
Abstract
The study explores barriers and suggestions for improving viral load testing (VLT) uptake in Tanzania, revealing that only 58% of patients receive VLT annually, contrary to the Tanzanian National Guidelines toward the 95-95-95 UNAIDS targets. Twelve individual interviews and three patient-focus groups were conducted as part of a qualitative study conducted in six human immunodeficiency virus (HIV) clinics in Dar es Salaam to identify potential suggestions for access enhancement, as well as barriers to VLT uptake. Using King’s theory of goal attainment, we found that missing appointments was the primary individual barrier to VLT uptake, along with limited knowledge among individuals living with HIV. Participants also face system–level barriers, such as a lack of integrated care and evening service availability. The study suggests that, despite challenges, there is potential for improvement in the uptake and quality of VLT services in Tanzanian public health facilities through a holistic approach.
Plain Language Summary
The study investigates barriers and potential suggestions to improve viral load testing (VLT) uptake in Tanzania, highlighting that only 58% of patients receive VLT annually, contrary to the Tanzanian national guidelines. A qualitative study in six HIV clinics in Dar es Salaam involved 12 in-depth interviews and three patient-focused group discussions to identify facilitators and barriers to VLT uptake, using King's goal attainment theory. Missing appointments is the main barrier to VLT uptake, attributed to distance from care and high transport costs. Healthcare providers and patients also face systemic and structural barriers, such as a lack of integrated care and evening service availability. Patients suggest effective communication, service extension, and knowledge sharing to improve VLT uptake. The study suggests that, despite challenges, there is potential for improvement in the uptake and quality of VLT services in Tanzanian public health facilities through a holistic approach.
Introduction
Viral load (VL) suppression is critical in achieving both reduction in mortality and morbidity as well as reducing human immuno-deficient virus (HIV) transmission. VL suppression of at least 95% is the third target of the 95-95-95 UNAIDS targets to eliminate the HIV/AIDS epidemic by 2030. 1 VLT is needed for appropriate monitoring of effectiveness of antiretroviral therapy (ART) as well as on time diagnosis and management of treatment failure. 2 Tanzania guidelines follow the WHO recommendations of doing VLT of all patients in care at 6 months after ART initiation, followed by another test at 12 and then at yearly. 3 The country scaled up the HIV viral load testing (VLT) in 2016 by establishing tertiary level (zonal and regional) laboratory capacity and invested on the chain of specimen transportation from respective tertiary level (zonal) facilities. 4 According to the recent data, in Tanzania, the adult HIV prevalence is 4.4% (with women having a higher prevalence of 5.6% compared to men's 3.0%), meaning that about 1,548,000 aged 15 years and above are living with HIV. 5 Tanzania HIV Impact Survey (THIS) data of 2022–2023 reports that, the country has 82.7% PLWH aged 15 years and above who know their HIV status, 97.9% of all people aged 15 years and above diagnosed with HIV are on ART, and 94.3% of all people aged 15 years and above on ART have achieved viral load suppression. 5 Regardless of the impressive achievements made toward UNAIDS goals on viral suppression, the number of PLHV on ART who receive VLT is still low in Tanzania. In one of the published reports, less than 40% of patients in care received VLT in 2018. 4 In a later study which was conducted in 2021, over half (57.6%) of participants had at least one VLT in the past 12-month period. 6 The rates of VLT in most sub-Saharan countries are similarly low, and it is estimated that, in both low- and middle-income countries (LMICs), only 50–60% of HIV patients can access VLT. However, some countries, including Uganda, have reported higher rates of up to 80%.7–9
System-level challenges of VLT in sub-Saharan countries have been widely reported including frequent inefficient specimen transportation, lack of knowledge among laboratory workers, reagent procurement delays and poor financial status to support the HIV-VLT scale-up.2,10,11 Furthermore, long turnaround time from specimen collection to results return at the clinic which threatens timely clinical decisions. Shortage of well-trained laboratory staff and difficulty in specimen transportation to the testing laboratory have been reported, and all these pose a threat for eligible patients in care to access the test and results. 10 Other challenges on the supply side include, lack of awareness among clinicians on the importance of ordering and testing for patient's viral load as it helps treatment monitoring to enhance long life to PLHV. 2
The perspectives of patients and the experiences of providers on the VLT services are not well documented. Gaining insight into their perspective will enhance compliance with the VLT guidelines for all eligible HIV patients receiving care, allowing for the monitoring of treatment efficacy and have an appropriate treatment for those with treatment failure. We therefore conducted a cross-sectional qualitative study involving patients and healthcare providers to share their perspectives on the potential suggestions to improve VLT uptake and barriers on VLT services in Dar-es-salaam. What we found is important in understanding the existing gaps including the patient's and care providers’ viewpoints on individual, and system-level-related barriers and suggestions for supporting quality improvement (QI) in order to improve adherence to VLT which is critical toward achieving the third UNAIDS HIV targets by 2030. The results of this study may also assist policy makers, implementers, and other interested parties in reevaluating their strategies to meet the patient-centered interests and achieve the respective community health outcomes.
Health Care System in Tanzania
The structure of the health care referral system is a pyramid. The community is at the base of the pyramid, with district level hospitals, health centers, and dispensaries making up the primary health care sector. Regional referral hospitals come next (secondary level healthcare facilities), and they are followed by tertiary level facilities which include zonal hospitals, specialized hospitals, and lastly the National Hospital.12–14 Since gaining independence from Britain in 1961, Tanzania has worked very hard to guarantee that all its citizens have fair access to high-quality fundamental social services, including health. By 2007, 64% of healthcare delivery was provided by government health services but there is progressive improvement in increasing the number of health facilities and services throughout the country. 15 Despite such development in the public sector, still in actuality, achievement of universal health coverage has been a policy concerns because of the coverage of the public health facilities. To cover the gap, there is a strong establishment of the public–private partnership which is a key feature of both Tanzania's policy approaches to health sector reform and international initiatives in the health sector in the country. 16 Despite the health care systems operating horizontally, several vertical programs have been established with the aim of improving quality and access to health care services. The HIV/AIDS programs operate vertically with the aim of improving treatment and care services to people living with HIV (PLHIV) and AIDS.17,18 The distribution of the services covers both public and private health facilities to ensure easy access to care under a special arrangement termed as Anti-Retroviral Therapy Clinic (ART). The clinic provides a range of services including health education and counseling, investigation, diagnosis and treatment, and clients are followed up for monitoring purposes include viral load suppression, CD4 counts, opportunistic infections, etc.1,9,19
Materials and Methods
Study Setting and Design
The qualitative study was conducted between November 2021 and March 2022 in HIV clinics in Dar es Salaam, Tanzania. The study was conducted and reported in accordance with the COREQ guideline of writing qualitative research. 20 Six facilities were randomly selected from a list of all 225 healthcare facilities with at least 1000 HIV patients/year to represent the five districts of the Dar es Salaam city. 21 The selected health facilities were stratified in three levels: the hospital level, health centers, and dispensary levels. From each stratum, two facilities were randomly selected using a randomly selection table. 22
Study Population and Recruitment Procedure
Patients
For the FGDs, we invited 8–12 adult PLHV in each group who had been in care for at least a year. They were conveniently approached by the research staff and invited to the discussion after receiving their health care services in the clinics. Informed consent was obtained for each participant by reading the ethical-approved participants information sheet, responding to their questions and after ensuring that, an individual participant understood everything regarding the study prior participation. The selection of patients to each of the discussion groups maintained a 1:2 male/female to represent the sex distribution of the HIV population in Tanzania. None of the approached patients or care providers refused to participate in the study. CTC in-charges gave support in the recruitment of the patients and other healthcare providers.
Healthcare Workers
The individual interviews (IDIs) included consented healthcare providers (HCPs) (clinicians or nurses) who had been trained and were involved in HIV care for more than six months in either care and treatment centers (CTCs) administration, ordering the test, collecting blood sample for the test, or share the viral load results to the patients. We intentionally targeted these participants due to their high interaction with patients during VLT or in administration and had experience in managing VLT and other HIV-related care services.
Data Collection
Interview Guides and Data Collection
The interviews and focused group discussions (FGDs) guides were grounded on King's theory of goal attainment.23–25 According to King's, in order to interact with a patient and agree to achieve their goals, healthcare providers must take the initiative, establish goals with the patient, and use an efficient chain of communication. The approach emphasizes how perception, expectations, and communication are crucial for both the patient and the practitioner to reach a desired result.23–25 These assumptions were key in the development of the data collection guides. To share their experience, we recruited healthcare workers who have been working in HIV care for at least 6 months and have been ordering the test, taking sample and, or share the viral load results to the patients, and were willing to give consent. Interviews with participants collected information on broad areas which include the following: (1) Factors on adherence to VLT guideline, (2) models for healthcare services delivery, (3) the experiences of the healthcare providers on patient's factors on accessing VLT, (4) availability of resources for VLT (such as human resources, and waiting time), (5) the healthcare provider–patient–communication, (6) knowledge sharing, and (7) reflection on the feedback of VLT and return of results. The FGDs were composed of adults PLWHV aged 18 years and above, active in care for at least 12 months on the day of interview, and willing to consent. Patient FGDs explored the barriers and potential suggestions in seeking and obtaining VLT as well as receiving the results including aspects of knowledge, attitude toward VLT and its importance, communication, satisfaction with the VLT services, how easy to access VLT, interpersonal relationship, health education on VLT, etc. Both IDI and FGD guides were pilot tested, corrected for clarity before actual data collection.
Both the interviews and FGDs took approximately 30–45 min and were conducted by PMK, a physician and ZAK a social scientist (research assistant) while EHS trained in qualitative methods and took the advisory role throughout the process. All interviews and FGDs were moderated in Swahili language and audio recorded. They were clinic based, conducted in a room or open space with limited interactions with non-participants to ensure freedom of expression and clear audio recording. Interviews continued until saturation point was reached. We defined saturation as having happened when the subsequent interviewees are no longer providing new information. This approach was essential to ensure that we did not miss any barriers or potential suggestions for improving VLT. No reimbursement or any other financial support was given to the participants because we had invited them to the clinic where they were receiving their routine HIV care. The notes captured during the interviews were shared during debriefing session with the research team to ensure that the interviews, and FGDs did not end prematurely. Due to limited project timeline, we did not return the transcripts to participants for comment and/or correction, however; we frequently listened to the audio carefully to confirm the correctness of the transcripts before translation.
Data Management and Analysis
With guidance from EHS, PMK, and ZAK read all the transcripts and listened to the audio carefully to confirm the correctness of the materials. Transcription of the audio recordings for the interviews and FGDs was done verbatim and was later translated into English. An initial code books for interviews and FGDs were developed based on King's theory of goal attainment where, the patient–healthcare provider interactions and communication during services served as a backbone for the preliminary codes.23–25 We then used deductive and inductive thematic analysis to analyze the transcripts and identify any new emerging themes. All individuals’ identifiers were removed from the transcripts to maintain anonymity of the study participants. Using four interviews as a trial, PMK and ZAK independently conducted coding to identify information that covered our predetermined themes from King's theory of goal attainment and the findings were categorized into individual and health systems factors (see the findings section). The same approach was used for the FGDs, with independently coding a one facility FGD transcript. All the coded data was reviewed by the whole team and consensus was reached by refining the codebook before embarking into the detailed coding for the rest of the remaining transcripts. Excel sheet was used to assist in coding, alignments of the participants information, and analysis of data.
Results
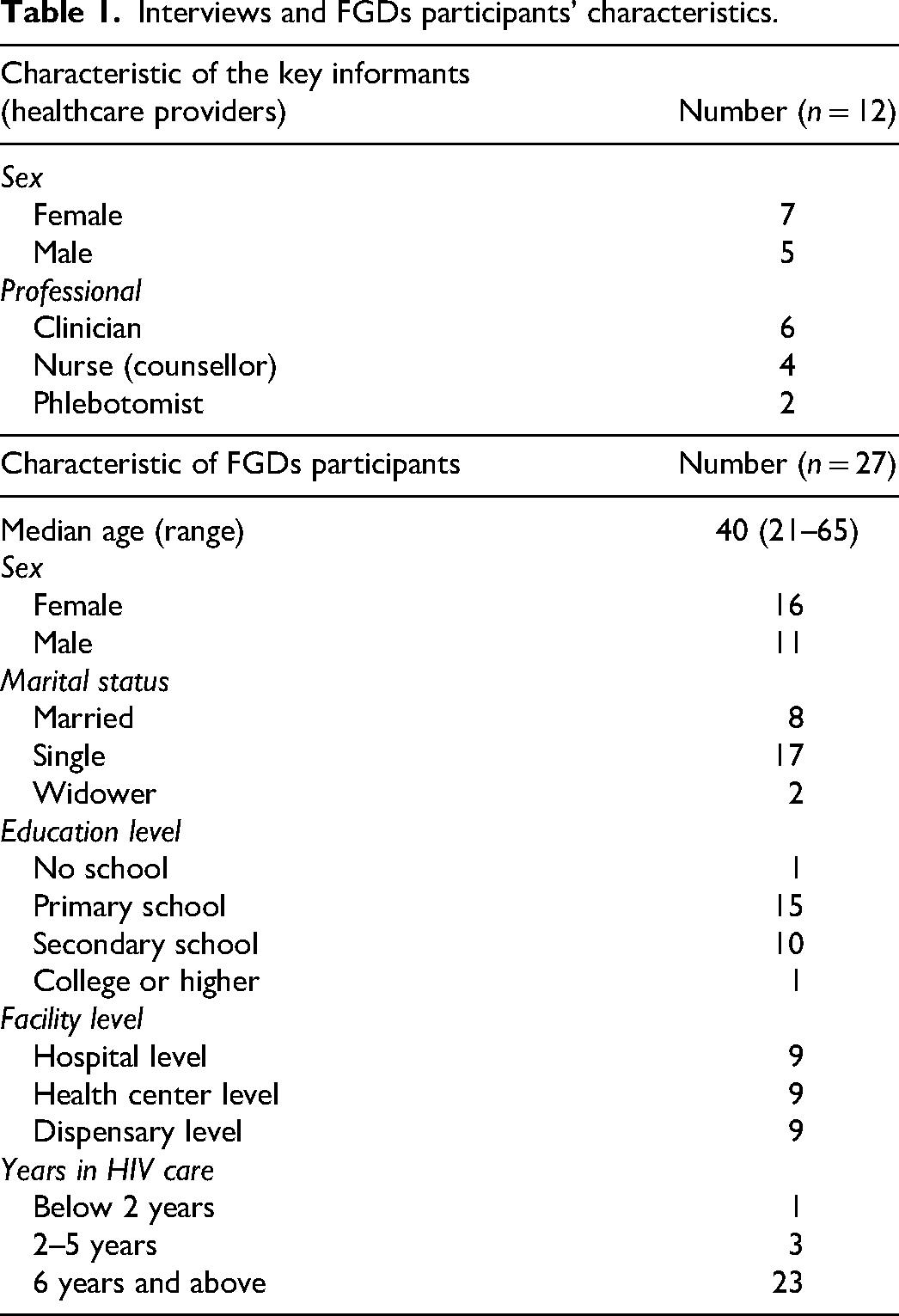
A total of 12 interviews with care providers were conducted of whom seven were females and five were males. These participants were both administrative members of the facility and/or directly dealing with VLT services of whom six were clinicians. In addition, three FGDs with patients were conducted with a total of 27 participants whose median age was 40 years. Majority were females (16) and single (17). We collected marital status information because they could have a different experience of access to care in terms of social economic factors and potential support in adherence to treatment including VLT. Educational-wise, 15 had completed a primary school level (Table 1). About three quarters of patients had been in HIV care for more than 5 years.
Interviews and FGDs participants’ characteristics.
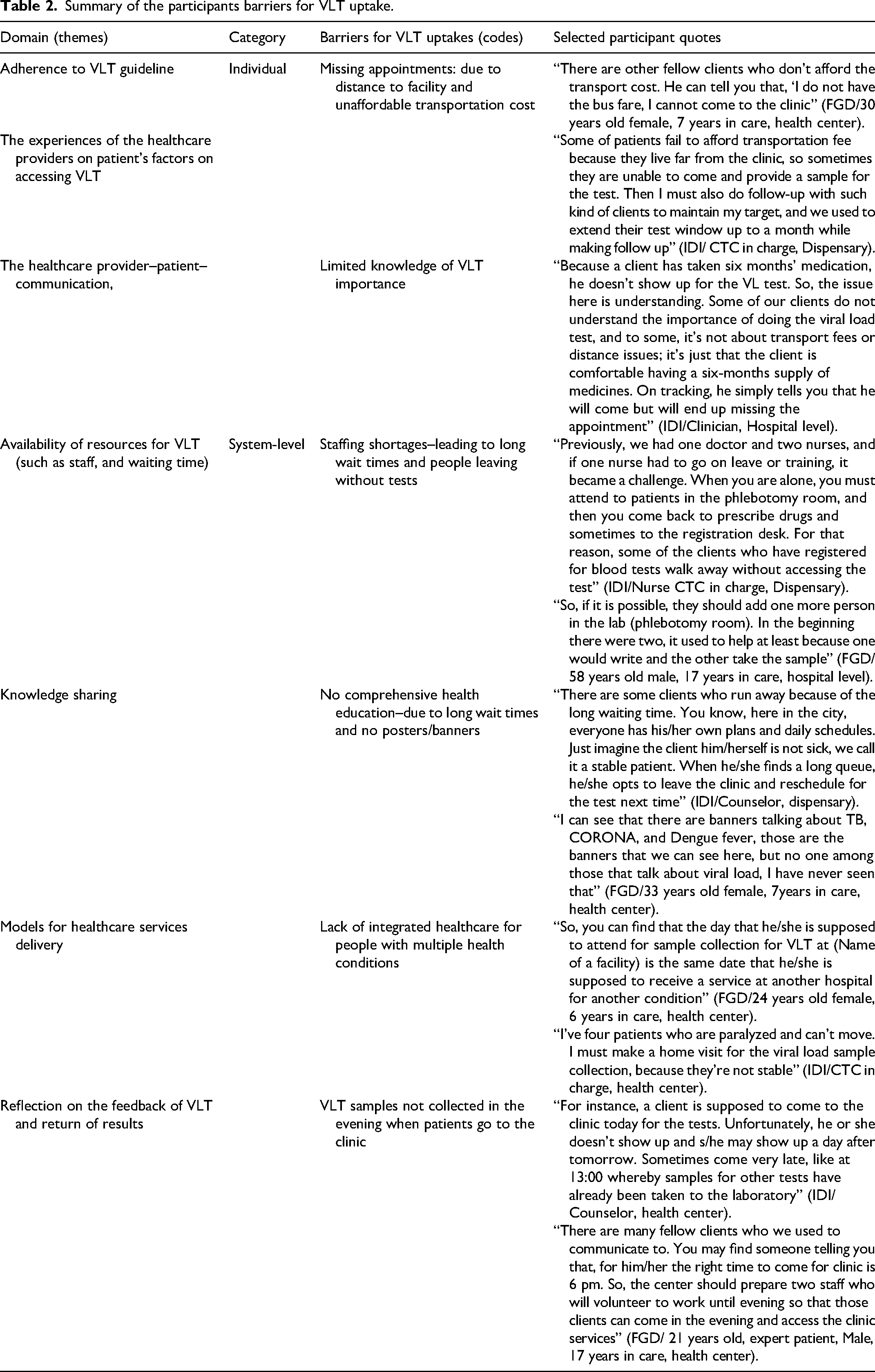
The study findings have revealed multiple factors influencing the uptake of the VLT. Reflecting on the broader area of King’s theory perception, expectations, and communications) two major categories of factors have emerged (individual and health systems) as summarized in Tables 2 and 3 with their associated quotations.
Summary of the participants barriers for VLT uptake.
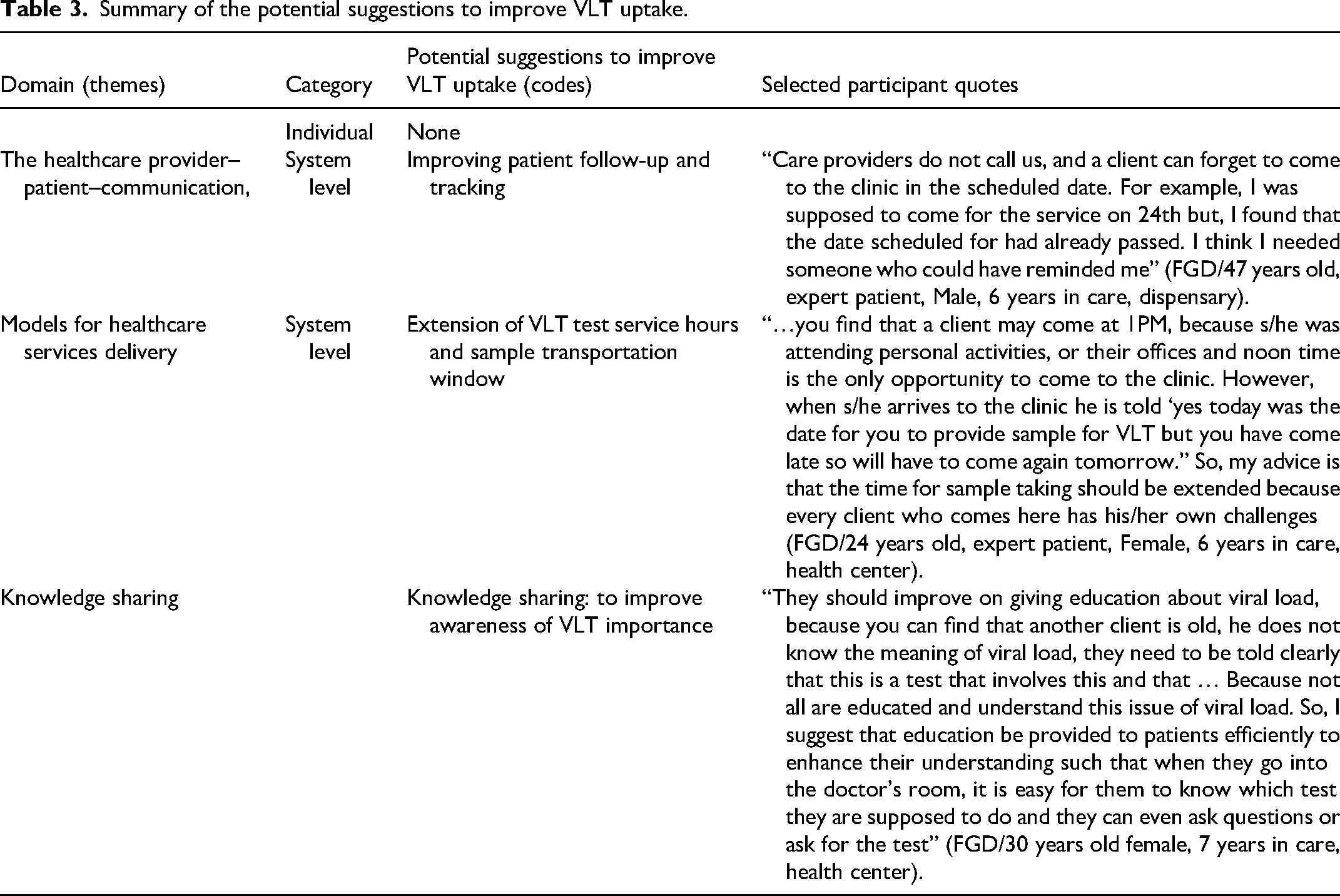
Summary of the potential suggestions to improve VLT uptake.
Barriers of VL Testing
While examining the barriers for VL test uptakes, five themes were identified and grouped into system-level and individual barriers. The individual barriers included missing appointment due to several reasons such as distance, unaffordable transport fee, and lack of knowledge among patients (Figure 1). The system-level barriers included shortage of staff, lack of integrated healthcare services, inadequate health education and narrow window for sample collection for VLT (Figure 2).
Individual barriers to VLT.

System-level barriers to VLT.
Individual Barriers
Missing Appointment
Missing appointments were widely reported by the patients during FGDs. The reasons were living far from the facility and failing to afford the transport costs. There are other fellow clients who don’t afford the transport cost. He can tell you that, ‘I do not have the bus fare, I cannot come to the clinic. (FGD/30 years old female, 7 years in care, health center)
The cost of transportation as a barrier to VLT was also confirmed by healthcare providers as some patients were said to live far away from the clinic. The CTC in-charge from the dispensary level said that distance was a hinderance factor for timely sample collection which necessitated close follow-up of patients to reach the targets. The appointment extension was said to be for up to a month or more. Some patients fail to afford transportation fees because they live far from the clinic, so sometimes they are unable to come and provide a sample for the test. Then I must also do follow-up with such kind of clients to maintain my target, and we used to extend their test window up to a month while making follow up. (Interview/CTC in charge, Dispensary)
Furthermore, healthcare providers declared missing appointments as a great challenge due to low turnup of patients in their respective VLT clinic schedules. You know, today I have 30 patients who need to be tested for viral load but you wonder they come only seven. This is a challenge. (Interview/HIV chancellor, Health Center)
Little Awareness on the Importance of VLT
As they continued sharing their experience and perspectives, healthcare providers also claimed that stable HIV patients who have with a six-month supply of ARVs find themselves missing their appointments which could partly be due to a lack of knowledge about the importance of the VLT. Because a client has taken six months medication, he doesn’t show up for the VL test. So, the issue here is understanding. Some of our clients do not understand the importance of doing the viral load test, and to some, it's not about transport fees or distance issues; it's just that the client is comfortable having a six-months supply of medicines. On tracking, he simply tells you that he will come but will end up missing the appointment. (Interview/Clinician, Hospital level)
System-Level Barriers
Shortage of Staff
Both healthcare providers during interviews and the patients during FGDs reported to experience long waiting time for HIV services including VLT at the clinic. The reason is frequently reported to be shortage of staff in public health facilities. Previously, we had one doctor and two nurses, and if one nurse had to go on leave or training, it became a challenge. When you are alone, you have to attend to patients in the phlebotomy room, and then you come back to prescribe drugs and sometimes to the registration desk. For that reason, some of the clients who have registered for blood tests walk away without accessing the test. (Interview/Nurse CTC in charge, Dispensary)
Patients had same reflection on the shortage of staff, and they thought that it should be addressed to improve VLT services as the quote below. So, if it is possible, they should add one more person in the lab (phlebotomy room). In the beginning there were two, it used to help at least because one would write and the other take the sample. (FGD/58 years old male, 17 years in care, hospital level)
Shortage of staff was said to contribute to long waiting times which discouraged patients to go for VLT. Healthcare providers acknowledged seeing some of patients who had visited the clinic for the VLT but ended up not performing the test even after the lab request form for sample collection had been completed. Sometimes the client comes to the facility for the test, and the clinician will fill the form. But if the patient is in a hurry, he can go to get other services faster, and leave the facility with the form without passing through this room for viral load sample collection. (Interview/Phlebotomist, Hospital)
Inadequate Time and Resources for Health Education on VLT
Patients reported to have been provided with little health education during consultation and there were no other sources of information to familiarize themselves with the VLT. In contrast healthcare providers complained that due to patient overload at the clinic those required for VLT were not ready to stay longer at the clinics for them to be provided with the services they require including comprehensive health education. There are some clients who run away because of the long waiting time. You know, here in the city, everyone has his/her own plans and daily schedules. Just imagine the client him/herself is not sick, we call it a stable patient. When he/she finds a long queue, he/she opts to leave the clinic and reschedule for the test next time. (Interview/Counselor, dispensary)
Apart from lack of comprehensive face-to-face education, patients revealed that none of the posters on the clinic notes board and at the health facility at large were hung to advocate for VLT and its importance. I can see that there are banners talking about TB, CORONA, and Dengue fever, those are the banners that we can see here, but no one among those that talk about viral load, I have never seen that. (FGD/33 years old female, 7 years in care, health center)
Healthcare providers were also not sure of the availability of visual sources of VLT education. For clients? I don't know if there are posters, but for us there are guidelines. (Interview/Clinician, hospital)
Lack of Integrated Care Services
Competing priorities were reported for patients with multiple chronic conditions at the health center and dispensary level, as they had to visit other clinics to attend to their specific medical conditions. Lack of integrated care was therefore said to contribute to missing the VLT appointment as the patient reports below. So, you can find that the day that he/she is supposed to attend for sample collection for VLT at (Name of a facility) is the same date that he/she is supposed to receive a service at another hospital for another condition. (FGD/24 years old female, 6 years in care, health center)
On the other hand, healthcare providers acknowledged the existence of multiple chronic conditions among HIV patients and that the severity of other disease conditions was also the main attribute of missing VLT. However, they have been making efforts, including a home visit, to ensure VLT and other HIV care is done. I've four patients who are paralyzed and can’t move. I have to make a home visit for the viral load sample collection, because they’re not stable. (Interview/CTC in charge, health center)
Unavailability of VLT Services at Evening Hours
While VLT is performed in the morning hours and early afternoon, healthcare providers reported that some patients coming late or VLT. This was the contributing factor for missing other important services, including the VLT as they only manage to collect ARTs. This was confirmed by care providers as a barrier for VLT services. For instance, a client is supposed to come to the clinic today for the tests. Unfortunately, he or she doesn’t show up and s/he may show up the day after tomorrow. Sometimes come very late, like at 13:00 whereby samples for other tests have already been taken to the laboratory. (Interview/Counselor, health center)
All samples from all health facilities in the city have to be shipped to the central laboratory for early processing and analysis. We have a phlebotomist here, so after the doctor orders the test, the client is sent directly to the phlebotomy room. There is a lady who is a phlebotomist; she collects samples from clients. Then a motorcyclist on duty will be called to transport samples for viral load testing to Temeke (a regional referral hospital). (Interview/Clinician, Hospital)
To increase the number of patients in testing for VL, healthcare providers were advised to reschedule and extend time for service provision to attend late comers as testified by the expert patient. There are many fellow clients who we used to communicate to. You may find someone telling you that, for him/her the right time to come for clinic is 6 pm. So, the center should prepare two staff who will volunteer to work until evening so that those clients can come in the evening and access the clinic services. (FGD/21 years old, expert patient, Male, 17 years in care, health center)
Suggested Areas for Improving VLT Uptake
While examining the potential suggestions for improving VLT uptake, three key themes emerged which included information sharing (communication), extension of service hours, and knowledge sharing
Information Sharing (Communication)
Due to missing appointments, participants suggested to have early and consistent communication together with having an effective patient tracking to improve the VLT uptakes. Care providers do not call us, and a client can forget to come to the clinic in the scheduled date. For example, I was supposed to come for the service on 24th but, I found that the date scheduled for had already passed. I think I needed someone who could have reminded me. (FGD/47 years old, expert patient, Male, 6 years in care, dispensary)
Patient tracking was seen important especially for the reminders either for them to pick up the results or recollection of the samples in case the first one was noted to be unsuitable for testing. Because this schedule of 3 or 6 months is a long time so if the results are out, they should send us a text message to tell us our results, it will really help us because as a client I can come back and repeat the test before the 6 months. Not that after 6 months when I come for my scheduled clinic is when they tell me there is no results because my sample was destroyed. (FGD/47 years old female, 13years in care, health center)
However, contrary to what patients responded, healthcare providers reported to have time of making a phone call to some of the patients as a remainder for their sample collection appointment as revealed in the quote; We do make phone calls. Sometimes when we do so, some patients may tell you, “I am on my way; I will be there, doctor. (Interview
In addition, healthcare providers do encourage patients to record the facility contact information for them to call and report in case of any challenge. We have the clinic specific contact for the clients, so during consultation, we insist them to record the facility phone number, and use it to communicate with the clinic staff in case of anything. (Interview/phlebotomist, Hospital)
On the other hand, healthcare providers agreed on having limited materials for health education and they all agreed the importance of developing and distributing information, education, and communication (IEC) materials and strengthening health education as awareness raising to patients regarding the VL test. First, we should also try to develop, produce and hang up posters for HIV viral load as we used to do for other indicators, maybe that could help. (Interview/Counselor, health center)
Extension of Service Hours
Participants suggested to have time extension for sample collection to those patients who come late for the services. … you find that a client may come at 1PM, because s/he was attending personal activities, or their offices and noon time is the only opportunity to come to the clinic. However, when s/he arrives to the clinic he is told ‘yes today was the date for you to provide sample for VLT but you have come late so will have to come again tomorrow.” So, my advice is that the time for sample taking should be extended because every client who comes here has his/her own challenges. (FGD/ 24 years old, expert patient, Female, 6 years in care, health center)
Some of the healthcare providers are committed to adhering to the protocol on sample collection and transportation. However, a challenge was noted such that if they are to allow for the collection of samples at late hours it implicates to also notifying the person from the central lab to come back for transportation of the late collected blood samples. But that doesn't bother us much though it's a problem because you have to call the motorcycle rider again to come back to take the blood sample. Even though we have set a deadline at 12:00, but when a patient shows up late, we must call someone for sample transportation. (Interview/Counselor, health center)
Knowledge Sharing
Health education was frequently reported by participants and recommended that if the sessions are improved and education provided in a better way, it will help to improve the awareness on the importance of doing the VLT. They should improve on giving education about viral load, because you can find that another client is old, he does not know the meaning of viral load, they need to be told clearly that this is a test that involves this and that … Because not all are educated and understand this issue of viral load. So, I suggest that education be provided to patients efficiently to enhance their understanding such that when they go into the doctor's room, it is easy for them to know which test they are supposed to do and they can even ask questions or ask for the test. (FGD/30 years old female, 7 years in care, health center)
However, healthcare providers continued defending the points that they have been trying their best to share knowledge on VLT to the patients. They[patients] have knowledge because education is provided daily in our clinic, and we have written all of the client rights on the noticeboard, so they are aware of not only their rights but also the status of their problem. (Interview/CTC in charge, dispensary)
Some complaints were directed at some of the patients for coming late to the clinic, where they found the health education session had ended. There are others who come at 13:00 o'clock in the afternoon when the clinic time is about to end, so you will have to share health education depending on the individual needs, and this has to be in the consultation room. (Interview/Clinician, Hospital)
Discussion
Qualitatively, we examined the barriers and potential suggestions for improving VLT uptake in Dar es Salaam, Tanzania. The majority of the participants had been providing (HCPs) or receiving (PLWHV) HIV care for an extended period; as a result, they had unique perspectives on the barriers and potential suggestions to improve VLT care. The findings have revealed individual and system-level barriers to hinder VLT uptake, whereby missing appointments, and limited knowledge of VLT importance been identified as the main individual barriers. System-level barriers included a shortage of staff, inadequate health education, a lack of integrated care services, and the unavailability of VLT services at evening hours.
Patients reported missing appointments as the main individual barrier to VLT uptake, for several reasons, such as distance and an unaffordable transport fee. Similar information was reported by the healthcare providers during interviews, who claimed not to see some of the patients in their daily list of eligible patients for VLT, and that has been an ongoing challenge. This has been commonly reported in LMICs, where patients with chronic conditions records several missed care appointments. 26 It is estimated that a patient can use $2.5–$6.5 as a return cost for transport to the clinic, 27 and in Tanzania, HIV-infected patients are estimated to use up to US $26.51 per year (2–4 clinic attendance per year) to cover transport costs to the care facilities. 28 Suggestions have been made to advise patients to attend the nearby care facilities; however, due to a lack of privacy, stigma from and toward their fellow residents remains a challenge. 6
Apart from unaffordable transport costs, we learned that some system-level barriers contribute to patients missing appointments. For instance, a lack of integrated care services for chronic conditions contributes to patients’ failure to access the VLT. The current model remains PLWH receiving their HIV care at the CTCs. Other care such as for NCDs are integrated into primary healthcare (PHC) services at lower-level facilities and vertically running at tertiary level facilities. HIV care is not integrated into routine PHC and is vertically funded as compared to other chronic conditions clinics at all levels of healthcare facilities. 17 Patients with multiple chronic conditions have reported visiting multiple clinics as a result of competing priorities, 17 which pose the risk of repeated missed appointments. On the other hand, there is some promise for reducing the cost of healthcare services with the new integrated care services model. For instance, findings from a pilot study on a model of integrated care for HIV and NCDs in Tanzania and Uganda describe that integrated management of two or more conditions in a person was less expensive for service payers and reduced household costs for service users compared to managing multiple conditions separately without an integrated approach. 17
ARVs have resulted in a prolonged life span for patients with HIV, which exposes them to the risk of developing non-communicable diseases. 29 A model of integrating services for HIV and other chronic conditions has been suggested, and it is under trial to determine if it can be effective to remove multiple standalone clinics for an individual patient with multiple chronic conditions.17,30 Managing HIV and other conditions at a one-stop clinic could help patients resolve competing priorities for services to attend at a time.
In this study, we also learned that there is an unavailability of VLT services in the evening hours. The operational hours for VLT sample collection in Tanzania start at 8:00 and end at 13:00, followed by transportation of the samples to the central laboratory. In Dar es Salaam, the central laboratory is located at the Temeke regional referral hospital, where all samples from the city and nearby coastal regions are processed and analyzed. Both patients and healthcare providers reported that some of the patients have been coming to the HIV clinic at late hours and ended up collecting ARTs only while missing other important services, including the VLT. Inaccessibility of after-hours HIV care has been reported in some of the LMICs, and patients would like this resolved. 31 Even though healthcare providers reported having the option of calling back the responsible person for transport of late-collected samples, this claim was practically denied by patients, and the statements of other healthcare providers reflected the same.
Other system-level barriers widely discussed included the shortage of staff and inadequate health education on VLT. Shortages of staff remain a great challenge to the health sector in resource-limited countries, and as a result, patients fail to access quality health care services.32–34 On the other hand, due to inadequate health education on the VLT at large, patients fail to value the importance of monitoring their treatment outcomes, and so they can skip some of the important HIV care services like the VLT. The inadequate health education and information exchange between the care providers and their patients have been reported in Tanzania and are said to contribute to poor utilization of health care services just because the patients lack awareness. 35
On the other hand, factors that were suggested to improve VLT uptake include information sharing. Participants suggested that having early and consistent communication together with effective patient tracking would significantly improve VLT uptake. Published data indicates that patients are likely to adhere to the treatment and access health services at their facility if they experience better communication from the healthcare providers.36,37 Communication is paramount to ensuring the sustainable engagement of patients in health care services. However, due to other system barriers, raising individual awareness of VLT and enhancing communication may not be enough to enhance VLT uptake. But enhancing the system overall would be beneficial. Some examples from what we found in this study include fixing the issue of timely specimen transportation, offering transportation subsidies, 38 and scheduling appointments during the evening.
As suggested above, extending service hours for sample collection to those patients who are busy with their daily routines and childcare could be helpful. The current practice doesn’t allow some of the key care services to be provided to late comers and poses the risk for these kinds of patients to miss the proper management. 31 Even if the patient looks stable, supplying ARVs only at the emergence window doesn’t give other opportunities for holistic care and treatment. That is to say, social economic and health-related needs should be considered and addressed to support patients with social economic challenges who need to access healthcare services. Therefore, the ministries of social welfare and health should work together to address the challenges facing poor patients. According to the published data, patients who come late and receive limited services feel like they are being denied their right to care and treatment and would like the services to be available at any time they attend the health care facilities. 31
Strengths and Limitations
The evidence from this study can help design ways to improve Tanzania's access and quality of VLT uptake. The study collected information from a cluster of healthcare facilities with representation from primary to tertiary level facilities. Most of the participants were those with long-time HIV care experience and, therefore, provided unique perspectives on barriers and potential suggestions to improve VLT care. All those methodological approaches have increased the reliability of the data. However, this study had some limitations. First, we only included public facilities in the city that are NGO-supported, so we cannot generalize the results to private or rural facilities or non-supported public facilities. Second, the FGD respondents were those who recurrently attended their respective HIV care and treatment clinics. We did not receive responses from patients with a track record of missing follow-up appointments or commonly missing appointments. Their experience could have resulted in a different view than that presented in this study. Third, we only included adult patients, adolescents, and children could have provided a different experience on VLT services. Fourth, we didn’t capture the facilitators of VLT among participants and only collected suggestive measures to improve the service. Facilitators could have informed the stakeholders of the strength of the current practices. Lastly, due to time and limited funds, we conducted a limited number of FGDs and interviews at only six public health facilities in Dar es Salaam city. More facilities, including those from other regions of the country and FGDs would have improved the strength of the study’s findings.
Conclusion
These qualitative findings build on prior research to examine the experiential quality of HIV viral load services in Tanzania. It offers insight to HIV stakeholders on improving the rates and quality of VLT services. That is to say, regardless of the existing challenges, the findings indicate there is room to improve the rates of VLT uptake. The highlighted individual barriers need attention from all stakeholders, while effective communication, extension of service hours, and sufficient health education would significantly contribute toward effective care and treatment services. On the other hand, efforts to keep improving the amenities and the number of staff are needed to support the quality-of-care services. A holistic approach, including the adoption of an integrated care services model, is needed to work on the individual, and system-level barriers to improving the rates of uptake and quality of VLT services in Tanzanian public health facilities.
Supplemental Material
sj-docx-1-jia-10.1177_23259582241273385 - Supplemental material for Patients’ and Care Providers’ Reported Barriers and Suggestions for Improving HIV Viral Load Testing in Tanzania: A Qualitative Study in Dar es Salaam
Supplemental material, sj-docx-1-jia-10.1177_23259582241273385 for Patients’ and Care Providers’ Reported Barriers and Suggestions for Improving HIV Viral Load Testing in Tanzania: A Qualitative Study in Dar es Salaam by Peter M. Karoli, Elizabeth H. Shayo, Grace A. Shayo, Zenais A. Kiwale, Claudia A. Hawkins, Sylvia F. Kaaya and Lisa R. Hirschhorn in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582241273385 - Supplemental material for Patients’ and Care Providers’ Reported Barriers and Suggestions for Improving HIV Viral Load Testing in Tanzania: A Qualitative Study in Dar es Salaam
Supplemental material, sj-docx-2-jia-10.1177_23259582241273385 for Patients’ and Care Providers’ Reported Barriers and Suggestions for Improving HIV Viral Load Testing in Tanzania: A Qualitative Study in Dar es Salaam by Peter M. Karoli, Elizabeth H. Shayo, Grace A. Shayo, Zenais A. Kiwale, Claudia A. Hawkins, Sylvia F. Kaaya and Lisa R. Hirschhorn in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors are very grateful to the study facilities and participants who consented to participate in this study.
Author Contributions
PMK, GAS, EHS, SFK, CAH, and LRH served as lead for study conception and protocol writing. PMK, EHS, and ZAK served as lead for responsible for the data collection. PMK, ZAK, EHS, and LRH served as lead for Data cleaning and conducting data analysis. PMK, EHS, GAS, and LRH served as lead for writing the manuscript. PMK, EHS, GAS, SFK, CAH, and LRH served as lead for conducting critical review to the paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Fogarty International Center of the National Institutes of Health (NIH) under Award Number D43TW010946. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Ethical Consideration
Ethical clearance was obtained from both the local Institutional Review Boards (IRBs) No. DA.282/298/01.C and No. NIMR/HQ/R.8a/Vol.IX/3902 and the collaborating international institution IRBs No. STU00215874. We also got permission to conduct this study from the study area authorities, the selected districts and their respective health facilities following a thorough explanation of the rationale of the study. Informed consent was obtained from the study participants. We observed the anonymity of the participant's data, voluntary participation, confidentiality, and privacy throughout the study. Transcripts in electronic format were password protected and were only accessed by authorized study team individuals. Compliance to all institutional review boards’ terms and conditions were observed during execution of this research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.