extensive reassurances 48 from the literature regarding the safety of the vaccine. Another limitation of this study is that we surveyed participants who was on ART treatment at least 6 months at the time of recruitment and might have better access to health care services and less HIV stigma.
However, even though the sample size was not large, participants were randomly enrolled from the registry of Almaty City AIDS center, the nation's largest city. We employed a forward selection strategy to build the multivariable model, including only variables that were significant in the bivariate analyses. This approach can overlook potentially important variables that are not significant in bivariate analyses but could contribute to the model when considered in combination with other predictors. To mitigate these concerns, we carefully selected the initial pool of variables based on prior literature and theoretical relevance, ensuring that important variables were not omitted.
Conclusions
In our study sample of PLWH, we identified factors associated with COVID-19 vaccine uptake. Less than half of our study population received the COVID-19 vaccine which was almost twice lower than among the general population in Kazakhstan. We observed that individuals with lower levels of education and higher levels of HIV stigma exhibited a decreased likelihood of COVID-19 vaccine uptake. Those experiencing mild symptoms of anxiety, possessing higher levels of vaccine confidence, and having a history of flu vaccination were more likely to get the COVID-19 vaccine.
Targeted educational campaigns should be specifically designed for PLWH and address their unique concerns and questions regarding COVID-19 vaccine safety and efficacy. That campaign should prioritize outreach to individuals who have never received a flu vaccination, emphasizing the benefits of vaccines in general and addressing misconceptions about the COVID-19 vaccine, ensuring it is easy to understand for individuals with limited education. Strategies aimed at increasing flu vaccination rates could concurrently boost COVID-19 vaccination efforts. The development of tailored educational initiatives addressing the specific concerns of PLWH regarding COVID-19 vaccine safety and efficacy can significantly enhance vaccine uptake. Incorporating visual aids, infographics, and multimedia content can effectively simplify complex information, making it more accessible and engaging for diverse audiences.
It is important to implement stigma reduction interventions within HIV care facilities and other healthcare facilities providing vaccination for healthcare providers to address and reduce HIV stigma, to create a welcoming and inclusive environment to improve vaccine uptake among PLWH. Another effective strategy for building trust within the PLWH community is to encourage peer support programs, where vaccinated individuals share their personal experiences.
These measures will empower PLWH to make informed decisions about the COVID-19 vaccine and improve access to it ultimately contributing to better health outcomes within this community.
Supplemental Material
sj-xlsx-1-jia-10.1177_23259582251328861 - Supplemental material for Determinants of COVID-19 Vaccine Uptake Among People Living with Human Immunodeficiency Virus
Supplemental material, sj-xlsx-1-jia-10.1177_23259582251328861 for Determinants of COVID-19 Vaccine Uptake Among People Living with Human Immunodeficiency Virus by Gaukhar Mergenova, Alissa Davis, Susan L Rosenthal, Assel Terlikbayeva, Sholpan Primbetova, Meruyert Darisheva, Assel Bukharbayeva and Alfiya Y Denebayeva, Jack DeHovitz in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251328861 - Supplemental material for Determinants of COVID-19 Vaccine Uptake Among People Living with Human Immunodeficiency Virus
Supplemental material, sj-docx-2-jia-10.1177_23259582251328861 for Determinants of COVID-19 Vaccine Uptake Among People Living with Human Immunodeficiency Virus by Gaukhar Mergenova, Alissa Davis, Susan L Rosenthal, Assel Terlikbayeva, Sholpan Primbetova, Meruyert Darisheva, Assel Bukharbayeva and Alfiya Y Denebayeva, Jack DeHovitz in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgements
This study was supported by the Fogarty International Center and the National Institute of Drug Abuse under Award Number D43 TW010046.PIs: Drs. Jack DeHovitz & Zhamilya Nugmanova. We thank the participants, research assistants, nurses, psychologist and administrative staff of Almaty City AIDS center.
Ethical Considerations
The study was approved by the Local Ethics Committee of SD Asfendiyarov Kazakh National Medical University (IRB00011496), Protocol No. 5 [128], April 27, 2022. Written Informed consent has been obtained from the involved participants prior to the survey.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Fogarty International Center and the National Institute of Drug Abuse under Award Number D43 TW010046.PIs: Drs. Jack DeHovitz & Zhamilya Nugmanova.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.