
Abstract
Young men of color who have sex with men are vulnerable to HIV and experience poor PrEP uptake and retention. We conducted a secondary data analysis and calculated adjusted Prevalence Odds Ratios (aPORs) for PrEP retention along with 95% CIs at 90, 180, and 360 days at an organization running safety net clinics in Texas for gay and bisexual men. We found statistically significant association with age, race, in-clinic versus telehealth appointments, and having healthcare insurance. White clients had an aPOR of 1.29 [1.00, 1.67] as compared to Black clients at 90 days. Age group of 18–24 had a lower aPOR than all other age groups except 55 or older at all three time periods. Clients who met providers in person had an aPOR of 2.6 [2.14, 3.19] at 90, 2.6 [2.2, 3.30] at 180 days and 2.84 [2.27, 3.54] at 360 days. Our findings highlight the need for population-specific targeted interventions.
Plain Language Summary
Lower PrEP retention for black and young MSM in Texas
Our study findings suggest that of all clients who start PrEP, Black clients and younger clients had a higher chance of not continuing PrEP as compared to White clients and older clients respectively. This analysis was done for a clinic that pre-dominantly offers services to gay and bisexual men. We also found that those who were attending clinic in person had higher chances of continuing. Further those who are insured also had higher chances of continuing.
Keywords
Introduction
Young men of color who have sex with men (such as the Latino and African American men who have sex with men) are disproportionately impacted by HIV/AIDS in the United States.1-3 As per the National HIV Surveillance System (2018), while the incidence of HIV has declined among White MSM over years, it has remained constant for Black men having sex with men (MSM) and increased for Latino/Hispanic MSM. 4 Data from the HIV network for prevention trials vaccine preparedness study, EXPLORE behavioral efficacy trial, and VAX004 vaccine efficacy trials found that the average risk per contact for unprotected receptive anal (URA) intercourse and unprotected insertive anal intercourse (UIA) with HIV seropositive partners were higher among younger participants of the trials and among the Latino participants when compared to White participants–—indicating a higher need of PrEP for HIV prevention among these groups. 5 Minority stress (social stress faced by sexual minority populations due to their stigmatized social status relative to heterosexual populations) 6 may lead to decreased self-care, lower access to safe sex resources, and create sexual health disparities. 7 Concurrently, findings from an analysis that dominantly had young men of color who have sex with men suggested lower uptake of HIV testing among young MSM. 8
Pre-exposure prophylaxis (PrEP) is an effective biomedical HIV prevention modality.9,10 Apart from the daily oral pill, PrEP is also now available as a long-acting injectable with an injection once every two months, administered by a provider.11-13 While young men of color who have sex with men bear the disproportionate burden of HIV and are more vulnerable to HIV, studies suggest that the uptake of PrEP among this group has remained lower than White MSM.14-17 Furthermore, lower PrEP awareness has been found to be associated with perceived healthcare discrimination for men of color who have sex with men. 18
An analysis of the HIV-negative individuals from the Observational Pharmaco-Epidemiology Research & Analysis (OPERA) cohort suggested that among 14598 individuals who were prescribed PrEP, those of non-Black race, older individuals, nonintravenous (IV) drug users, and those with commercial insurance were overrepresented in the cohort. 19 Another analysis of the AIDSVu 20 dataset found that the PrEP-to-need ratio (PrEP prescriptions divided by HIV diagnoses in the county) had negative correlations with percent African American and percent uninsured. 21
Furthermore, young men of color who have sex with men report several other barriers to PrEP uptake such as low perception of risk, burden of daily dosing, perceived side effects, and stigma of using PrEP. 22 Even if young men of color who have sex with men start PrEP, studies suggest that they are prone to poor persistence or retention.23,24
There is an overall paucity of research that brings forth disparities in PrEP retention with respect to such minority groups. Clinics and healthcare sites offering PrEP need to dive deeper into these issues to understand the inequities and get more attuned to the needs of young men of color who have sex with men to facilitate PrEP uptake/retention and contribute towards the goals outlined in the Ending the HIV Epidemic initiative in the United States. 25 Center for Health Empowerment (CHE) is a group of clinics operating in Austin and Dallas (Texas) that offers HIV testing, daily oral PrEP, STI testing, and antiretroviral treatment. 26 For the time-period of this analysis, the organization was running one clinic in Austin, two clinics in Dallas, and a centrally run Telehealth clinic. The organization is a safety net clinic for gay and bisexual men, offering community friendly services to all—irrespective of their insurance status. While there is a focus on gay and bisexual men, the clinic offers services to all those who seek them at the clinic. The clinic uses a pay-forward model where revenue generated from paying clients is used to pay for clients who are uninsured or not covered by other payment assistance programs). The aim of this study is to conduct a secondary data analysis and explore potential inequities with PrEP retention, identifying vulnerable groups who are dropping out of prevention care. Findings of this study will help guide the development of population-specific interventions that could improve PrEP retention.
Methods
Study Settings
We included all clients who completed a PrEP appointment and had a prescription written from the period starting 1 September 2016 until 31 April 2023 so that 360 day retention could be accurately calculated. Clients receiving their first PrEP prescription after 31 April may not require a prescription for 360 days yet and would create bias. We did not add additional days to 90, 180, and 360 as a window or buffer since we already included medication lag in the total days in care. If any values were missing for independent variables (such as race or ethnicity), those were described as not specified and included in the study population. We extracted data for clients accessing services at CHE—a 340b covered organization that was running one sexual health clinic in Austin, two in Dallas and across Texas through telehealth, during the period for which this analysis was done. The data were extracted from 340bwell software—used along with the Electronic Medical Record (EMR) system by the clinic to streamline client navigation. The 340bwell software imports data from EMRs and contract pharmacies (those pharmacies that are 340b eligible 27 and work with the clinic) and collate them together for clinic staff to supervise PrEP navigation and client needs.
A data extraction template was provided to the clinic team, and they used Sequential Query Language (SQL) to query the database of 340bwell and extract required variables in excel format. Based on our discussion with the clinic, the excluded group would include clients who showed interest but did not schedule an appointment, or scheduled an appointment but did not complete it, or completed an appointment but did not get a prescription. The excel file given by the clinic team was imported in Stata (provided by the University of North Carolina Chapel Hill's Virtual Lab). 28
Dependent Variables
The primary outcome of our study was PrEP retention among the clients at 90 days (3 months), 180 days (6 months), and 360 days (1 year). The periods were chosen after scanning the literature and finding similar studies that examined PrEP retention in United States.29-31 Secondary outcome included PrEP discontinuations that are described ahead.
We used the prescription date, quantity, and refill to calculate the number of days for which the client would have medication—using prescription data is consistent with other studies in the literature that analyze PrEP retention.32-35 The limitation of this approach is included in the discussion section. The providers at the clinic wrote prescriptions with varied numbers of quantities (range = 7–90) and refills (range = 0–6). Hence, it was not feasible to simply look for a prescription in a specific period or after a specific period. Hence, to understand retention and possible discontinuation, we described the following parameters:
Quantity: Quantity of one fill in the prescription;
Number of refills: Number of refills for that prescription;
Gap between prescriptions: Number of days of gaps between two consecutive prescriptions;
Prescription coverage: Number of days covered by a prescription; calculated as [quantity] × [1 + refills];
Medication lag: [gap between prescriptions] − [preceding prescription coverage];
Total number of days in care: Σ prescription coverage i + Σ medication lag j (for all medication lag > 0), where i = 1, 2, 3, 4 … 12; j = 1, 2, 3 … 11;
Retained in care: If total number of days in care > 90, 180, and 360;
Discontinuation: If medication lag > 14.
Figure 1 shows these parameters and provides a visual representation of how they are calculated.
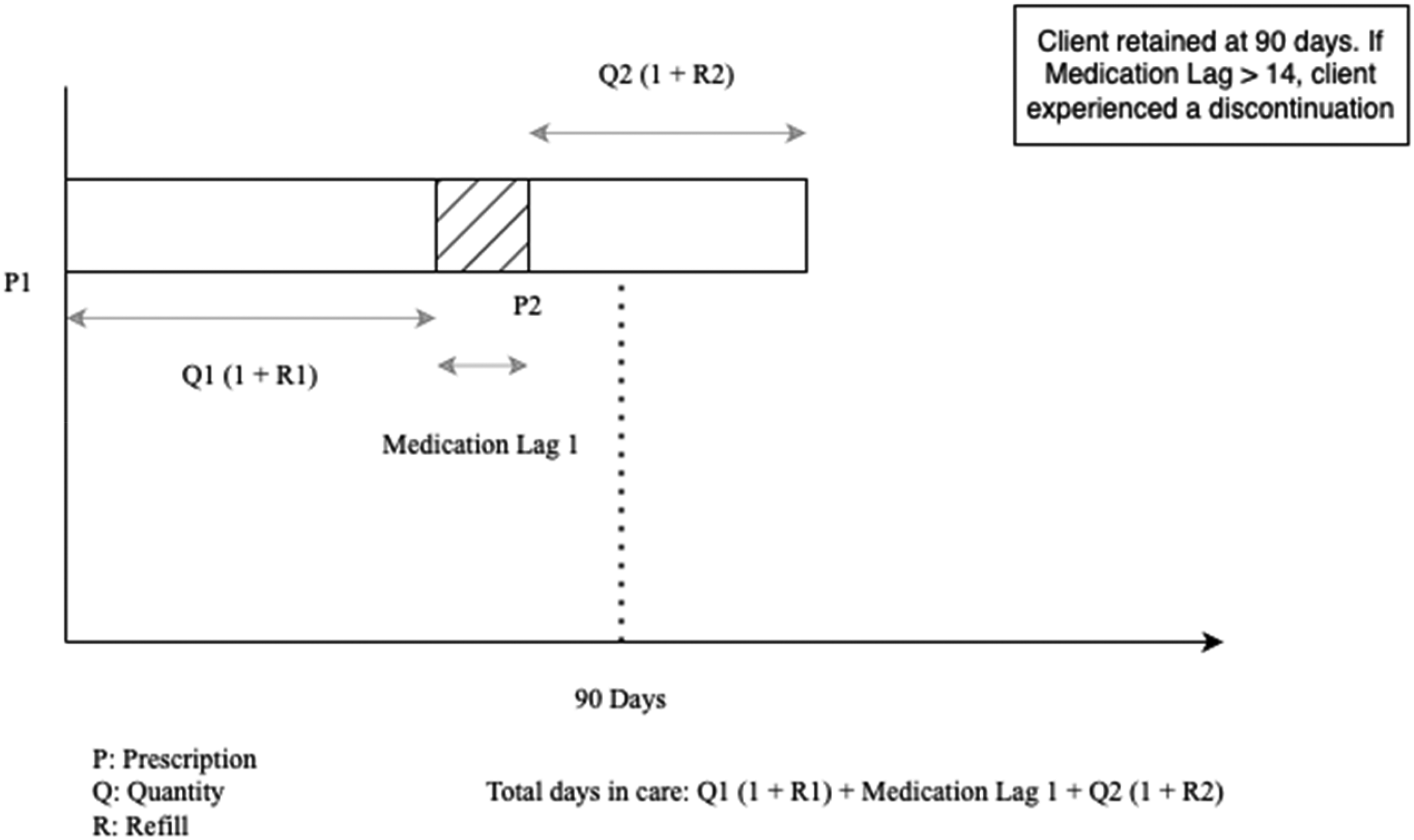
Calculation of the total number of days in care using prescription quantity and refill data.
Hence, a client was considered retained at a specific time period if the number of days in care was more than that given time period (90, 180, and 360 days). Discontinuation was defined as having a medication lag > 14 days but having a future prescription written. The 14 days cutoff was based on pharmacodynamic data that indicated that protection from HIV was low by 14 days after the last dose of PrEP. 36 This is consistent with another study that studied discontinuation among Black MSM in Atlanta (Georgia). 37
Independent Variables
Independent variables included race, ethnicity, age group, appointment type (telehealth vs in-clinic) and insurance at the first prescription.
We used Directed Acyclic Graphs (DAGs) to select covariates. 38 Insurance and zip code were identified as mediators for race and ethnicity. Insurance alone was selected as a mediator for the age group. Zip code was selected as a confounder for clinic. Age was selected as a confounder for telehealth. Race, ethnicity, and age group were identified as confounders for insurance.
Data Analysis
To reduce bias, we excluded those clients who had any two consecutive prescriptions written within 15 days (about 2 weeks), because as per clinic, those could be clients who may have requested a change in medication and hence had a new prescription. We then calculated retention at defined periods, along with discontinuations for those retained at the three time periods described. We created frequency tables for retention at 90, 180, and 360 days and other independent variables and then calculated prevalence odds ratio and adjusted prevalence odds ratios along with 95% confidence intervals using multivariate logistic regression We did not conduct a sensitivity analysis.
Ethical Approval and Informed Consent
The study was approved by UNC Chapel Hill IRB (IRB Number 23-1655) and informed consent was approved to be exempted by the IRB.
Results
Participant Characteristics
The final study population had 1704 entries. The study population was predominantly MSM with 56% (n = 961) self-reported gay and 16% (n = 271) bisexual. At the same time, the study population also had 12% heterosexual individuals (n = 208). Our study population consisted of 79% (n = 1350) cis-gender males; concurrently, a little more 10% of the clients were cis-gender females (n = 178). The remaining 176 individuals consisted majorly of those who did not specify their gender (n = 102) along with transwomen (n = 14) and genderqueer (n = 23). There were 42% (n = 721) White individuals, 25% (n = 419) Black individuals along with 17% (n = 299) identifying as Native American, Native Hawaiian, or other races. There were 11% (n = 195) clients who did not specify their race. Age group 25–34 was the largest age group in our study population with 45% (n = 772) individuals followed by 35–44 at 15% (n = 426). Both 18–24 and 45–54 were close to 11%. For ethnicity, 42% (n = 722) clients identified as non-Hispanic, 15% (n = 251) as Hispanic, and 43% (n = 731) did not specify their ethnicity. A total of 56% (n = 955) used telehealth modality and 16% (n = 281) clients were insured at the date the first prescription was written.
PrEP Retention, Discontinuation and Statistical Analysis
Table 1 illustrates retention at the defined time periods along with prevalence odds ratios (POR) and adjusted prevalence odds ratio (aPOR) with 95% confidence intervals (CIs). Overall retention dropped from 50% (n = 856) at 90 days (3 months) to 40% (n = 684) at 180 days (6 months) and 27% (n = 477) at 360 days (1 year). For all clients retained at 90 days, 70% (n = 603) of the clients experienced at least one discontinuation. For 180 days (about 6 months) and 360 days (about 12 months), this was 78% (n = 538) and 85% (n = 406).
PrEP retention, prevalence odds ratios, adjusted prevalence odds ratios, and 95% confidence intervals.
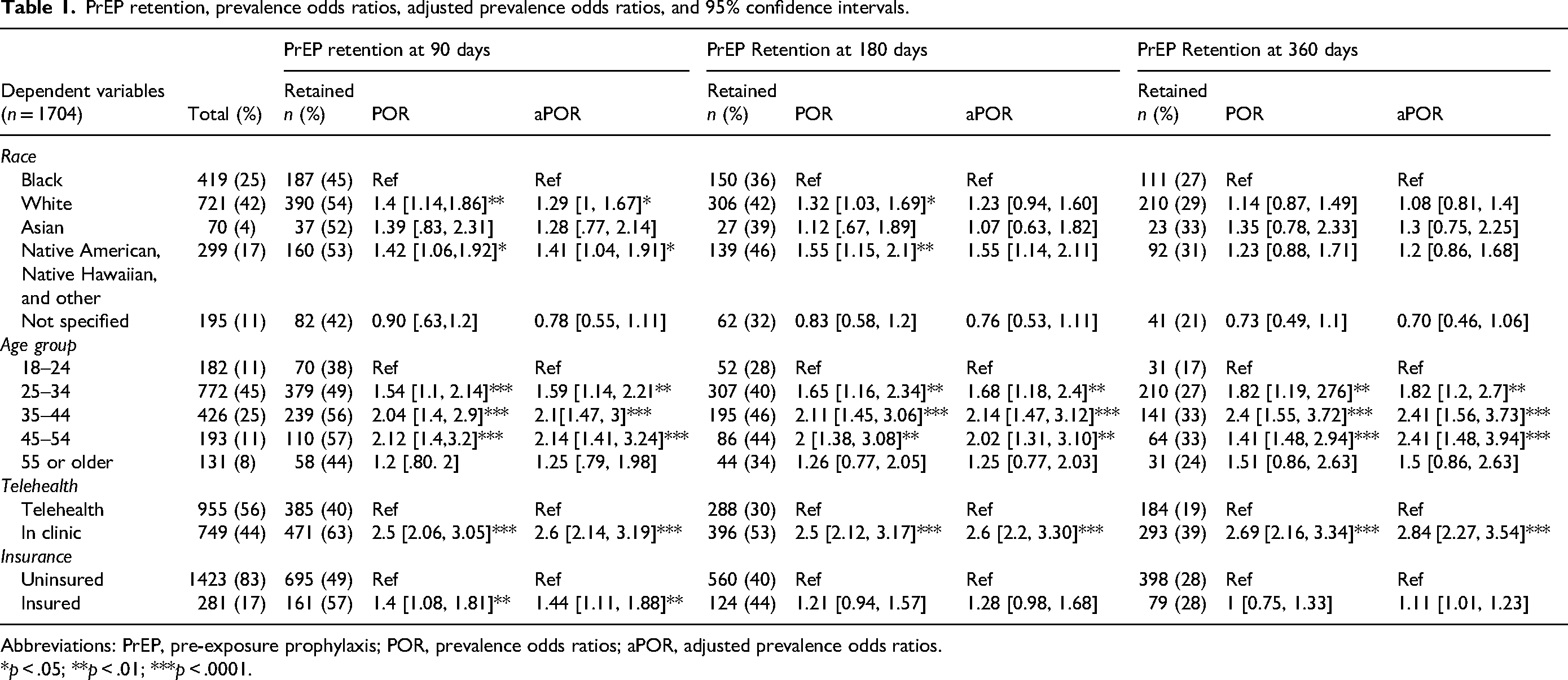
Abbreviations: PrEP, pre-exposure prophylaxis; POR, prevalence odds ratios; aPOR, adjusted prevalence odds ratios.
*p < .05; **p < .01; ***p < .0001.
At 90 days, we found that White clients were more likely to be retained with an adjusted prevalence odds ratio (aPOR) and 95% confidence interval of 1.29 [1, 1.67] as compared to Black clients. All age groups except 55 or older had an aPOR>1 as compared to the 18–24 age group. Those in the age group 25–34 had an aPOR of 1.59 [1.14, 2.21]; those in the age group 35–44 had an aPOR of 2.1 [1.47, 3] and those in the age group 45–54 had an aPOR of 1.25 [1.41, 3.24]. Clients having in-person appointments had an aPOR of 2.6 [2.14, 3.19] as compared to telehealth clients and those who had insurance at first prescription had an aPOR of 1.44 [1.11, 1.88] as compared to those with no insurance at the first prescription.
At 180 days, we did not find aPOR that were statistically significant for race and for age groups as well; we found that the age group 25–34 had an aPOR of 1.68 [1.18, 2.4]; those in the age group 35–44 had an aPOR of 2.14 [1.47, 3.3] and those in the age group 45–54 had an aPOR of 2.03 [1.21, 3.1]. In-clinic clients had a POR of 2.6 [2.2, 3.3] as compared to telehealth clients. At 360 days, we found a similar pattern with the age group 25–34 (aPOR 1.82 [1.2, 2.7]), age group 35–44 (aPOR 2.41 [1.56, 3.73]), age group 45–54 (aPOR [2.41 [1.48, 3.94]), and in-clinic clients (aPOR 2.84 [2.27, 3.54]). We did not conduct multivariate regression for Ethnicity because of the large number of missing records for self-reported ethnicity.
We further conducted a sub-analysis of the 18–24 age group and examined aPOR for the race in this age group. However, we did not find any statistical significance for any retention periods.
Discussion
Our study findings uncover that young people and Black people had poorer PrEP retention as compared to most of the other older age groups and those who self-reported race as White, respectively. Furthermore, those who had in-clinic appointments had greater retention as compared to those who sought telehealth appointments, and insured clients had better retention than uninsured clients. Retention in our study was lower than another study in Texas that also looked at prescription data for retention in El Paso and reported retention to be at 82.5% and 54% at 90 days and 180 days. 29 However, the study population in this study was predominantly Hispanic. We did not find any other studies that measured PrEP retention in Texas. However, in the neighboring state of Louisiana's New Orleans, another study reported retention at 48% at either 3 or 6 months. 39 In Jackson, Mississippi, a study reported 18% of clients attending their first clinical follow up within 105 days of first prescription pick up in a pharmacy led program—which is a lot lower than our own findings. 40 The way other studies measure retention and the study settings may influence the scale of such measures and must be interpreted accordingly.
Our findings reveal that the 18–24 age group was most vulnerable to not being retained for all three time periods. This underscores the need of urgent PrEP retention interventions focused on young people. Another study that conducted a secondary data analysis for PrEP at the Planned Parenthood League of Massachusetts found results similar to our study with older clients having higher number of mean PrEP prescriptions. 41 A cross-sectional study in San Francisco also had similar results with those who self-reported as White and older were more likely to be on PrEP. 17
Similar to our study, several other studies in the literature discuss prevalent racial disparities with respect to PrEP use among the MSM communities.42-45 Those at the cross-section of these vulnerable identities around age and race, may experience further disparities and inequities18,46—however, we did not find statistical significance for such groups in our analysis.
We found higher retention among those clients who were attending clinic in person as compared to telehealth clients. This is particularly interesting since it is anticipated that telehealth would overcome barriers to access to PrEP and studies have usually found telehealth to be acceptable among those who are using PrEP or would benefit from it.47-49 Our findings re-instate the importance of in-person engagement and the role it can play in keeping clients retained.
We found that insured clients were more likely to be retained at 90 days. A survey among young MSM corroborates our findings of having healthcare insurance correlated with higher PrEP use. 50 Another study conducted in St Louis, Jackson, and Providence found that insured patients were four times as likely to use PrEP services. 51 The literature illustrates several other studies across United States that reveal similar observations around correlation between lack of insurance and PrEP use.52-54
Our study has some limitations; since we do a cross-sectional analysis of secondary data, we cannot establish causality. Furthermore, our study does not uncover the reasons for these interruptions and some of those interruptions could be planned interruptions for reasons such as entering a monogamous relationship. 55 At the same time, some clients may have moved out of state (and hence not eligible to receive care at this clinic) or have switched to another clinic—hence, they would still have been retained, just not at this clinic. Not knowing the status of those who were not retained at this clinic and using prescription data where there could be clients who obtained a prescription but did not fill it or use PrEP, may have an influence on the accuracy of our measures. Also, we consider insurance at the date of first prescription—however, insurance status may change over time. However, these limitations do not underplay the relevance of the findings of our study that characterize PrEP related inequities even at a safe-haven clinic for the community in Texas.
Our findings bring forth prevalent inequities with PrEP use that clearly illustrate the need of population specific interventions to improve PrEP retention for vulnerable communities. Studies show that designing interventions that are based on recommendations by the clients are more acceptable and satisfactory. Interventions that leverage technology, use social/sexual networking applications, or leverage enhanced patient navigation are also some of the promising avenues that should be explored.55-58 Furthermore, clinics providing HIV/AIDS related services should consider collecting additional data to understand the social determinants of health (such as education, income, housing stability, and more) better.59,60 Interventions that consider the social, structural, behavioral factors, and their interplay are likely to be effective in retaining clients. 61
Conclusion
Young and Black gay and bisexual men experience worse PrEP retention outcomes as compared to individuals belonging to older age groups and racial groups, respectively. There is an urgent need to explore key barriers to PrEP retention among these groups and implement population specific and culturally competent evidence-based PrEP retention interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.