
Abstract
Background:
Describing factors related to high attrition is important in order to improve the implementation of the Option B+ strategy in Haiti.
Methods:
We conducted a retrospective cohort study to describe the variability of antiretroviral therapy (ART) retention across health facilities among pregnant and lactating women and assess for differences in ART retention between Option B+ clients and other ART patients.
Results:
There were 1989 Option B+ clients who initiated ART in 45 health facilities. The percentage of attrition varied from 9% to 81% across the facilities. The largest health facilities had 38% higher risk of attrition (relative risk [RR]: 1.38, 95% confidence interval [CI]: 1.08-1.77, P = .009). Private institutions had 18% less risk of attrition (RR: 0.82, 95% CI: 0.70-0.96, P = .020). Health facilities located in the West department and the South region had lower risk of attrition.
Conclusion:
Being on treatment in a large or public health facility or a facility located in the North region was a significant risk factor associated with high attrition among Option B+ clients. The implementation of the Option B+ strategy must be reevaluated in order to effectively eliminate mother-to-child HIV transmission.
Introduction
With an HIV prevalence of 2.1%, Haiti has the second highest HIV prevalence and the highest number of people living with HIV in the Caribbean region. 1 In recent years, Haiti’s national HIV program has achieved many improvements in access to testing and care services which have contributed to a stabilization of the epidemic. 2,3 Antiretroviral therapy (ART) service availability expanded from 41 sites in 2008 to 131 in 2013. 4 Prevention of mother-to-child transmission of HIV (PMTCT) services expanded from 36 sites in 2004 to 137 in 2013. 5 Increased coverage of ART and PMTCT services contributed to an improvement in patient survival and a reduction in new HIV infections from mother to child. 6
In June 2011, at the United Nations (UN) General Assembly High Level Meeting on AIDS, Haiti adopted the declaration on intensifying the efforts to eliminate HIV/AIDS. 7 This statement included a commitment to work toward the elimination of mother-to-child transmission of HIV by 2015. During the same period, July 2011, Malawi implemented an innovative approach that increased the number of HIV-positive pregnant and breastfeeding women who started ART. 8 This strategy, called Option B+, removed the barrier of requiring a CD4 count to determine eligibility for treatment versus prophylaxis among HIV-positive pregnant women. Prior to 2012, Haiti’s national guidelines recommended that HIV-positive pregnant women with CD4 count ≤350 cells/mm3 or pregnant women in World Health Organization (WHO) clinical stage 3 or 4 be enrolled on a lifelong ART irrespective of their gestational age. Pregnant women who did not meet those criteria were recommended to initiate ART starting at the 14th week of gestation until childbirth if not breastfeeding or until 1 week after cessation of breastfeeding. In 2012, following Malawi’s experience, the Haitian Ministry of Health (MOH) updated guidelines of care for pregnant women to accelerate HIV testing among pregnant women and early treatment of all HIV-positive pregnant women. With the adoption of the Option B+ strategy, ART for HIV-positive pregnant and lactating women was no longer limited to prophylaxis during pregnancy and the breastfeeding period but was offered as lifelong treatment regardless of CD4 count.
Studies in countries implementing Option B+ show an increased coverage of ART treatment initiation among pregnant and lactating women. 8,9 However, retention in treatment is an ongoing challenge. 10 -12 Indeed, continuity of the treatment is critical for reducing risk of HIV transmission to others, and retention in care is one of the early warning indicators (EWIs) established by the WHO to monitor HIV drug resistance. 13 Monitoring EWIs informs national HIV programs of situations and practices that might favor the emergence of HIV drug resistance and provides an opportunity to take corrective actions.
In Haiti, studies on retention 14,15 are regularly conducted at the national level to provide the national HIV program and its nongovernmental implementing partners adequate information to monitor the program and prevent the emergence of resistance to ART. In a national study, the MOH described the retention of the cohort of ART patients who started treatment in 2011. The retention rate was 73.3% of ART patient retention rate at 12 months. Among the 26.7% of patients who were inactive, 62% were lost to follow-up (LTFU) and 23% had died. 15 Following the application of the Option B+ strategy in Haiti, another study on retention that included pregnant women was reported by Domercant et al. 16 Comparing ART attrition among men, nonpregnant women, and Option B+ clients, the study showed that Option B+ clients had 1.5-fold excess risk of attrition at 12 months compared to other adults (relative risk [RR] = 1.47, 95% confidence interval [CI] = 1.37-1.58, P < .001). 16 This Option B+ retention study highlighted several risk factors associated with high attrition, including younger age, rapid initiation in ART after HIV diagnosis, initiation of ART late in pregnancy, less advanced HIV disease state, and no uptake of counseling services. A contemporaneous mixed-method study led by the MOH, involving interviews with health-care providers and women who were LTFU in the PMTCT cascade, grouped reasons that led to ART discontinuation into 2 categories. 17 Community factors included transportation fees, distance to health facility, beliefs, lack of food, and relocation. Institutional factors grouped side effects, waiting time, concerns about lack of confidentiality, and inhospitable clinic as barriers to retention on ART. 17
This analysis uses the same cohort as the study by Domercant et al 16 to measure and explain the differences in retention across facilities. We will (1) describe the variability in ART retention across health facilities among pregnant and lactating women enrolled on ART from October 2012 to December 2013 in 45 health facilities in Haiti, (2) assess differences in ART retention between Option B+ clients and other ART patients and describe the variability in this comparison across health facilities, and (3) explore facility-level factors associated with ART retention among Option B+ clients.
Methods
Study Setting
Haitian health facilities offering ART services began implementing Option B+ in October 2012. Haiti adopted Option B+ in its national guidelines in the following ways: The initiation of lifelong treatment immediately after the confirmation of an HIV-positive test of a pregnant or lactating woman; The availability of CD4 results no longer required to start lifelong ART among pregnant or lactating women; and The ART regimen tenofovir/lamivudine/efavirenz (TDF/3TC/EFV) as the first choice for ART initiation.
In Haiti, health facilities that provide ART use one of the 3 available electronic medical records (EMRs) to register patient visits. iSanté, the largest EMR, covers 71 of the 131 national ART facilities that are located in 9 of the 10 health departments of the country. 18 The proportion of patients newly enrolled on ART in the iSanté EMR represents 70% of the national ART enrollments. Among the 71 sites, we selected those that enrolled at least 10 pregnant women on ART between October 2012 and December 2013. Forty-five sites met this criterion. We conducted a retrospective cohort study using deidentified data extracted from the iSanté central server located at the MOH.
Study Population
We collected information on all Option B+ clients and other patients enrolled on ART within the study period in the 45 heath facilities and the characteristics of these health facilities. Patients who did not have a registered age or sex were excluded from the analysis. We used the date the patient picked up ART at the pharmacy for the first time to determine the date of enrollment on ART. We followed up the patients by registering all pharmacy visits for ART pickups during the year following the starting date of their ART. Attrition, defined as a documented death or a patient LTFU, was the outcome of the study. The patients LTFU at 12 months were those who were not reported as deaths or transfers and who did not have evidence of having received ART within the time window from 270 to 365 days following the date of their ART initiation (a programmatic definition used by the MOH in its routine analyses of 12-month retention).
Data Analysis
Many factors might determine health behavior by motivating a patient to seek care or by impeding this behavior to occur. In his model of health services utilization, Andersen grouped those factors into 2 large categories: the population and the environment characteristics.
19
According to the variables available on the EMR, we were able to collect Option B+ client characteristics such as: Client demographics: age, marital status; Client clinical information: WHO stage, number of days for ART initiation after HIV test, regimen, trimethoprim/sulfamethoxazole (TMS), and tuberculosis (TB) prophylaxis; Client laboratory results: CD4 count, hemoglobin; Clients follow-up: number of counseling sessions.
The environment characteristics available on the EMR were the following: The size of the health facilities: The 45 study health facilities were divided into 4 groups by the number of Option B+ clients enrolled during the study period (10-25 clients, 26-35, 36-55, and the health facilities that enrolled more than 55 Option B+ clients); The network the health facility belongs to, according to the nongovernmental organization (NGO)/MOH partner that supervises the health facility: In Haiti, all health facilities that provide ART services are supervised by an NGO or other institution partner of the MOH. In this study, there were 9 MOH partners who were responsible for the ART program management of the 45 sites. The MOH partners who supervised at least 6 health facilities among the selected facilities were separately included in the analysis. The MOH partners who supervised 5 or fewer health facilities enrolled in the study were categorized as other.
We collected other environment factors from the Service Provision Assessment (SPA) data set and the national master health facility list
20,21
: The type of health facility: There were three types of health facility (public, faith-based, and private). The department where facilities were located: The 9 departments included in the study were categorized into 3 regions. Grand Nord grouped the sites located in North, North West, North East, and Artibonite. Ouest included only the sites of the West department. Grand Sud grouped the sites located in Grand Anse, South, South East, and Nippes. Urban or rural location as designated in the MOH classification of health institutions used in the SPA of 2013. The level of organization of the institution: The structure of the Haitian health system has 3 levels of organization.
22
The primary level includes first-level health facilities with or without bed and referral community hospitals. The second level includes the 10 department hospitals. The third level includes the university hospitals of the country. In this analysis, because of the small number of level 3 health facilities in the data set, we grouped level 2 and 3 facilities together and compared them with level 1 facilities.
Descriptive statistics for Option B+ women included the medians and interquartile ranges (IQRs) for the continuous variables (age, CD4 count, and number of days for ART initiation after HIV test) and frequencies and percentages for each categorical variable (WHO stage, marital status, number of counseling sessions, regimen, TB, and TMS prophylaxis).
To illustrate the pattern of attrition of Option B+ clients across health facilities, for each health facility, we computed attrition rates for Option B+ clients versus other adults. To compare these attrition rates, we calculated the RR of attrition and 95% CI.
Finally, using data from Option B+ clients at all facilities, we conducted a multivariable analysis to assess the relationship of facility variables with the risk of attrition, adjusting for individual-level patient risk factors. We used a modified Poisson regression model with log link and robust standard errors to estimate RRs of attrition and 95% CIs. The model incorporated generalized estimating equations with working exchangeable correlation structure to account for correlation among patients at the same facility. 23 Predictor variables included all health facility characteristics and all patient characteristics previously described. The level of significance was set at a P value of <.05. We used Stata 12 (Stata Corp, College Station, Texas) to conduct the data analysis.
Ethical Review
The study involved secondary analysis of deidentified patient data and was granted a nonhuman subjects research exemption by the University of Washington Human Subjects Division. The study took place with approval of the US Centers for Disease Control and Prevention and the National Bioethics Committee of the Haiti MOH.
Results
The study population included 1989 Option B+ clients with a median age of 28 years (IQR: 23-33 years; Table 1). Clinically, among the 68% of Option B+ clients with a registered WHO stage, 92% were at stage I/II. In regard to the timeliness of initiating Option B+ clients on ART, among the 76% of clients with a registered date of HIV test, about 34% started ART the same day as the result of their HIV test. Cumulatively, 54% of them initiated the treatment within 1 week after the result of their HIV test. Following the guidelines of the national HIV program, 98.8% of the cohort was placed on treatment using one of the first-line regimens. Tenofovir + lamivudine + efavirenz (TDF/3TC/EFV) was the first choice regimen for initial ART used (80.8%); 66% of the Option B+ clients received TMS prophylaxis.
Characteristics of Option B+ Clients.a

Abbreviation: ART, antiretroviral therapy; EFV, efavirenz; IQR, interquartile range; TB, tuberculosis; 3TC, lamivudine; TDF, tenofovir; TMS, trimethoprim/sulfamethoxazole; WHO, World Health Organization.
a N = 1989.
Among 60% of women who had a baseline CD4 count available, the median CD4 count was 496 cells/μL (IQR: 331-678 cells/μL). Among the 49% of women who had a hemoglobin concentration available, 27% had a moderate or severe anemia.
The PMTCT guidelines describe the counseling sessions that HIV+ pregnant or breastfeeding women must receive prior to ART initiation and at each visit. The counselor is required to discuss treatment adherence, infant-feeding options, social support, and family planning. Moreover, counselors are encouraged to take a patient-centered approach in communicating with women about their situations and needs. Although counseling sessions offer a great opportunity for in-depth discussion between the health-care worker and the Option B+ patient, we found that 87% of the women were enrolled without a registered counseling session.
Half of the 45 health facilities enrolled fewer than 36 patients during the period (IQR: 24-55); 40% of the facilities were public institutions. More than a third (36%) of health facilities was located in the West department. The facilities were more likely to be located in an urban area (82%) and to be of level 1 category (58%; Table 2).
Site Characteristics.

Abbreviation: NGO, nongovernmental organization.
There was a large difference in the level of attrition after 12 months among Option B+ clients, which varied from 9% to 81% across the 45 health facilities. Nineteen (42%) sites had 50% or more cases of attrition among their Option B+ clients. Only 2 (4%) sites were able to reach WHO’s target of maintaining more than 75% of their cohort on treatment (having attrition lower than 25%) for 1 year (Figure 1).

Attrition rate of Option B+ clients across health facilities. Red line: Mean attrition rate across all sites.
Forty-three (95%) health facilities had a higher risk of attrition among Option B+ clients compared to other adults on treatment (Figure 2). In the 2 health facilities where the percentage of attrition was higher in other adults compared to Option B+ clients, the difference in attrition between both groups was not statistically significant (Figure 3). In contrast, among the 43 health facilities with higher attrition among Option B+ clients, in 21 (nearly 50%) of the 43 facilities, the difference was statistically significant.
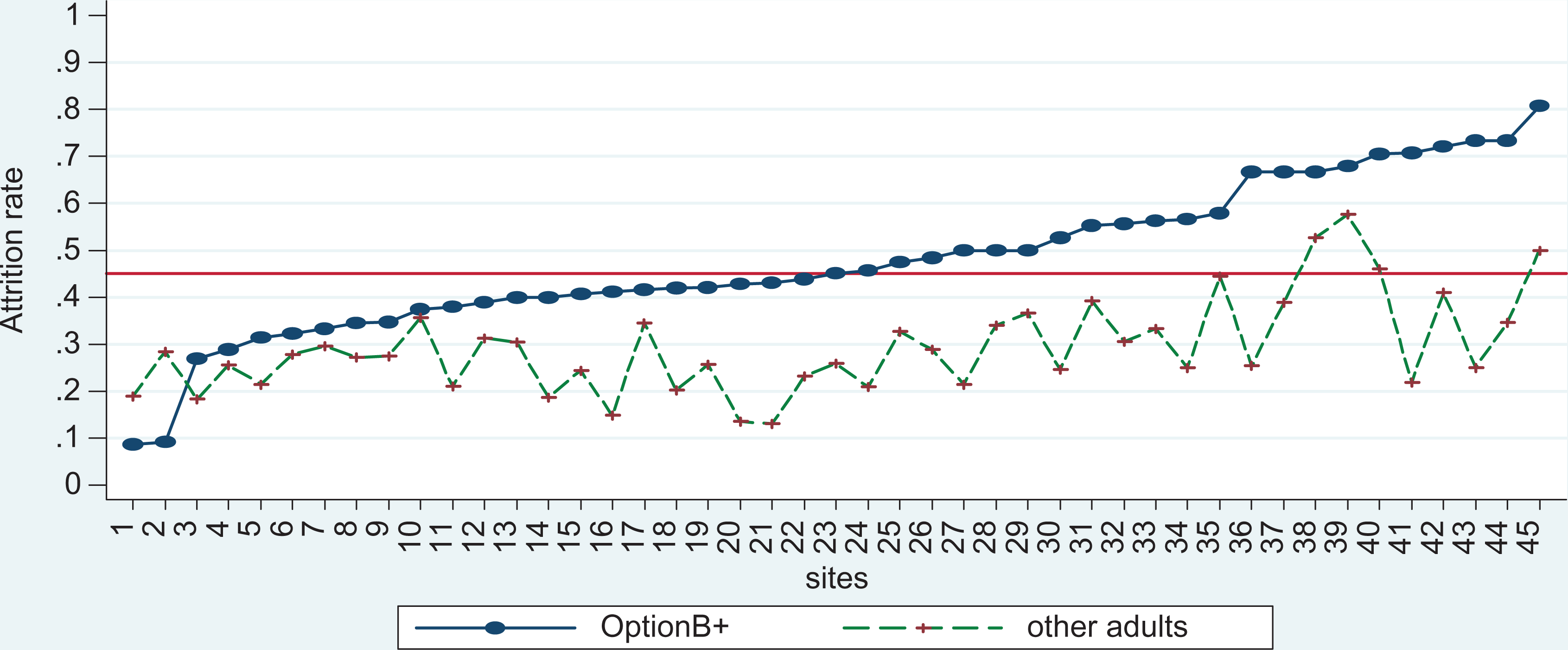
Comparison of attrition rate between Option B+ clients and other adults across health facilities. Red line: Mean attrition rate across all sites.

Relative risk of attrition for Option B+ clients compared to other adults. Red line: Null value.
The RR of attrition for Option B+ clients compared to all other adults enrolled on ART varied from 0.32 to 3.24 (Figure 3). Among the 19 health facilities that had 50% or more of their Option B+ cohort no longer on ART after 12 months, 11 (58%) had a significant difference in the risk of attrition for Option B+ clients compared to other adults enrolled on treatment at the same health facilities.
In the multivariable analysis (Table 3), the largest health facilities (those that enrolled more than 55 Option B+ clients) had 38% more risk of attrition (RR: 1.38, 95% CI: 1.08-1.77, P = .009) compared to the smallest health facilities (10-25 Option B+ clients). Compared to public health facilities, faith-based and private institutions had 18% (RR: 0.82, 95% CI: 0.70-0.96, P = .020) and 23% (RR: 0.77, 95% CI: 0.65-0.93, P = 0.006) less risk of attrition, respectively.
Risk Factors Associated with Attrition.

Abbreviation: ART, antiretroviral therapy; CI, confidence interval; EFV, efavirenz; NGO, nongovernmental organization; TB, tuberculosis; 3TC, lamivudine; TDF, tenofovir; TMS, trimethoprim/sulfamethoxazole; WHO, World Health Organization.
Health facilities located in the West department and the South region had significantly lower risk of attrition than those located in the North region, respectively (RR: 0.74, 95% CI: 0.64-0.85, P < .001; RR: 0.69, 95% CI: 0.52-0.90, P = .007). There was a substantial significant difference between attrition among 3 MOH partner networks. Compared to network A, network C had 51% higher risk of attrition (RR: 1.51, 95% CI: 1.19-1.91, P = .001) and network D had more than 100% higher risk of attrition (RR: 2.14, 95% CI: 1.59-2.87, P = .001). Level of facility within the Haitian health system pyramid was marginally associated with attrition, while location in urban versus rural areas was not significantly associated with attrition in this study.
Several individual-level factors showed significant associations with attrition (Table 3). Protective effects included older age (RR: 0.97, 95% CI: 0.96-0.98, P < .001), enrollment on ART at least 1 day after the date of the HIV test (RR: 0.82, 95% CI: 0.71-0.94, P = .006), realization of counseling sessions before enrollment on ART (RR: 0.81, 95% CI: 0.74-0.89, P < .001), and prescription of TMS prophylaxis (RR: 0.88, 95% CI: 0.78-0.99, P = .043). Having a moderate/severe anemia was a risk factor (RR: 1.23, 95% CI: 1.04-1.44, P = .011).
Discussion
Like several other countries, 9 -11 Haiti is experiencing challenges related to retention on HIV treatment among Option B+ clients. Overall, 50% of Option B+ clients were no longer on treatment 1 year after the initiation of ART. This result is far above the national rate of 27% of 12-month attrition among all newly enrolling adult ART patients. Prior studies have discussed Option B+ client characteristics associated with high attrition 16 as well as community and institutional factors that influenced Option B+ clients to discontinue their treatment. 17 Our present analysis provided additional information by describing variability in the attrition phenomenon across health facilities and by analyzing associated health facility factors.
Key Findings
High variability of outcomes across facilities
We observed an extremely high variability among health facilities in attrition of Option B+ clients. The size of the site, the category, the region, and the MOH partner network were important factors affecting retention. Other countries that have analyzed attrition among their Option B+ cohorts have also described the variability of ART retention across health facilities. In Malawi, the difference in ART attrition varied from 4% to 29% across 141 health facilities after a period of 6 months. 24 In Mozambique, the difference in ART attrition between 6 health facilities ranged from 5% to 32% after 90 days. 25 In this analysis, we observed a difference that varied from 9% to 81% across health facilities after 1 year.
In Malawi, as in our study, higher attrition was observed in large health facilities and those managed by the MOH compared to small, faith-based, and private facilities. 10 However, contrary to Malawi, our study did not find any association between attrition and the category of health facility (level 1 or levels 2 and 3) or site’s location in urban or rural region, after controlling for other covariates.
Notable disparities in outcomes for Option B+ clients compared to other adults
A particularity of this study was the comparison of retention among Option B+ clients and other adults enrolled on treatment at the same period to determine whether higher or lower attrition levels were consistent across all groups of patients. The finding that a large number of health facilities (21/45, or 47%) had significantly higher levels of attrition among Option B+ clients compared to other adults indicates that there are unique challenges to successfully treating pregnant and lactating women on ART. Indeed, after the diffusion of the new PMTCT guidelines, health facilities had the responsibility to determine the best way to implement the strategy. Few of them succeeded. A lot might be learned from the health facilities which were “positively deviant”—those that had a very low attrition and those where there were no disparities between Option B+ clients and other adults. Studying these sites could reveal best practices which could be taken up by other sites.
Incomplete compliance with PMTCT guidelines
Our study also provided evidence about the extension of the application of the new PMTCT guidelines. Compliance with PMTCT guidelines was modest, with room for improvement. Use of recommended first-line regimens was high, but only a little more than half of clients with known HIV testing dates were started on ART within 1 week of their test. In regard to the timeliness of the treatment initiation, we observed that almost a quarter of the Option B+ clients did not have a registered date for their HIV test (23.6%). The missing values might be related to the lack of connection between Voluntary Counseling and Testing (VCT) Center and ART services. This analysis also showed that nearly 90% of Option B+ clients lacked record of an ART counseling session before ART initiation, a percentage that was higher than for other adults (men or nonpregnant women) who initiated ART during the same period (60%). 16 According to the guidelines, an ART adherence counseling session must be done before the initiation of ART.
Limitations
Although iSanté is the largest EMR in Haiti, the findings cannot be generalized to the national level. Moreover, data quality in terms of low completeness of data or underreported transfers might have led more patients to be classified as LTFU in some sites more than others. Also, the factors we analyzed are not exhaustive. Based on Andersen model, other factors might have influenced the implementation of the strategy. Among the population characteristics, some unmeasured factors are income/occupation, education, family, geographic access, health and cultural beliefs, and social support. Among environment characteristics, other unmeasured factors are the human resources available to provide the service, the tracking of patients, and the integration of services (antenatal clinic [ANC]/ART).
Although we were able to analyze many individual- and facility-level factors, we did not have the ability to analyze the organization of the services in health facilities, a potentially important factor that might explain better performance in some facilities compared to others. In Haiti, PMTCT services are organized differently depending on the health facility; 56% of ANCs with the capacity to offer HIV testing do not provide ART services. 20 Therefore, those clinics refer HIV-positive women to other sites for ART initiation. In other health facilities, the integration of PMTCT into ANCs needs to be strengthened. 26 A study in Malawi took into consideration the model of care when assessing the performance of health facilities. 24 The study showed that highest retention rates among HIV-positive pregnant and lactating women occurred when the women initiated their ART in dedicated ART programs (in facilities both with and without ANC services), rather than when women initiated ART within the ANC setting and were later expected to transfer care to an ART clinic for follow-up. Further study of the role of organization of services in Option B+ client retention is needed in Haiti.
Finally, the lack of record of counseling session before ART initiation could have ambiguous meaning. The electronic version of the counseling form is available in the EMR to be filled out for each patient. However, we cannot distinguish whether the absence of a documented counseling session means that no counseling was done or that it was done but simply not documented by the health-care workers.
Recommendations
In order to improve retention among HIV-positive pregnant women, various countries have developed different strategies. These include integration of community health workers, quality improvement interventions, peer-based education, and psychosocial support or the availability of a mother support group for HIV-positive women at the facility. 27 -31 Health facilities that had better retention rates in our analysis may have put in place additional measures to enhance service delivery while implementing the Option B+ strategy. An evaluation of their strategies could help the MOH make adequate recommendations to ensure long-term treatment for HIV+ women who initiated ART during pregnancy or lactation.
Using results and recommendations available from previous studies, Haiti’s national HIV program should discuss with the MOH partner networks a reorganization of the services in terms of tracking of missed visits, adequacy of human resources, quality and realization of counseling, and education sessions. According to the results of this study, although the program should prioritize quality improvement in the large, public sites and the sites located in the North region, appropriate interventions should be planned in all health facilities to increase patient treatment adherence and improve health outcomes.
The national HIV program recently updated guidelines of HIV care to apply a “test and start” approach to long-life antiretroviral treatment for all HIV+ adults and adolescents, regardless of their CD4 count. 32 As learned from the implementation of the Option B+ strategy, the diffusion of new guidelines must be supported by adequate evaluations of resources available and constraints in the organization of the services in order to strengthen the health system to ensure the continuity of a quality service to the population. In Haiti, the methodology HIVQUAL/HEALTHQUAL 33 had helped achieve a great improvement in quality of care in the HIV program. With the availability of EMRs in all health facilities, a quarterly follow-up of cohort of patients is feasible. Therefore, in addition to feedback from yearly evaluations, health facilities must be encouraged to consider retention on treatment as an indicator for quality improvement projects.
Conclusion
Analyzing attrition among 45 health facilities implementing Option B+, this study revealed that retention on HIV treatment was a general concern among the Option B+ clients in Haiti. Only 2 (4%) sites had <25% attrition at 12 months among Option B+ clients. Twenty-one (47%) sites had a significantly greater RR of attrition among Option B+ clients compared to other adults. In the most extreme case of disparity, the excess risk of attrition among Option B+ clients reached 3 times the risk of attrition of other adults on treatment. In the adjusted analysis, public, largest health facilities, and those located in the northern region of Haiti were more likely to have higher attrition. The organization of care services in PMTCT health facilities is likely be associated with attrition among Option B+ clients, and further research is needed in order to identify adequate models of care and guide the elaboration of new policy recommendations.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention, the National Institutes of Health, or the Health Resources and Services Administration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the Health Resources and Services Administration, under award number U91HA0680, and the US Centers for Disease Control and Prevention, under award number GH001130, to the International Training and Education Center for Health (I-TECH) at the University of Washington. Research reported in this publication was also supported by NIAID, NCI, NIMH, NIDA, NICHD, NHLBI, NIA, NIGMS, and NIDDK of the National Institutes of Health under award number AI027757 to the University of Washington Center for AIDS Research (CFAR).