
Abstract
Background
Option B+ aims to prevent mother-to-child transmission of HIV by providing lifelong antiretroviral therapy (ART) to pregnant and breastfeeding women living with HIV (PBWHIV). Identifying and reengaging PBWHIV who disengage or fail to initiate ART is essential for the success of Option B+. However, the process is often suboptimal, leading to challenges such as misclassification of patients as lost to follow-up. Healthcare workers (HCWs) are pivotal for monitoring engagement, but little is known about their monitoring practices. This study aimed to explore how HCWs monitor women's engagement in Option B+ services.
Methods
A qualitative study was conducted in five high-volume health facilities in Lilongwe, Malawi. Thirty HCWs responsible for monitoring women in Option B+ were purposively selected as key informants. Semistructured interviews were conducted between March and June 2021. Thematic analysis employing deductive and inductive coding methods was utilized. The Consolidated Framework for Implementation Research was used to map gaps, strategies, barriers, and facilitators of monitoring.
Results
Monitoring was described as tracking a PBWHIV from HIV diagnosis to initiation of ART to subsequent ART visits for up to 2 years postpartum. The gaps included timing variations in tracing. No procedures to follow up formal transfer-outs or management of silent transfers during emergency ART refills were identified. Strategies identified included interfacility collaboration, record review, tracing, escorting women during initial visits, and self-reports. Technological innovations, such as WhatsApp groups, were highlighted as game changers in interfacility collaboration when tracking women's movements. Barriers included resource constraints (human and operational), poor work attitudes, and challenges faced by women (partner support, stigma, and HCW rapport). The facilitators included implementing partner support, leadership, and strategies such as education and tracing.
Conclusion
Addressing resource constraints, women's relationship dynamics for self-management, HCWs’ attitudes, and standardizing tracing protocols are crucial for effective monitoring. Leveraging instant messaging for clinic coordination may enhance tracing. Further research and interventions should target identified gaps to promote effective monitoring in similar settings.
Plain Language Summary
This study investigates how HCWs monitor women's engagement in Option B+, which aims to prevent mothers from transmitting HIV to their children by providing lifelong ART during pregnancy and breastfeeding. Through interviews with 30 HCWs in Lilongwe, Malawi, the study reveals strategies such as collaboration, record review, tracing, and WhatsApp communication. Challenges include timing variations in tracing, resource constraints, negative attitudes, and difficulties faced by women. To enhance monitoring, addressing resource constraints, supporting women, improving HCWs’ attitudes, and standardizing tracing protocols are crucial. Utilizing instant messaging for communication could improve tracing efforts. The study underscores the importance of addressing these issues to improve monitoring effectiveness and calls for further research and interventions to bridge identified gaps in similar settings.
Introduction
Option B+ is a program aimed at preventing mother-to-child transmission of HIV by providing pregnant and breastfeeding women living with HIV (PBWHIV) with lifelong antiretroviral therapy (ART). 1 This initiative has significantly advanced global efforts to eliminate pediatric HIV infections, leading to a 62% decline in new HIV infections among children, from 300,000 in 2010 to 120,000 in 2023.2,3 However, delays in starting or sustaining engagement, failures to join or reengage, and dropping out of Option B+ all hinder its success and increase the risk of HIV transmission to children. 4 Therefore, monitoring women's engagement with Option B+ is imperative to address these challenges and enhance the program's impact.
Optimal monitoring involves prompt identification, reaching out, and reengaging those who have disengaged or lapsed in engagement, including those who move between or switch clinics.5,6 Importantly, monitoring should incorporate a mechanism for shared decision-making between healthcare workers (HCWs) and women in Option B+, fostering accurate information exchange regarding their contacts, movements, and engagement decisions.7,8 The Malawi Clinical Management of HIV in Children and Adults guidelines highlight monitoring as an important strategy for increasing retention in care.9,10 These guidelines provide a framework for our study by outlining recommended practices for tracking and supporting women in Option B+. Malawi has made substantial efforts to optimize monitoring that corresponds to programmatic shifts in the prevention of mother-to-child transmission of HIV (PMTCT). 11 These efforts span the implementation of electronic data systems, task shifting, simplified paper-based tools, and defaulter tracing, all of which support the evolving needs of PMTCT.9,12–14
Despite these efforts, monitoring of women in Option B+ remains suboptimal, as studies indicate that patients are frequently misclassified as lost to follow-up (LTFU) while in care at another clinic or have died.15–19 Additionally, a study from the United States of America suggested that only 53% of HIV care providers engage in systematic monitoring in facilities, and this percentage might be even lower in low- and middle-income countries.20,21 Therefore, understanding monitoring from the perspectives of frontline HCWs is crucial, as it may offer insights for improving monitoring practices of women's engagement in HIV care. This study aimed to explore the processes, barriers, and facilitators involved in monitoring women's engagement in Option B+ among HCWs in Lilongwe, Malawi.
Methods
Design and Setting
This qualitative study was conducted in 5 high-volume health facilities in Lilongwe, Malawi, serving a combined catchment area of approximately 700,000 people. The facilities serve over 50,000 pregnant women annually, including more than 1500 women living with HIV.22–24 These sites were selected due to their high patient volume, documented challenges with LTFU, and suboptimal monitoring.25,26 The facilities provide PMTCT services that are delivered at multiple service points, including antenatal clinics (ANC), maternity clinics, HIV testing services (HTS), ART clinics, and under-5 clinics (U5C). The Health Management Information System (HMIS) office of the Malawi Ministry of Health (MoH) supports data collection and management for Option B+.
The study is grounded on a phenomenological research paradigm to deeply explore and interpret HCWs’ lived experiences and perspectives on monitoring women's engagement in Option B+. 27 This approach aims to reveal the nuanced barriers and facilitators in monitoring engagement in Option B+ services.
Routine Process for Monitoring Engagement in Option B+
The standard process for monitoring women's engagement in Option B+ begins when a pregnant or breastfeeding woman is diagnosed with HIV and continues until the child reaches 2 years of age. This process involves 4 key aspects. First, a documentation workflow, which highlights the system for collecting information for determining engagement status through the use of several data collection tools. These include the ART Mastercard for the mother and the infant exposed to HIV “pink” card, which serves as the primary patient file. The HIV Care Clinic Register logs HIV-exposed children, while the ART Register or Electronic Medical Records System (EMRS) tracks clients living with HIV. The woman's health passport, a booklet maintained by the woman at all clinic visits, records her ART number and the next appointment date.
Second, the linkage process focuses on tracking newly diagnosed pregnant or breastfeeding women who initiate ART on the same day. If a woman is not ready to start ART, a “reflection period” of up to 14 days is provided. Third, subsequent visits attendance is tracked throughout participation in the program. Tracing begins 2 weeks after a missed appointment. Visits are classified as “defaulter” if ART has run out for 2 or more months, or exposed children, 2 months after the next appointment date given at the last visit. Women are considered LTFU if overdue and there is no indication that they have stopped ART, died, or transferred to another facility. Lastly transfers, official transfers include providing the mother/child with their Mastercard and pink card for presentation to a new clinic. The receiving clinic will record the transfer in their record. Unofficial transfers may be identified by review of the health passport to detect previous ART use. Verbal consent is obtained, and locator information is collected from PBWHIV for active follow-up on late appointments.
Population and Sampling
A total of 30 HCWs were purposefully recruited as study participants. These included key personnel or point persons working in ANC, maternity, HTS, ART clinics, HMIS, and U5C clinics on Option B+. The HCW cadres included nurses, data personnel, health surveillance assistants (HSAs)/counselors, and clinicians. In this paper, the HMIS personnel will be referred to as data personnel. The sample size was determined using existing recommendations of 25–30 participants minimum to reach saturation for interview studies. 28
Data Collection
Prior to data collection, potential participants were sensitized about the study. Data were collected between March and June 2021 through face-to-face interviews that took 30 min to 1 h. A female-trained bilingual research assistant (RA) with a diploma and more than 8 years of qualitative experience, along with the first author (male), a data manager with a Master's degree conducted interviews using a semistructure in-depth interview guide. The participants did not know the interviewers and they only knew them as researchers from UNC Project Malawi. The guides were pilot-tested to assess language, concept, and content understanding of the questions and revised accordingly before using them in the study. The study participants described how the process of monitoring women's engagement was conducted and explained the gaps, strategies, barriers, and facilitators associated with monitoring in Option B+. Interviews were audiotaped with participant consent, conducted in the participants’ preferred language (Chichewa or English), and scheduled based on their availability. No third person was present during the interviews. A 1-step approach was used for translation and transcription by the RA, with the first author reviewing all transcripts for accuracy. This method was chosen for its practicality and cost-effectiveness, given that both the RA and first author were bilingual. Although this approach may introduce some inaccuracies, it was deemed appropriate for this study. The value of forward and back-translation for future research is acknowledged. The transcripts were not sent for comment to the participants. No field notes were made during the interview. No interviews were repeated, and none had to be canceled.
Theoretical Framework
The study used the Consolidated Framework for Implementation Research (CFIR) to map relevant factors affecting HCWs to monitor women's engagement in Option B+. CFIR is a meta-theory framework that systematically identifies factors that may emerge in various multilevel contexts that influence implementation.29,30 The CFIR has 39 constructs related to implementation across 5 domains: characteristics of the intervention, outer setting, inner setting, characteristics of the individuals involved, and the process of implementation. 31 The framework was applied to map identified barriers and facilitators into relevant CFIR domains and constructs, enabling a structured analysis of implementation challenges and opportunities for monitoring engagement in Option B+.
Data Analysis
The transcripts were analyzed using thematic analysis, 32 employing deductive and inductive approaches, with NVivo and Microsoft Excel software aiding the process. Initially, the data were familiarized through repeated reading of transcripts. The codebook was then developed and refined through deductive coding based on the interview guide's primary questions, followed by inductive coding to identify emerging themes. These steps were done in NVivo. Identified barriers and facilitators for monitoring were mapped deductively into relevant CFIR domains and constructs using Microsoft Excel. Data coding and interpretation were conducted independently by the first author and independent analyst (male)—a clinician with a master's degree who was not involved in the data collection or cleaning. If there were any disagreements on the data coding and interpretation of themes, the two researchers would go through the transcripts and discuss the differences until a consensus was reached. A senior qualitative expert (female)—director of nursing and qualitative unit with a doctoral degree, reviewed and validated the codes, themes, and interpretation.
Ethical Approval and Informed Consent
This study was approved by the National Health Research Science Committee (approval no. 18/08/2137). All participants provided written informed consent prior to enrolment in the study. To maintain privacy and confidentiality, the consenting process and interviews were performed in a private place chosen by the participant within their respective facility.
Results
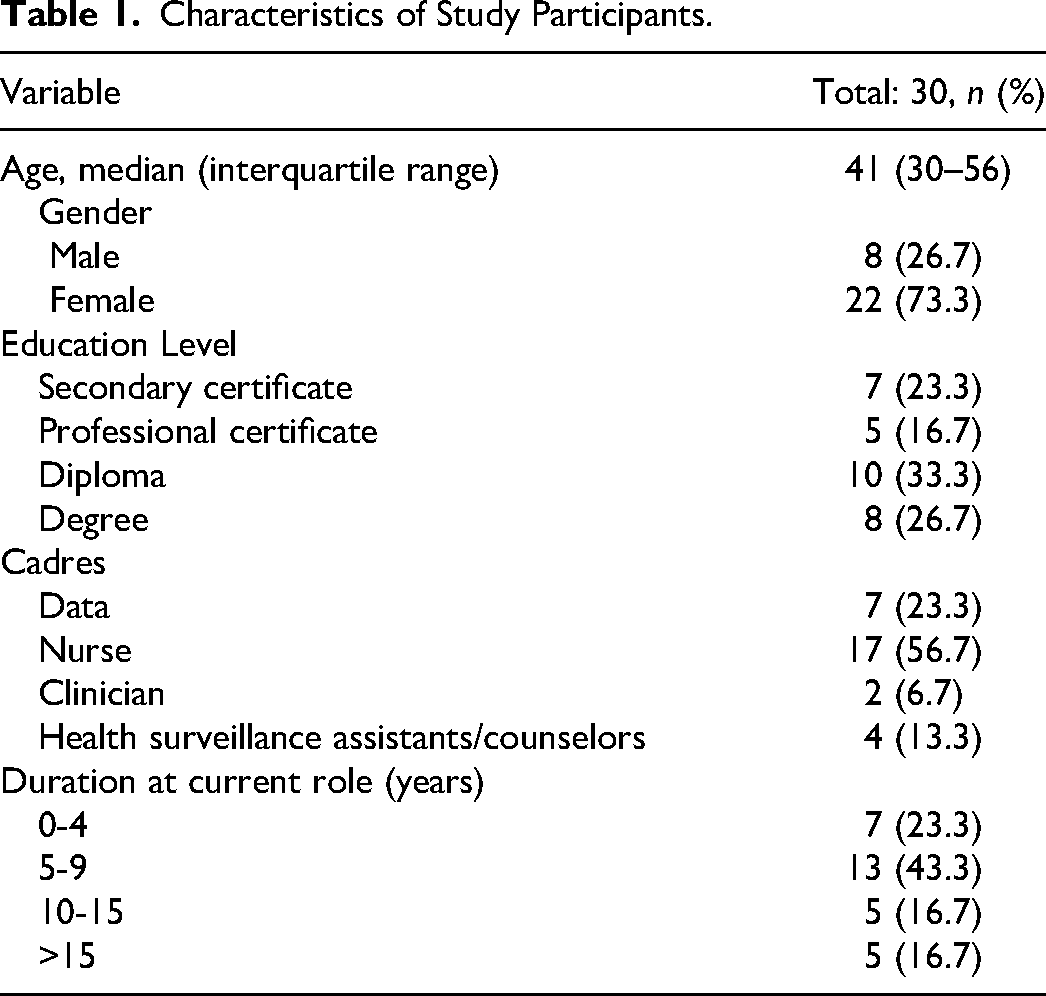
We recruited 30 key informants with a median age of 41 years. Three-quarters had 5 or more years of experience, and over half were nurses, who are leaders of PMTCT implementation (Table 1).
Characteristics of Study Participants.
Current Procedures for Monitoring Engagement
HCWs described the monitoring process in ways that were similar to the standard approach, such as the prescribed duration for tracking engagement in Option B+ and the reported tools used for tracking the engagement status of women (though some mentioned other tools being piloted by partner organizations such as the tracing register). For instance, one nurse explained; We identify them through the health passport of the mother when a woman has come with a child. Health passports contain a sticker which shows that the woman is on ART, the last visit date, as well as date of the next visit… we use registers, these are available in all departments providing PMTCT services like the antenatal clinic, labor ward and from where the child gets care during breastfeeding, until when two years…we also use a woman's Mastercard and a child's pink card. (Nurse, 40 years, Site 2) If a person transfers without any procedures but explains they were taking medication. We test them to confirm their status. She begins like a new client then we ask them for a locator to ensure that they are properly followed-up. (HSA/Counsellor, 54 years, Site 4)
Similarly, the reported management of transfers, especially those formally transferring away from or into the facility, was consistent with the standard approach. A nurse explained: For formal transfers, its simple. For transfer-out, we have a form where we document everything, including information about the child. The child has a pink card, which we give to the woman to take with her wherever she is going… When transfer-ins come, they bring the child’ pink card, and we register the child according to the cohort. The mother also presents her Mastercard, and we then register. (Nurse, 46 years, Site 5)
Gaps in the Monitoring Process
Defaulters are in two groups, there is this one for PEPFAR which we like using with our partners, they state that defaulter is 28 days but there is the other one I don’t know if it's the Ministry of Health its two months. So, what happens we review our data almost every day to check how many have defaulted, so we take the names of those women and share them with expert clients or patient supporters for tracing. (Nurse, 49 years, Site 5)
When we transfer them out, we are done with them…because we do not have a system to follow them up…We don’t know if they have arrived or not. It is the same as those facilities that do not provide ART. They refer the patients to health facilities where ART is provided but they are not sure if they really go or not because they do not follow them. (Nurse, 34 years, Site 1)
Those who come without proper procedures, we have procedures that we follow. For example, if someone comes and say “I am HIV positive and on ART but I do not have a transfer,” we test them to confirm they are HIV positive and we give them emergency supply but we emphasize to them that they need to go and get their transfer. Some are able to go and get their transfer but there are others who say “I cannot manage to go and get my transfer. Enrol me as a new patient.” And it happens. (HSA/Counsellor, 43 years, Site 5)
Strategies for Monitoring Client Engagement
Participants described various strategies for monitoring women's engagement in Option B+. This primarily included reviewing records during clinic visits and retrospectively, sometimes cross-referencing daily reports from different service points. Phone and physical tracing frequently revealed self-transfers or deaths. Usually, it is [silent transfer identification] through tracing by community health workers, when they go for tracing in the communities, they receive reports that this individual has transferred somewhere. Sometimes, if you call them [women] and they happen to answer, they say I am no longer there, I transferred but I did not come there to report that I am now at this other facility. (Nurse, 46 years, Site 4)
If a woman came without any document from where they were, we go on that WhatsApp group, and write on that group transfer out this number from your facility, then we ask let's say she was at Chikwawa, then we write that Chikwawa coordinator or Chikwawa data clerk or what, can you inbox me because we cannot put the name on that group since we are many there? (Nurse, 49 years, Site 5)
Escorting women through each service point and prioritizing them during clinic visits were also frequently mentioned but in the context of initial or linkage visits, unlike subsequent visits.
When a woman is found HIV-positive from the HTS, we escort them to the appropriate room and hand over them for counselling. After receiving counselling, they also escorted them to the ART clinic for ART counselling. At ART, they document the women and enter them into the system. (HSA/Counsellor, 43 years, Site 5)
Emergency ART refill is a strategy that ensures treatment continuity when women temporarily move between clinics. Participants reported that some silent transfers were identified during emergency pill access. One participant felt that this strategy prompted women to potentially mask themselves as new initiators after the refill period. However, participants mentioned that most identified silent transfers end up being registered as new clients.
For those people who come to the facility and are not able to produce the transfers, we enroll them as new positives and start giving them ART … we monitor her every month for six months. (Nurse, 30 years, Site 2)
Other strategies mentioned were women's self-reports, their demonstrated PMTCT knowledge during clinic interactions for defaulters or self-transfers, and their memory recall of familiar faces.
Barriers and Facilitators of Monitoring Engagement
Factors affecting the process of monitoring women's engagement were found to fall within 3 domains and 8 constructs of the CFIR framework.
Inner Setting
… the workload it's just overwhelming, during morning handover, it's been discovered that our facility is able to see approximately 200 pregnant women every day, from Monday to Friday, so you can imagine 200 against 2 people sometimes if you are lucky 3 people … so it's easier to lose someone with such kind of numbers, yah. (Nurse, 35 years, Site 4)
To say the truth, we left that to partners, but after they go, it is when we as government; we will be seen not working on it… otherwise, we call it a partner thing knowing that the partner is implementing it for the government. (Nurse, 53 years, Site 3)
The leadership has challenges providing support, maybe because there is no money, but in terms of moral support, they do provide. (Nurse, 49 years, Site 5)
We have no cadre for field tracing, but we take advantage of the HSAs [Health Surveillance Assistants] to do the tracing in the communities, but this is occasional as you know that you cannot delegate HSAs without a refreshment… [Laughter]… We depend on the expert clients. (Data Personnel, 35 years, Site 3)
We have different organizations that we work with. These organizations help us a lot in following up with the women. From the MOH [ministry of health], we have HSAs [Health surveillance assistant] who help to physically trace the women. However, the partner organizations help a lot with phone tracing, and they also provide expert clients [peer mentor mothers that support women in Option B+] to perform physical tracing. (Nurse, 41 years, Site 1)
Outer Setting
Sometimes these women when they are coming, they come with their names changed … so you notice them through face recall, then you would say are you not so and so? What happened for you to change your name? Ah no, I was afraid that you would shout at me because it has been some months since I left coming to collect my medication. (HSA/Counsellor, 54 years, Site 4)
Participants also reported strategies for sustained engagement in Option B+, including maintaining confidentiality, patient prioritization, and integrating services for privacy and reduced clinic time. Outreach programs and emergency ART refills help reduce the burden of clinic visits. Community involvement, peer support, tracing, phone reminders, and a patient-centered approach provide social support. Collaboration with women to gain partner support through clinic invitations, retesting, and home visits was found to be useful. Last, patient education and counseling were frequently mentioned as fundamental, as knowledgeable clients are more likely to comply with program demands. Mostly it is through counselling and motivation, and if the woman received good counselling, she is motivated to come to the clinic for ART. (Nurse, 30 years, Site 2)
Others, when they are told to bring a transfer after getting the emergency supply twice, they just change their health passport. Therefore, they come as new initiates, and you document them as such, but somewhere they also appear that they are on ART which you cannot know. (Clinician, 37 years, Site 1)
Characteristics of an Individual
This process is very important because for us to work better, it means PMTCT women should be followed up, and if the child born from this woman is HIV negative, it means we have achieved. Sure, for me as a health worker because one of my tasks is to ensure that we have a healthy community. (Nurse, 33 years, Site 2)
Challenges that we may face as a facility is that not every staff is following or monitoring these women diligently others are just lazy to do the follow ups that's the challenges that we face we talk about all the time, but it's just a personal interest or personal initiative for one to follow up the women. (Nurse, 35 years, Site 4)
We cannot do well in the PMTCT program as a single department because the women pass through different departments, such as ANC, the labor ward, and the postnatal ward, then to their communities. Therefore, the biggest gap that is there is the knowledge gap on health providers in other departments. (Nurse, 41 years, Site 1)
Only one participant highlighted that discrepancies in documentation may contribute to misclassification of an outcome.
Discussion
Through the lens of frontline HCWs in high-volume facilities in Lilongwe, Malawi, our study revealed that gaps in the monitoring process encompassed inadequate follow-up procedures for formal transfers, timing variation in tracing, and lapses in patient identifier management. Strategies for monitoring included interfacility collaboration, escorting women during clinic visits, access to emergency ART refills, and record reviews. Barriers or facilitators to effective monitoring were mapped to 3 CFIR domains: Inner Setting (resource availability, partner organization support, and leadership), Characteristics of Individuals (HCWs’ work attitudes), and Outer Setting (women's knowledge and experiences).
Our study revealed that the monitoring process lacked a tracking procedure for formal transfer-out, whereby HCWs do not confirm whether the client has successfully switched clinics. This finding aligns with previous research showing that even with official transfers, the reengagement of clients is often delayed33–35 Having mechanisms to remind HCWs to follow-up transfer-out within prespecified periods may avoid delays or LTFU. One way would be to embed an algorithm within the EMRS to send text reminders for HCWs and to have a dashboard that lists all unconfirmed transfers. World Health Organization (WHO) recommends digital tracking combined with decision support to enhance HCWs’ responsiveness. 36 Additionally, Schwebel and Lamrimer's 37 review found text reminders effective in appointment management with patients in over 80% of studies, suggesting similar benefits may be realized for HCWs managing transfer-outs.
The other finding was timing variations for tracing, where the 30-day and 60-day thresholds were used to trace defaulters. Studies have highlighted timing variations in the general population of people living with HIV and have further shown that timing thresholds differ in their effectiveness.12,38,39 Using a shorter window period for tracing is ideal because it may reduce the risk of vertical transmission of HIV associated with delayed reengagement. 40 The unique identification of women across services or spans of time and space is a well-known gap.41–43 The current management of identifiers during clinic switching in Malawi entails that an ART client is assigned a new ART number that is based on the transfer-in site ART numbers. 9 Our result shows that women identified as silent transfers during emergency refills were mostly registered as newly diagnosed clients. This may highlight a shift in which HCWs prioritize ART continuity over focusing on transfer procedures, and access to ART has become easier for mobile clients.
The monitoring strategies found in this study align with those identified in other research, including interfacility collaboration, tracing methods, record review, escorting of women, and self-reports.44,45 Furthermore, the results showed that an instant messaging app (WhatsApp) was used for interfacility collaboration and was considered efficient. This mirrors the broader trend within the healthcare sector, where there is a notable informal use of the app in health facilities, alongside increasing advocacy for its formal integration.46–48 The findings suggest that this technology offers an alternative communication solution for interfacility collaboration, which could enhance tracing efforts. However, it is imperative to establish guidelines to safeguard women's privacy and address any legal, regulatory, or ethical concerns that may arise with its widespread adoption.49–51 Furthermore, exploring technology functionalities to enhance monitoring is needed, given its self-propelling nature. Our results also showed that the escorting of women was predominantly utilized during linkage visits, which is consistent with the initial focus on access and uptake to the PMTCT program. This strategy needs to be used in subsequent visits, especially in the perinatal period. Patient escorting is said to increase patient satisfaction and reduce anxiety, 52 which may be key in reducing women's disengagement.
Resource constraints including human and operational resources (inner setting: availability of resources), hindered follow-up, aligning with prior research.53–55 For human resource challenges, there is a need to explore staff ratios in the monitoring workflow to avoid an overload of work, which may compromise the quality of work. 56 Methods such as workload analysis, time-motion studies, and benchmarking against established standards could be employed to evaluate current staffing levels.57–60 Adjusting staff ratios based on these assessments could help prevent work overload and in turn, may optimize engagement monitoring to Option B+. Additionally, the quality of work is also challenged by poor remuneration.61,62 This may explain our finding of the prioritization of incentivized tasks or demanding incentives to undertake a monitoring task or the poor work attitude toward monitoring tasks (characteristics of individuals: culture). A lack of operational resources (airtime, transport, and standard tools for tracing) may force HCWs to use their own resources, thus demotivating HCWs from working with diligence. 61 Therefore, continued support from development partners and adequate funding from the government is needed; otherwise, the implementation of interventions/strategies will remain suboptimal. This funding/support may transform facility leadership from mere motivators to drivers of change (inner setting: leadership). Data quality is often recognized as a hindrance to effective monitoring. 17 However, it was surprising that HCWs did not frequently raise this concern (characteristics of individual: self-efficacy). This suggests a gap in understanding or prioritizing data quality monitoring workflows, which could undermine the effectiveness of monitoring efforts. 63 Employing a multipronged data quality improvement strategy that incorporates at minimum; routine audits, targeted training, real-time validation, and regular feedback may provide the necessary skillset and understanding to HCWs in turn may optimize monitoring efforts.64,65
HCWs recognized the need to address patient-level barriers to have an optimal monitoring process (outer setting: patient needs). The barriers corresponded with previous studies that identified stigma, disclosure, poor HCW attitudes, misconceptions (COVID-19), religion, and transportation as deterrents to women's engagement in PMTCT.24,38,66–70 Among these, stigma, disclosure, and HCW attitudes were salient, highlighting the crucial role of relationship dynamics in care engagement. This calls for innovative interventions to foster stronger relationships throughout the care journey, ultimately promoting self-management. 71 A review from developed countries suggests that combining skills training with technology-assisted interventions, such as phone counseling, may be effective. 72 Similarly, a Malawi study on noncommunicable diseases recommended peer-patient and support groups for fostering self-management. 73 These strategies could be adapted for Option B+. Education and counseling were identified as key mechanisms for client compliance, which aligns with the recognition of psychological issues as integral to HIV care. Additionally, tailoring message packages based on engagement outcomes should be considered, as evidence suggests personalization improves engagement and outcomes in behavioral interventions. 74 For instance, Morrison et al 75 found that participants preferred tailored feedback over generic self-assessment due to its perceived personal benefit.
All in all, using the CFIR, the study revealed the deep interconnection of the inner setting, external setting, and characteristics of individuals with each domain influencing and being influenced by the others. Like, resource availability affects leadership engagement and organizational culture, which in turn impacts HCWs’ self-efficacy and knowledge. Similarly, patient-level barriers affect how well interventions are implemented and monitored, which is shaped by external policies and internal processes. Understanding these interconnections helps in identifying strategies for improving implementation and monitoring in healthcare settings.
The limitations of our study included using interview guides that were not structured to align with the CFIR constructs, which may have limited the exploration of some specific implementation areas. However, open-ended questions allowed participants to highlight the most prominent implementation areas from their perspectives. Additionally, the study was conducted in high-volume urban health facilities, which may not provide insights into rural or low-volume settings as they differ in contextual factors. Furthermore, conducting the study in one city in Malawi may affect the transferability of findings to other settings. Future research should consider these differences to improve applicability across diverse settings.
Conclusion
The study highlights various monitoring techniques, including interfacility collaboration, tracing methods, and record review. It also identifies gaps in the monitoring process, such as variations in tracing timing, lack of tracking for formal transfers, and inadequate differentiation in guidelines. Barriers to monitoring include resource constraints, challenges experienced by women, and poor work attitudes, while facilitators include implementing partner support and strategies for sustained engagement. This study emphasizes the importance of addressing relationship dynamics and implementing interventions to promote self-management. However, limitations in the study design and participant selection should be considered. Overall, this research provides valuable insights that can guide improvements in monitoring practices for optimal care delivery.
Supplemental Material
sj-pdf-1-jia-10.1177_23259582241299006 - Supplemental material for Monitoring Patient Adherence and Follow-up in Option B+ Program: Understanding Healthcare Workers’ Practices, Challenges, and Facilitators in Lilongwe, Malawi
Supplemental material, sj-pdf-1-jia-10.1177_23259582241299006 for Monitoring Patient Adherence and Follow-up in Option B+ Program: Understanding Healthcare Workers’ Practices, Challenges, and Facilitators in Lilongwe, Malawi by Wiza Kumwenda, Angela M. Bengtson, Shaphil Wallie, Agatha K. Bula, Jimmy Ba Villiera, Edith Ngoma, Mina C. Hosseinipour and Victor Mwapasa in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We gratefully acknowledge the study participants who took their valuable time to participate in this study as well as Zione Bonomali, Emmie Msiska, Tarsizious Chikaonda, Mercy Tsidya, Annie Thom, and Yamiko Phiri for their assistance with data management.
Author Contributions
WK led the conception and design of the study; conducted the data cleaning, analysis, and interpretation; and wrote the manuscript. SW and EN were involved in the implementation of the study and reviewed the manuscript. JV was an independent qualitative analyst involved in the data analysis and interpretation and reviewed the manuscript. AKB provided guidance on the qualitative design and analysis and reviewed the manuscript. AMB, MH, and VM supervised the conception and design of the study and reviewed the manuscript critically for important intellectual content. All the authors have read and approved the final manuscript.
Availability of Data and Materials
The dataset (which includes individual transcripts) is not publicly available due to confidentiality policies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Africa Center of Excellence in Public Health and Herbal Medicine, Kamuzu University of Health Sciences, Malawi HIV Implementation Research Scientist (MHIRST) Training Program, National Institute of Mental Health (grant numbers 151847, D43TW010060, and R00MH112413).
Ethical Approval and Informed Consent
This study was approved by the National Health Research Science Committee (approval no. 18/08/2137). All participants provided written informed consent prior to enrolment in the study. To maintain privacy and confidentiality, the consenting process and interviews were performed in a private place chosen by the participant within their respective facility.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.