
Abstract
This study represents one of the few exploring the effectiveness of an integrated HIV nurse navigation program on engagement and virologic outcomes. A navigator provided individualized care management (eg, pillbox renewals), intensive outreach, and collaboration with existing support systems (eg, families, community programs). Clinical data from the Veterans Affairs (VA) Medical Center site of a longitudinal, observational study of HIV in the District of Columbia (DC) cohort were used for comparison (N = 706). Navigation patients (n = 84) were less likely to have permanent housing, and more likely to be disabled, have detectable viral load, comorbid depressive, and substance use disorders. Navigation patients showed improvements in clinic visits (doubled), rate of medication renewal (40.91% to 80.61%), CD4 count and CD4%, and viral rates of Veterans with <200 copies/mL increased from 47.6% to 69.0% after one year. Integration of nurse navigation into a HIV primary care setting shows promise in improving engagement and virologic suppression in a high-risk population.
Keywords
Introduction
Patient navigation is a recommended intervention that may improve retention and engagement as defined by regular clinic attendance, medication adherence, and virologic suppression. 1 Patient navigation was first pioneered in 1990 to address the disparities in cancer outcomes by reducing barriers to care. 2 This included creating partnerships between the patient, medical team, community resources, and social support. Despite advances in antiretroviral therapy (ART), individuals with HIV are observed to experience similar challenges to successful outcomes. For example, there is consistent and progressive loss of individuals linked, retained, and engaged in HIV care. 3 The most recent US surveillance report noted that out of the estimated 1 218 400 US individuals currently living with HIV, only 36.2% were prescribed ART and 30.2% had viral loads less than 200 copies/mL. 4 This is a discrepancy in outcomes compared to the targets set by the Office of National AIDS Policy 3 and the Joint United Nations Programme on HIV/AIDS 5 to achieve the following by 2020: 90% with HIV diagnosis will receive ART and 90% of those receiving treatment will achieve viral suppression. Effective and innovative interventions that target engagement are needed in order to help achieve successful HIV outcomes for all and with this in mind, nurse navigation started to be integrated. 6
The Washington, DC Veterans Affair Medical Center Infectious Disease Clinic, an urban primary care clinic with a predominantly African American patient base, observed challenges in sustaining engagement for a subset of at-risk veterans. Despite employing the “medical home” approach where each patient’s team consists of a medical support assistant, nurse practitioner, and physician along with an integrated on-site team of social workers, a clinical pharmacist, a hepatologist, a diabetes specialist, and an HIV psychologist, 21% of HIV-positive veterans with at least 1 visit in 2013 still had a detectable viral load. 7 Furthermore, those who obtained initial virologic suppression were at extremely high risk for viral rebound—approaching 40% at 2 years. 8
In order to facilitate full engagement in care and support virologic suppression, the clinic hired a dedicated nurse navigator (registered nurse) in March 2014. Her primary responsibilities were to create a navigation program that promoted engagement in care, implementing strategies to increase medication adherence. The program included coordinating with the clinical team to provide HIV health education, providing reminders to the patients to support regular clinic attendance, and medication adherence support interventions (ie, text reminders, pill boxes). The primary aim of this study was to examine the characteristics of patients referred to the nurse navigator as compared to a representative sample of HIV-positive veterans. The secondary aim was to assess the impact of nurse navigation on key outcomes: HIV-1 RNA viral load, CD4 count, CD4%, medication adherence, and clinic attendance.
Methods
Study Population
All veterans (approximately 1 000) enrolled in the Infectious Disease (ID) primary care clinic were eligible for the nurse navigation program. Prior to the implementation of the nurse navigation program, 200 veterans were with detectable viral load. Patients were referred for navigation after being identified as poorly engaged in care by any member of the clinical team listed above. Poor engagement in care was evidenced by either multiple no shows for scheduled appointments, inconsistent medication renewal, and/or elevated viral loads. The nurse navigator maintained a clinical registry as part of regular clinical care. Individuals referred to the nurse navigator between March 1, 2014, and March 1, 2015, were identified retrospectively for this study. Since this was a secondary data analysis of a clinical database, this study was exempted from review by the institutional review board of the participating medical center, since the study posed minimal risk to patients’ privacy, and any identifying data were removed to maintain confidentiality.
Comparison Sample
Since this was a retrospective secondary data analysis, there were no baseline data for the rest of the general clinic population. As a substitution, this study compared navigation patients to veterans enrolled in the District of Columbia (DC) cohort in order to explore the differences between individuals referred to navigation versus the overall veteran population enrolled in the ID clinic during the study period. The DC cohort is a longitudinal, observational study of HIV-positive persons receiving care at 13 major clinics in the DC. 9 There were 706 patients receiving care in the Veterans Affairs (VA) clinic and enrolled in the DC cohort between January 2011 and March 2014. 10 For the period under study (January 2011-March 2014), the total VA clinic population was approximately 1 000 patients. There were no significant differences in gender and ethnicity between veterans who enrolled and declined (n = 68) to participate in the DC cohort; therefore, the cohort population is a likely representative of the general clinic population. District of Columbia cohort’s data and statistics coordinating center provided the comparison data for this analysis. All participants in the DC cohort signed an institutional review board–approved informed consent. Given the methods used in this project, it is likely that navigation patients were also enrolled in the DC cohort. Navigation veterans were not excluded from the DC cohort data.
Intervention
The nurse navigator has experience working within integrated teams and chronic disease management. In addition to her educational (registered nurse) and clinical experiences, the clinical staff described her as a warm, caring, and compassionate provider. Many of the veteran experienced stigma related to their HIV diagnosis along with other discriminations related to comorbid conditions (eg, homelessness, substance use disorder). The mission for the ID clinic is to create an inclusive and accepting “medical home” environment for their veterans.
She provided an individualized approach that included care management, intensive outreach, and collaboration with existing support systems (eg, families, social work, community programs, and other medical services). The higher level of outreach provided by the nurse navigator is exemplified by comparing responses to missed clinic visits. As a standard practice, a veteran missing an appointment received 2 phone calls and a letter requesting they contact the clinic to reschedule the appointment. In contrast, the nurse navigator actively reached out to patients by calling both the veteran and any available emergency contact until the patient was reached.
Other unique implemented strategies include medication adherence and clinic engagement support in the form of pillbox renewals, reminder calls (ie, upcoming appointments and medication renewal), aiding veterans with text reminders, the same day walk-in appointments, and collaboration with family members and other medical staff. Finally, the nurse navigator maintained a database of the patients she supported, which included medication renewal dates, upcoming appointments, and a record of most recent contact. She regularly maintained the database and disseminated any pertinent information (eg, patient moved out of state) to the rest of the treatment team.
Study Variables
Demographic data, comorbid psychiatric and substance use diagnoses, and HIV engagement indicators were obtained for all navigation patients through review of the clinical registry and electronic medical records. Demographic and clinical data collected included age, gender, racial/ethnic group, housing status, employment status, mental health diagnoses, and substance abuse diagnoses.
HIV engagement and outcomes were assessed by a combination of lab values (viral load, CD4 count, CD4%) and clinic adherence indicators (number of scheduled ID clinic visits, percentage of completed medication renewal). The infectious diseases laboratory performed the clinical viral load, CD4%, and CD4 counts for the medical center as part of regular clinical practice and to monitor health outcomes.
Prenavigation laboratory values were the most recent value before or at the start of navigation. Prenavigation clinic visits and percentage of completed medication renewals were assessed 6 months prior to enrollment in the navigation program. Postnavigation viral load, CD4 count, and CD4% were identified as laboratory values closest to July 31, 2015. Postnavigation clinic visits and medication renewals were collected from the start of enrollment until the end of data collection (July 31, 2015). Undetectable viral load was defined as less than 200 copies/mL. The duration of the nurse navigation program was measured in days.
Data Analysis
Statistical analyses were performed using PASW Statistics version 20. 11 Descriptive statistics are reported for all measures. Baseline differences were analyzed using t tests and χ2 tests.
Results
Navigation patients (n = 84) consisted of 82 (97.6%) males and 2 (2.4%) females. Mean age was 55.12 years (SD = 11.88) and most were black (n = 72, 85.7%) with stable housing (n = 53, 63.1%). There were variabilities in sources of income with approximately a third reporting having full- or part-time employment (n = 25, 29.8%). More than half (n = 44, 52.4%) had HIV viral load of 200 copies/mL or greater. The mean CD4 count was 355.67 (SD = 269.78) and CD4 mean percentage was 19.11% (SD = 11.90). Other demographic and clinical information are shown in Table 1.
Baseline Comparisons between Nurse Navigation and DC Cohort Participants.

Abbreviations: DC, District of Columbia; IQR, interquartile range; SSI, supplemental security income.
Navigation Sample Compared to DC Cohort
Baseline demographic and clinical characteristics of navigation patients (n = 84) compared to the DC cohort veteran population (n = 706) are shown in Table 1. Since enrollment was ongoing, enrollment period ranged from 156 (5.2 months) to 497 days (1.4 years). The navigation patients were less likely to live in permanent or stable housing (n = 53, 63.1%) compared to the general DC cohort population (n = 646, 91.5%), P < .001. They were more likely to be disabled or to be receiving disability (navigation = 23.8% vs DC cohort = 1.3%; P < .001) and have a comorbid depressive (navigation = 31.0% vs DC cohort = 18.3%; P = .03) or substance use (alcohol and illicit drugs) disorder (P < .01).
Navigation patients (n = 40, 47.6%) were also less likely to have a viral load <200 copies/mL compared to the DC cohort sample population (n = 536, 75.9%). Additionally, navigation patients were more likely to have AIDS by CD4 count and CD4% criteria (n = 28, 33.3%) compared to the DC cohort population (n = 75, 10.6%) and less likely to have a CD4 count ≥500 cells/mm3 (n = 24, 28.6%) compared to DC cohort patients (n = 363, 51.4%).
Changes in Postnavigation Enrollment
Pre- and postnavigation values are shown in Table 2. Prenavigation, 33% of patients (n = 28), had a CD4 count <200 cells/mm3 and 42.9% (n = 36) had a CD4% <14%, meeting the CD4 criteria for AIDS. For those with viral loads greater than 40 copies/mL (n = 50; 59.5%), the mean viral load was 73 097.06 copies/mL (SD = 177 735.89). Prenavigation patients attended clinic once (
Pre- and PostNavigation Comparisons.a
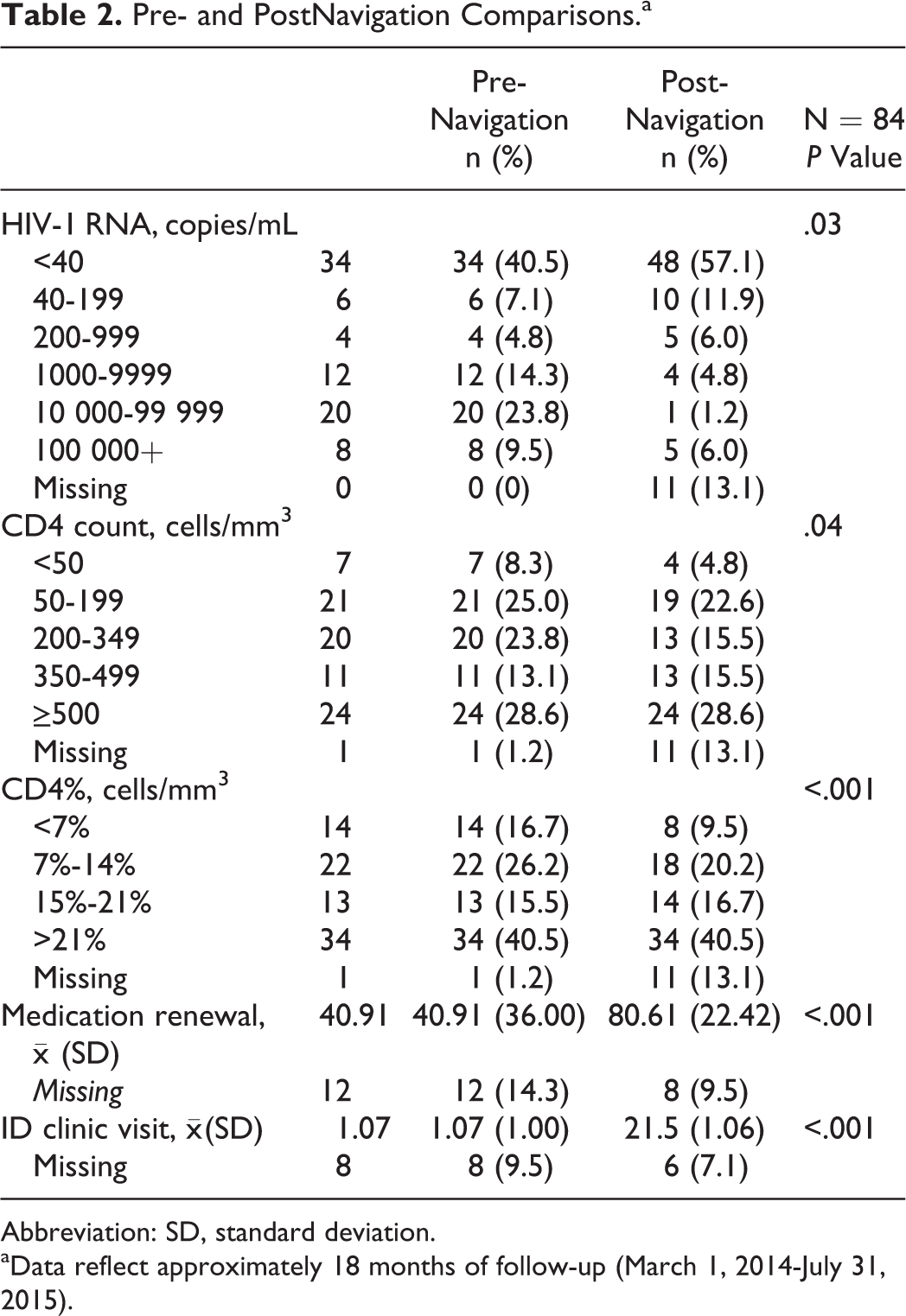
Abbreviation: SD, standard deviation.
aData reflect approximately 18 months of follow-up (March 1, 2014-July 31, 2015).
Following navigation, viral suppression (<200 copies/mL) was achieved in 69.0% (n = 58) of patients, compared to 47.6% (n = 40) of patients prenavigation. Notably, 2 patients with baseline viral loads greater than 100 000 copies/mL were able to achieve viral loads <40 copies/mL postnavigation. The median CD4 count increased from 295.0 to 375.0 cells/mm3. In addition, 30% of the participants with CD4 counts <200 cells/mm3 increased their CD4 counts to ≥200 cells/mm3, with 1 participant achieving ≥500 cells/mm3.
Paired-samples t tests were conducted to compare the number of ID clinic visits and the rate of medication renewal. There was a significant increase in the number of clinic visits from 1.1 (SD = 1.00) prenavigation to 2.1 (SD = 1.06) postnavigation, t(74) = −9.14, P ≤ .001. There was also a significant increase in the rate of medication renewal from 40.9% (SD = 36.00) to 80.6% (SD = 22.42), t(69) = −8.75, P = <.001.
Discussion
Our data provide an early assessment of outcomes on integration of a dedicated nurse navigator in an urban, predominantly African American HIV Clinic. We have demonstrated that among patients with challenges to engagement in care, an integrated nurse navigator program may promote clinic visits, medication renewals, and virologic suppression. Prior research has linked these factors to reduced hospitalization, 12 reduced instances of AIDS-defining illness, 13 and improved survival. 14
The findings here are particularly significant, given the population of patients referred for nurse navigation. Previous studies note significantly lower retention rates in HIV care among minorities, 15-16 individuals with comorbid mental health and substance use disorders, 17-18 and individuals with lower baseline CD4 counts. 16,19 The current sample enrolled in nurse navigation included those at highest risk within an already high-risk population, those with disability, the absence of permanent and stable housing, depression, current substance use disorder, and CD4 counts meeting the criteria for AIDS. These individuals have the greatest risk of opportunistic infections, hospitalization, and poor HIV outcomes. A focused and individualized navigation intervention can achieve considerable movement toward the previously mentioned 2020 targets of 90-90-90: 90% in care, 90% on ART, and 90% virologically suppressed. 5
A primary limitation of our study is that this was not a randomized, controlled trial. It is possible that the act of referring a patient for navigation was sufficient stimulus to heighten an individual’s awareness of the critical nature of engagement in care and consequently improve engagement without navigation intervention. In addition, the individualized nature of the intervention made it difficult to identify specific mechanisms of action (eg, phone calls, pill box, nurse navigator’s interpersonal style) that best facilitate engagement in care. Although conducting a more controlled research study may provide this insight, there was valuable information gained by the study of this real-world clinical application of nurse navigation.
An additional consideration is that there were a number of patients with missing follow-up data, despite the 5-month duration with navigator. The missing information may have caused some participants with significant changes to go undetected. There may have also been data from those who had no change, thus reducing the size of impact observed. Furthermore, we did not collect participants’ reasons for failure to re-engage along with the details of navigation services (ie, number of calls, type of contact), which might have allowed for a more nuanced assessment of our data.
Despite these limitations, the results of the present study do suggest that integrating nurse navigation into a primary HIV care setting has a significant effect on engagement in care, medication adherence, and virologic suppression among those at greatest risk of poor HIV outcomes. In addition, our results highlight the importance of high-level, individualized care, particularly for individuals who have difficulties with sustained virologic suppression. Although our patient population consisted of veterans, our findings may generalize to other high-risk HIV-positive population. Future studies will focus on identifying specific treatment components that can promote reengagement and consistent engagement in care. In addition, we are also planning to evaluate the effects of navigation on viral rebound and the economic impact of the program compared to usual care.
Footnotes
Authors’ Note
Preliminary results of this study were presented as an abstract at the 2015 American Conference for the Treatment of HIV in Dallas, Texas.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.