
Abstract
Objective
This study investigated women living with HIV/AIDS (WLHA)'s practices and decision-making regarding disclosure of HIV status in healthcare settings in Vietnam.
Methods
We conducted in-depth interviews with 30 WLHA in Hanoi, Vietnam. Thematic analysis was conducted to investigate the patterns, considerations, and consequences of HIV disclosure.
Plain Language Summary
This study focuses on how women living with HIV/AIDS in Vietnam decide to share their HIV status with healthcare providers. We interviewed 30 women with HIV/AIDS in Vietnam and found that many choose to reveal their status only in certain situations, depending on the medical procedure and the setting. They weigh various factors before deciding to disclose, including the risk of facing stigma, the need to protect their privacy, how relevant their HIV status is to their other health issues, their wish to protect their healthcare providers and other patients, and how they have been advised by HIV specialists. Unfortunately, choosing not to disclose their status sometimes stops them from getting the full range of medical care they need. The findings stress the importance of helping these women make well-informed choices about disclosing their HIV status. We also need to provide them with additional support and navigational help through healthcare services. Moreover, reducing stigma in healthcare, enhancing providers' ability to gather necessary health information, and ensuring patient privacy are crucial to encouraging more open discussions of HIV status in medical settings.
Introduction
With advancements in effective treatment, HIV infection has now become a manageable chronic disease. The life expectancy of people living with HIV has increased substantially over the last 25 years. 1 This positive trend underscores the growing importance of addressing the broader medical needs of the population living with HIV. 2 Disclosing one's HIV status to healthcare providers poses a considerable challenge for people living with HIV on a global scale.3-6 People living with HIV are not obliged to disclose their HIV status when seeking general healthcare services. 7 Choosing not to disclose HIV status can help individuals avoid emotional distress, stigma, discrimination, and potential breaches of confidentiality along with associated social repercussions.6,8,9 However, withholding information about their HIV-positive status and ongoing antiretroviral therapy (ART) can result in suboptimal management of co-infections, potential complications from drug interactions, and overlooked effects of HIV infection on the progression of other medical conditions.4,5
While the literature on HIV disclosure is abundant, recent studies providing insights into the factors that influence individuals living with HIV to either disclose or withhold their HIV status from healthcare providers are limited.3,6,8,10-12 A handful of studies conducted in Africa and the United States indicate that approximately 20% of individuals did not disclose their HIV status to healthcare providers.4,5,13 The main reason for non-disclosure was the fear of discrimination and rejection, often stemming from previous experiences of mistreatment in healthcare settings.4,8,13 Other factors included healthcare providers not inquiring about HIV status, the belief that providers did not need to know, and the absence of a consistent healthcare provider. 5 On the other hand, factors facilitating disclosure were a greater availability of HIV services, a trusting relationship with healthcare providers, and perceived social support.5,14,15
More than half of the global population living with HIV and 46% of all new HIV infections are women. Women living with HIV/AIDS (WLHA) face greater vulnerability to HIV infection than men for a variety of reasons.16-18 Biological factors, such as more exposure zones or a different immune activation, contribute to women's heightened susceptibility to HIV acquisition and faster disease progression.17,18 WLHA experience a unique set of social vulnerabilities, including a high prevalence of intimate partner violence, severe stigma, gender-based financial disparities, and educational inequities.19,20 As a result, they bear a substantial burden of mental stressors and unmet sexual and reproductive health needs.21-24 Additionally, WLHA faces limited access to healthcare and worse health outcomes.19,20,25,26
Over the last two decades, Vietnam, a Southeast Asian country, has made significant progress in expanding HIV treatment services, reaching 82% of the 183,458 individuals with known HIV positivity and achieving excellent viral suppression rates.27-29 Despite these achievements, HIV stigma persists as a significant challenge in the country. Surveys indicate that as many as 76% of the general population hold stigmatizing attitudes towards people living with HIV, and 26.1% of individuals living with HIV have reported experiencing HIV-related discrimination in healthcare settings within the past 12 months.27,30
WLHA, accounting for one-third of the population living with HIV in Vietnam, 27 face distinctive challenges attributed to gender norms that underscore their responsibilities as caregivers and the value placed on purity and modesty.21,31 In Vietnam, the societal expectations for women to have children place added importance on WLHA to seek reproductive healthcare services and consider disclosing their HIV status to receive prevention of mother-to-child transmission services, in order to safeguard the health of the child. 32 Nonetheless, the frequent linkage of HIV diagnosis to behaviors like substance use or extramarital sex often results in WLHA being stereotyped as individuals who have strayed from societal female virtues. 30 These stereotypes contribute to WLHA's internalized stigma, resulting in psychological stress and potentially creating additional barriers to disclosing their HIV status when seeking healthcare.
Between 2021 and 2022, we conducted a qualitative study in Vietnam to explore WLHA's stigma experiences, mechanisms to combat stigma, and barriers to service-seeking. 33 The analysis presented here focuses on the practices of disclosing HIV status to healthcare providers of Vietnamese WLHA, providing insights into their decision-making processes regarding disclosure and the potential consequences of disclosing/not disclosing their HIV status in healthcare settings.
Methods
The study was conducted among WLHA in Hanoi, the capital of Vietnam and the socioeconomic and medical center of the country. In 2022, it held the second-highest national ranking in terms of monthly income per person. 34 The city was home to 18 HIV outpatient clinics, providing care to over 14,000 people with HIV, of whom approximately 25% were female. 35
To recruit participants, we distributed study flyers with contact information in HIV outpatient clinics in Hanoi. Additionally, recruited WLHA were encouraged to invite their peers to participate. Eligible participants were 1) at least 18 years old, 2) female at birth, and 3) self-reported to be HIV-positive. We ensured diversity in our sample by including WLHA with varying background characteristics such as infection route, marital status, and parental status. Before initiating the interviews, participants were informed about the study's purpose, procedures, and potential benefits/risks. They were also informed that their participation was entirely voluntary. Verbal informed consent was acquired from each participant before the interview. The refusal rate of the study was approximately 10%.
Ethical Approval and Informed Consent
The study was approved by the Institutional Review Boards at the University of California, Los Angeles (IRB#21-001503) and Hanoi Medical University (TRB-VN0 l .001/IRB00003121).
Data Collection
The study team specifically developed the in-depth interview guide based on the study aims and the relevant literature to facilitate in-depth exploration of the WLHA's experiences and perspectives (please refer to the supplementary document). The interview guide was pilot-tested with three WLHA (who were not participants of the study) to ensure clarity and relevance. Thirty WLHA participated in in-depth interviews one-on-one with study interviewers between December 2021 and March 2022. Given the local COVID-19 situation at the time of the interviews, we offered participants the option of being interviewed either in person in a private room or via Zoom. The study interviewers (BDN, TTN, and DTH) were PhD and Master level researchers in public health; they are female native Vietnamese speakers with substantial training and experience in qualitative research. The interviewers did not have pre-existing relationships with the study participants or assumptions on the interview topics. They administered the interviews using a semi-structured interview guide with open-ended probes. The participants’ background characteristics, including their demographics and family backgrounds, as well as their HIV infection history were inquired at the beginning of the interview. The interview guide included questions about cultural beliefs about HIV and females living with HIV, stigma experiences in various settings (including families, workplaces, and communities), strategies for coping with stigma, and health-seeking needs and experiences. The interview specifically inquired about HIV status disclosure practices in different settings, considerations/planning of disclosure, and the consequences of disclosure or non-disclosure. Examples of questions were “Would you inform your non-HIV healthcare providers about your HIV status? Why and why not?” “In which circumstances would you reveal your HIV status?” or “Tell me an incident in which you disclosed your HIV status to a healthcare provider.” The interviews lasted 60–90 min and were audio recorded with participants’ consent. The interviewers took field notes of the date, time, location, and the participant's non-verbal reactions. Each participant received 300,000 VND (approximately 13 USD) to compensate for their time and efforts.
Data Analysis
The audio recordings were transcribed verbatim. All information that could potentially disclose participants’ identity, such as the name of the community and/or clinic, was removed from the transcripts. The Vietnamese transcripts were then translated into English to ensure that the data could be reviewed and analyzed by research team members in the U.S. The initial translation was conducted by study team members fluent in both Vietnamese and English. The interviewers then reviewed the translations of their own interviews to ensure accuracy and fidelity to the original content. The final English translations were imported into web-based ATLAS.ti, a platform that allows multiple coders to collaborate on coding simultaneously. 36
We applied a thematic analysis to the interview data. The coding was performed by a team of four investigators, including two who conducted the interviews. During the coding process, the coders frequently met to reach a consensus on code definitions, applications, and revisions. Data analysis was conducted simultaneously with data collection to monitor the emergence of new themes and ensure that thematic saturation was reached. We conducted an initial round of coding for the main paper, which was themed around cultural aspects of stigma facing WLHA in Vietnam. 33 For this particular paper that focused on HIV disclosure to healthcare providers, a more detailed analysis was conducted on the specific set of codes related to disclosure. Each transcript was revisited to distill the practices associated with disclosing one's HIV status to healthcare providers. Guided by the Disclosure Process Model, 37 we coded disclosure-related content into categories such as disclosure considerations/goals, disclosure contents, disclosure events, confidant, reaction of the confidant, and disclosure outcomes.
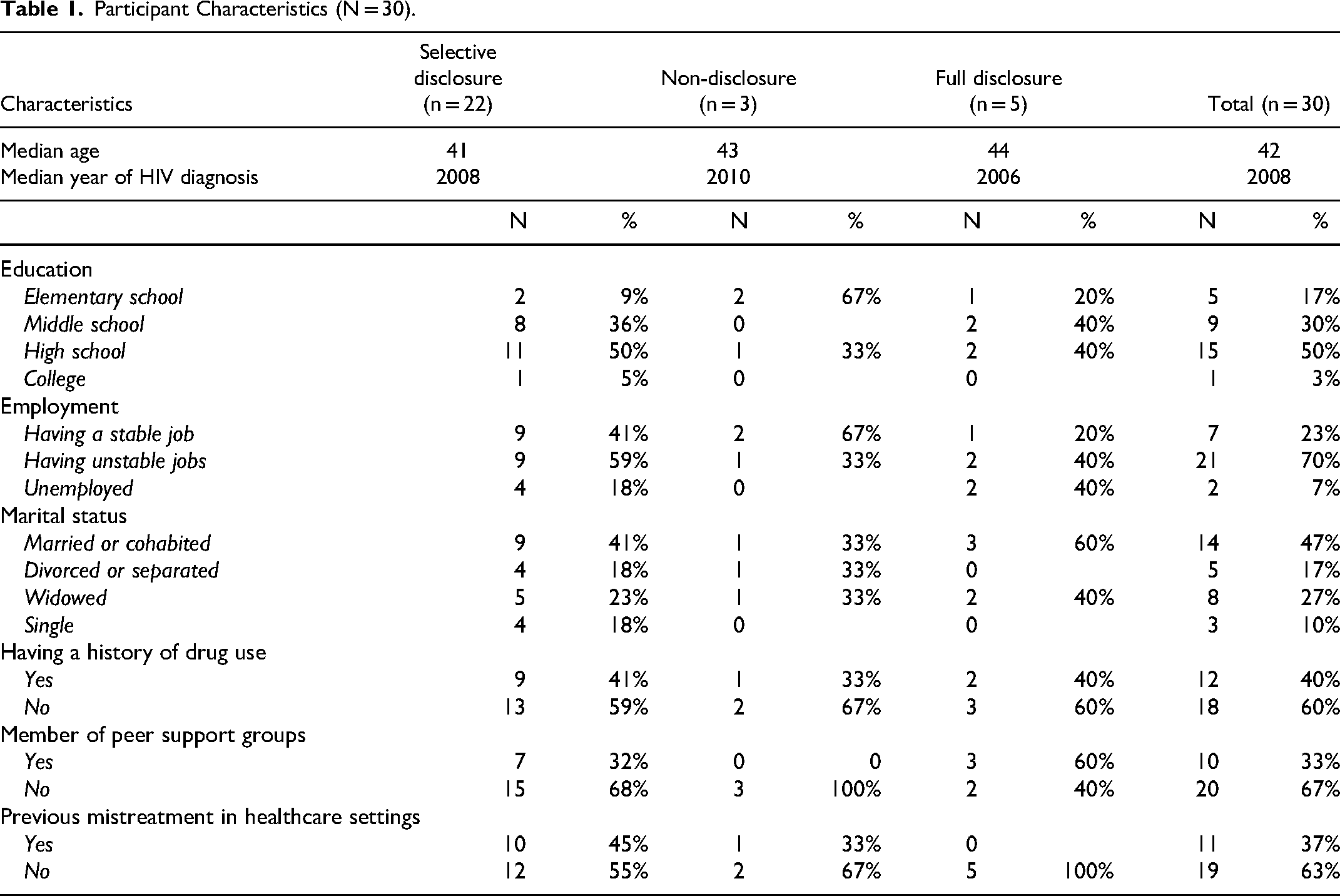
Drawing insights from existing literature, 14 we summarized the HIV disclosure patterns among participants with diverse characteristics, such as age groups, marital status, education attainment, employment, years of HIV diagnosis, substance use history, and support groups (Table 1). We described the disclosure patterns, disclosure/non-disclosure considerations, and consequences of disclosure/non-disclosure. We followed the COnsolidated criteria for REporting Qualitative research (COREQ) checklist to ensure comprehensive and transparent reporting of the qualitative research process.
Participant Characteristics (N = 30).
Results
Disclosure Patterns
The study participants’ characteristics and their disclosure patterns are presented in Table 1. The average age of the participants at the time of the interview was 42. Among the 30 participants, half had a high school education, the majority (70%) had unstable jobs, and less than half (47%) were married or cohabiting. Forty percent of the participants reported a history of drug use, and approximately one-third (37%) had experienced mistreatment in healthcare settings.
Three disclosure patterns were identified:
Disclosure/Non-Disclosure Considerations
When participants deliberated whether to disclose their HIV status, they weighed several critical factors, including concerns about stigma and discrimination, risks of confidentiality breach, relevance to healthcare provision, altruism, and advice from HIV providers.
Concerns of Stigma and Discrimination
Avoiding HIV-related stigma and discrimination was the primary factor influencing participants’ decisions not to disclose their HIV status in all or selective situations. Some participants shared their past experiences of stigma in hospital settings, including instances of unnecessary referrals and avoidance right after disclosure. These encounters significantly influenced their decision-making process when deciding whether to disclose their HIV status while seeking medical care.
I reached a nearby hospital, but they declined to facilitate childbirth for people with HIV. Consequently, I had to seek assistance at a higher-level hospital. (38 years old, widowed, employed, diagnosed with HIV in 2004)
Just that one, because I did experience… There were times when I was seriously ill, I disclosed that I was taking treatments for HIV. Next, they hurriedly told me that they didn’t have the department that I needed, and transferred me to another hospital. I had to start all over again. (40 years old, single, unstable job, diagnosed with HIV in 2014)
Participants were aware that healthcare providers are legally prohibited from discriminating against people with HIV; nonetheless, they remained concerned about the potential impact of implicit discrimination. One participant recounted an incident involving a friend:
My friend had uterine fibroids and her fibroids broke. When she came to one hospital, [the hospital] kept referring her to another one, then another one. […] Now people are smart. With many laws against discrimination, they won’t explicitly say you’re not treated because of your HIV. (45 years old, divorced, self-employed, diagnosed with HIV in 2003)
Risks of confidentiality breach. Participants believed that public, large hospitals in urban centers, especially those specializing in infectious diseases, carried lower risks of confidentiality breaches. This perception stemmed from the inherent trust in the training and professionalism of healthcare providers within major centralized, specialty care settings:
If I go to an infectious disease hospital, I can ask about my disease, I say it easily because many people like me go there, so it's nothing to be scared of… I think it's okay to be in upper-level hospitals, but in commune hospitals, sometimes people tend to gossip, I hesitate to go there (37 years old, married, unstable job, diagnosed with HIV in 2009)
There were mixed feelings about the public and private sectors: some expressed concerns about privacy protection in private clinics, while others felt more at ease disclosing their HIV status to private providers. The latter group cited that private providers often have more time for meaningful communication with patients:
Doctors at a private facility consider me as a patient, a customer so they are willing to listen to what I say. On the contrary, at a public one, the doctors have many patients … These doctors have to see the next patients so they cannot sit and talk to me or listen to what I say about my treatment process (40 years old, single, unstable job, diagnosed with HIV in 2014)
Several participants encountered inadvertent disclosure of their HIV status at commune health stations, resulting in significant turmoil and negative consequences in their lives. One participant shared her experience of involuntary HIV status disclosure in her rural residence:
When my test result was sent to my ward, they were publicly announced via loudspeaker. I was at home when four medical people suddenly entered my house. (50 years old, married, unstable job, diagnosed with HIV in 2005)
While this incident occurred nearly 20 years ago, it continued to weigh heavily on participants’ decisions regarding HIV status disclosure, because in close-knit communities where people often knew each other, participants lacked confidence in healthcare providers’ practice to maintain the confidentiality of their HIV status:
It depends on the situation, you know, if the clinic were not around my husband's place, I would disclose it to the doctors there. I mean, the main thing is that if people don’t reveal it to other people, then I will disclose my HIV status to them. (36 years old, married, unstable job, diagnosed with HIV in 2010)
Relevance to Healthcare Provision
One motivation for HIV status disclosure was the desire for more holistic care, as participants believed that knowing their HIV status was necessary for service providers to fully understand their situation and provide more appropriate and specialized care more efficiently.
When physicians know I have the virus and my antibodies are problematic, they’ll put me right in specialty care, no need to go around from room to room to all different departments. (36 years old, married, unemployed, diagnosed with HIV in 2003)
I just thought I should report my condition so that people at the clinics could understand. If I hid it, the doctors would go around in circles, then eventually figure out my illness and say, “why didn’t you tell me earlier? I could have focused directly on your problem. You are wasting both of our time”. I think they would say that. But honestly, from my point of view, if I have any conditions, I will definitely tell the doctors so that they can see the whole picture. (44 years old, married, unstable job, diagnosed with HIV in 2002)
Participants who chose selective disclosure strategies made their own judgment on whether the services they were receiving were relevant to their HIV status to decide on disclosure. For example, as stated above, health issues involving invasive procedures, such as surgery, or those requiring exposure to blood and other bodily fluids, were typically considered relevant for HIV disclosure. Conversely, several participants mentioned disclosure during routine checkups was unnecessary.
Yes, if it's not related to surgery. Normally, during the normal examination, I would not disclose it to anyone. I think I don't need to disclose it (44 years old, divorced, unstable employment, diagnosed with HIV in 2003)
This assessment, however, lacked standard criteria. For instance, while some participants considered skin issues significant enough to warrant HIV disclosure, others did not view dermatological concerns as related. Participants also reported conflicting decisions about disclosure in cases of ultrasound/x-ray examinations, respiratory diseases (eg, flu and COVID-19 infections), and gynecologic service seeking.
Despite being critical to the health of participants, potential drug interactions did not seem to factor into some of the participants’ decision-making regarding disclosure. Indeed, in situations of non-disclosure, participants would refrain from disclosing both their HIV-positive status and the use of ART medications.
Q: Have you ever worried that the doctor may prescribe something that will affect your ART? A: I’ve never thought about that. I've only asked how many pills to take a day or whether they should be taken after or before meals. (46 years old, single, female sex worker, diagnosed with HIV in 2009)
Altruism
Another motivation for participants to disclose their HIV status was to protect healthcare providers, especially in situations involving blood draws or invasive procedures. In addition, they highlighted the need to inform healthcare staff about their HIV status to ensure proper sanitization protocols were followed to safeguard not only healthcare providers but also fellow patients:
I would never allow people to take blood without telling people that I got it. Because firstly, I have to keep them safe, you know. (48 years old, married, stable job, diagnosed with HIV in 2018)
I should let them know. So as far as I know, when they examine me, they will go into my throat, right? Then their viruses will stick to the medical instrument so they will have to disinfect or do whatever to protect others. To protect other patients, the staff must sanitize [the stick used to inspect my throat] with a 10% solution specific to the virus. For other diseases, a one or two-percent solution might suffice. (33 years old, married, unemployed, diagnosed with HIV in 2021)
Advice from HIV Providers
Given the trust participants had in their HIV clinics, the advice of HIV treatment providers significantly influenced their decisions regarding disclosure when seeking non-HIV related services:
The physicians here will tell me where to go to treat my health issues. If they say that I can tell the other doctors, then I'll do it. (35 years old, married, unstable job, diagnosed with HIV in 2015)
Consequences of Disclosure/Non-Disclosure
Participants reported diverse experiences regarding the consequences of disclosing their HIV status in healthcare settings. While some indicated that disclosure could result in stigma and discrimination, a significant proportion of those who disclosed their status reported receiving additional support from healthcare providers afterward.
Yes, the doctor just took a magnifying glass and looked at my skin, but after I informed you that I had HIV and my skin was like that. I saw the attitude of the doctor was completely different. The doctor got up to wash his hands, his attitude was completely different. (35 years old, widowed, unemployed, diagnosed with HIV in 2009)
No discrimination at all. [The doctors and nurses] were very caring. […] They gave me two milk bottles and encouraged me to drink to gather strength for the birthing process. (44 years old, married, peer outreach worker, diagnosed with HIV in 2002)
On the other hand, non-disclosure caused participants to hesitate when it came to routine check-ups or examinations. This hesitation stemmed from their desire to keep their status private while also avoiding any dishonesty with healthcare providers. As a consequence, some participants ended up avoiding all non-HIV-related medical services.
Since I left, I have not gone for any general check-ups…I feel embarrassed. To be honest. It's nothing but I just felt reserved so I don't like it. We’re afraid of facing the problems. When I go there, if, unfortunately, they asked me to provide my health background and how I felt, then it would be kind of… Well, if I didn’t disclose it, I would be a liar, or if I really had to disclose it, I just don’t like doing so. So what I ended up with is that I always refrain from going to get the general check-ups done at the hospital. (44 years old, divorced, unstable employment, diagnosed with HIV in 2003)
Discussion
In the context of notable enhancements in the life expectancy of people living with HIV and their growing needs for non-HIV medical care,1,2 deciding when and where to disclose one's HIV status is a difficult process in which our participants had to consider many factors. Our study contributed to the much-needed but underdeveloped literature on the disclosure of HIV status to healthcare providers, focusing on WLHA in Hanoi. We identified three patterns of HIV status disclosure, providing insights into participants’ decision-making and potential outcomes of their disclosure practices.
Selective disclosure is the predominant practice of disclosing one's HIV status to healthcare providers. People with HIV may justify this practice given the persisting stigma and discrimination in healthcare settings at a global scale.38,39 The considerations for disclosure reported in our study shared some similarities with the literature. Globally, reluctance to disclose HIV status is often driven by fear of rejection and self-blame, while motivations for disclosure include the desire to protect healthcare providers and receive better care.12,37 Our participants expressed concerns about protecting not only healthcare providers but also fellow patients, a nuance that had not been previously highlighted.
Our participants’ fear of implicit HIV-related discrimination when seeking medical services suggested people living with HIV in Vietnam might experience an imbalanced power dynamic with healthcare providers, which could lead to distressing situations where healthcare providers may choose not to admit them, unnecessarily refer them to other hospitals, and/or provide suboptimal care. On a related note, concerns about breaches of confidentiality also warrant serious consideration. In the Netherlands, the “duty of professional confidentiality” contributes to participants’ confidence in disclosing their HIV status to healthcare providers. 12 Despite the existence of the law on HIV confidentiality in Vietnam since 2006,40,41 not all participants felt assured in the discretion of healthcare providers. Participants’ mistrust of community-based healthcare settings and perceived confidentiality protection in distant, large healthcare facilities could lead to overcrowding in centralized, specialty care facilities; additionally, these factors may contribute to a lack of acceptability of community-based HIV prevention and care services.42,43 This underscores a critical need for attention in the configuration of medical settings in Vietnam, particularly in terms of enforcing confidentiality practices in rural and community-based clinics.
Besides the fear of stigma, the decision not to disclose one's HIV status to healthcare providers also often stems from a prevailing belief that such information is irrelevant to the safety of healthcare providers and the provision of care.5,12 Our research delved into the underlying criteria influencing these judgments. Participants commonly viewed procedures involving blood or bodily fluids as either posing risks to healthcare providers and fellow patients or as being critical enough to care provision to warrant disclosure. However, some participants’ judgments that dermatological and gynecological conditions were irrelevant to HIV treatment and care were not based on sound medical knowledge. 12 Without a comprehensive understanding of participants’ HIV status, healthcare providers may be unable to address potential interactions between ART medications and other drugs, or manage other HIV-related complications, posing serious risks to participants’ health.5,12 Our research underscores the significance of educating WLHA about the pros and cons of disclosing their HIV status to healthcare providers in general healthcare settings so that they can make well-informed decisions. Mock sessions to practice disclosure in healthcare settings, along with peer navigation, could be effective strategies to prepare patients for disclosure and support them when disclosing their HIV status in healthcare settings.44,45
This study offers several implications for the Vietnamese healthcare system to better support WLHA in disclosing their HIV status within healthcare settings. Firstly, leveraging the trust that patients place in HIV clinics, HIV treatment providers can serve as essential resources by offering guidance on disclosure when WLHA seek non-HIV healthcare services. These providers can also facilitate connections to non-HIV medical services that are known to be supportive and accommodating. To reduce the burden on HIV treatment providers and promote access to care, it is crucial to implement general education and training for all healthcare providers. This training should focus on improving communication skills during history-taking to effectively elicit information about HIV and other infectious diseases. Such education must address the specific needs of patients at risk of or living with HIV, including considerations for increased risks of co-occurring conditions and potential medication side effects and interactions. Promotion of the Undetectable = Untransmittable (U = U) 46 concept among general populations can play a significant role in reducing stigma, encouraging disclosure, and mobilizing support. Additionally, leadership in community-based settings should prioritize adjustments to hospital setups and enforce clinical ethics to enhance confidentiality protections. These systemic changes will help create a more supportive environment for WLHA, facilitating more open and safe disclosure of their HIV status in seeking holistic care.
The study comes with several limitations. First, the participants were recruited from Hanoi, the capital of Vietnam, which has relatively advanced medical resources. WLHA in other regions of Vietnam might have different considerations or face other challenges in HIV disclosure that were not captured in our study. Additionally, most of the WLHA in the study had some contact with healthcare systems; further research is needed to explore the disclosure practices of WLHA who are not receiving ART to better address the needs of the most disadvantaged WLHA. The study also inherently suffered from recall bias and social-desirability biases. Lastly, due to the limited sample size, we did not perform quantitative analysis to formally identify factors associated with the three identified disclosure patterns. Future research with larger sample sizes is needed to explore how WLHA's characters and service experiences are correlated with their disclosure patterns.
Conclusion
Our study illuminates the three patterns of disclosing HIV status to non-HIV healthcare providers among WLHA in Vietnam and the factors considered in their decision-making. When left unaddressed, WLHA might suffer from a lack of timely care or lower quality of care. Our findings highlight the importance of educating WLHA to make well-informed decisions and supporting them throughout the disclosure process. Furthermore, we recommend additional training for healthcare providers in history-taking skills to effectively gather information about HIV infection and other infectious diseases. It is also crucial to enforce confidentiality protection and non-discriminatory policies to eliminate the negative experiences associated with disclosure for WLHA.
Supplemental Material
sj-docx-1-jia-10.1177_23259582241277655 - Supplemental material for Disclosure of HIV Status in Healthcare Settings: Practices and Considerations among Women Living with HIV/AIDS in Vietnam
Supplemental material, sj-docx-1-jia-10.1177_23259582241277655 for Disclosure of HIV Status in Healthcare Settings: Practices and Considerations among Women Living with HIV/AIDS in Vietnam by Thu Trang Nguyen, PhD, Dang Thi Huong, MD, MSc, Lynn T. Nguyen, BA, Bich Diep Nguyen, MD, PhD, Le Minh Giang, MD, PhD, and Chunqing Lin, PhD in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-2-jia-10.1177_23259582241277655 - Supplemental material for Disclosure of HIV Status in Healthcare Settings: Practices and Considerations among Women Living with HIV/AIDS in Vietnam
Supplemental material, sj-pdf-2-jia-10.1177_23259582241277655 for Disclosure of HIV Status in Healthcare Settings: Practices and Considerations among Women Living with HIV/AIDS in Vietnam by Thu Trang Nguyen, PhD, Dang Thi Huong, MD, MSc, Lynn T. Nguyen, BA, Bich Diep Nguyen, MD, PhD, Le Minh Giang, MD, PhD, and Chunqing Lin, PhD in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
This study was funded by the Fogarty International Center (FIC) grant number R21TW012018 and the National Institute of Mental Health (NIMH) grant number P30MH058107. We thank the Outpatient clinics in Nam Tu Liem and Hoang Mai Districts of Hanoi and Vietnam Network of People Living with HIV/AIDS, Vietnam Network of Sex Workers for their efforts to recruit study participants for this study.
Author's Contribution
NTT was involved in data collection and analysis and took the lead in conceptualization and manuscript writing. DTH contributed to data collection and analysis. LTN assisted with data analysis and manuscript editing. NBD was responsible for data collection and was involved in data analysis and manuscript writing. LMG was responsible for study implementation and funding acquisition. CL was responsible for data analysis, manuscript writing, and funding acquisition. All authors reviewed and approved the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by the Institutional Review Boards at University of California, Los Angeles (IRB#21-001503) and Hanoi Medical University (TRB-VN0 l .001/IRB00003121).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Fogarty International Center (FIC) grant number R21TW012018 and the National Institute of Mental Health (NIMH) grant number P30MH058107.
National Institute of Mental Health, Fogarty International Center (grant numbers P30MH058107, R21TW012018).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.