
Abstract
Background
Uptake of HIV early infant diagnosis (HEID) among HIV-exposed infants is the key to timely initiation of Antiretroviral Treatment (ART). However, despite the availability of HEID services in Tanzania, its uptake is low. We aimed to determine predictors of mothers living with HIV’ with HIV-exposed infants’ uptake of HEID services in Iringa District, Tanzania
Methods
A health facility-based cross-sectional study was conducted in Iringa District from May to June 2023. Mothers with HIV-exposed infants were recruited in the study through a multistage sampling technique and interviewed using pre-tested structured questions. Logistic regression analysis was employed to determine potential predictors of HEID uptake.
Results
A total of 309 mothers with HIV-exposed infants participated in the study. About 78.3% of the HIV-exposed infants had initial DNA PCR for HEID within 6 weeks of age and 86.1% within 8 weeks. Most mothers had high perceived benefits on uptake of HEID with a mean score of 4.3, high perceived self-efficacy with a mean score of 3.8 and 2.7 perceived risk of HIV infection on their HIV-exposed infants on the 5 scale Likert scale with 5 showing the highest perceived benefit, self-efficacy and risk. High perceived self-efficacy and being a businesswoman were the predictors of uptake of HEID. The odds of self-efficacy on the uptake of HEID by 2.4 times (aOR 2.4 95% CI 1.6–3.2) within 6 weeks of age and 1.9 (aOR 1.9 95% CI 1.3-2.7) within 8 weeks. The odds of being a businesswoman were 0.4 for 6 weeks and 0.3 for 8 weeks (aOR 0.4 95% CI 0.2-0.8) and (aOR 0.3 95% CI 0.1-0.8) respectively.
Conclusion
Over three-quarters of the HIV-exposed infants had initial DNA PCR for HEID testing as recommended. Perceived self-efficacy was the main factor influencing HEID uptake. These findings highlight the need for strengthening HIV-positive mother's self-efficacy for improved uptake of HEID services.
Plain Language Summary
Predictors of mothers living with HIV’ uptake of HIV early infant diagnosis services in Iringa District, Tanzania
This study aimed to find out the factors associated with the uptake of HIV early infant diagnosis (HEID) services among mothers living with HIV in Iringa District, Tanzania. The uptake of HEID in Tanzania is still below the 95% national and global target of ending AIDS as a public health by 2030 We employed a cross-sectional study design and collected data from May to June 2023 to determine predictors of mothers with HIV-exposed infants’ uptake of HEID in Iringa District, Tanzania. The analysis was done by descriptive statistics and logistic regression analysis. A total of 309 mothers with HIV-exposed infants participated in the study. About 78.3% of the HIV-exposed infants had initial DNA PCR for HEID within 6 weeks of age and 86.1% within 8 weeks. Most mothers had high perceived benefits on uptake of HEID with a mean score of 4.3, high perceived self-efficacy with a mean score of 3.8 and 2.7 perceived risk of HIV infection on their HIV-exposed infants. High perceived self-efficacy was positively associated These findings highlight the need for strengthening HIV-positive mother's self-efficacy for improved uptake of HEID services.
Keywords
Introduction
Approximately 1.7 million children aged 0–14 years are infected with the Human Immunodeficiency Virus (HIV) globally with the majority 86% of them living in Sub-Saharan Africa. 1 During 2021, approximately 301 pediatric AIDS-related deaths occurred daily with 850 new children being infected daily. 2 Nearly half (48%) of the infants and children infected with HIV are not on anti-retroviral treatment (ART). 1 When infants infected with HIV are not on treatment, the mortality is highest during the second or third month of life and about half of them die before the age of 2 years.3,4
Timely initiation of antiretroviral therapy (ART) to infants with HIV infection decreases mortality among infants by 76% and progression to severe consequences by 75%. 5 However, timely ART initiation among these infants can only be possible with a prompt uptake of HEID. 6 The World Health Organization recommends HEID to all HIV-exposed infants (HEI) at 4–6 weeks of age with the use of NAT-DNAPCR. 7 Uptake of HEID is of profound benefit to both HIV- positive and HIV-negative infants and is the gateway to early clinical evaluation, provision of prophylaxis, timely ART initiation, optimal viral load suppression (<1000 copies/ml) and increased infant survival and health outcomes. 8 Despite the benefits of HEID. only 63% of HEI received the HEID test within 8 weeks of age globally, below the first 95% national and global target. 2
In Tanzania, HEID is integrated into the Prevention of Mother-to-Child Transmission (PMTCT) services. 9 The PMTCT services are offered by more than 90% of all health facilities in Tanzania. 9 Despite the wider availability and accessibility of PMTCT/HEID services in the country, the uptake of HEID services within 8 weeks of life has progressively decreased from 58% in 2016 to 46.6% in 2019 10 which is below the national target of 95%. 11
Increasing the uptake of HEID among the HEI in the country requires not only improved availability and accessibility of HIV testing services but also that mothers living with HIV sufficiently utilize the EID services for their HEI. 12
Several factors are reported to influence the accessibility and utilization of HEID services. These include health system and structural factors (logistics and supply, skilled staff), socio-economic factors (stigma, occupation), and individual factors (age, education level, parity, marital status, maternal duration of HIV status diagnosis, knowledge of HIV, PMTCT and EID.12,13 Although this information is useful in understanding the structural and contextual factors in HEID utilization it remains unclear on the potential influences to HEID uptake among mothers of HIV-exposed infants. Thus, we sought to determine the factors of mothers living with HIV on HEID uptake that can be targeted to improve the uptake of early infant HIV diagnosis using the constructs of the health belief model (HBM). The HBM model highlights key elements that influence decision-making in health-seeking behaviors, such as perceived risk, perceived benefits, and perceived self-efficacy.
Materials and Methods
Study Design and Setting
A cross-sectional study was conducted in eight healthcare facilities from two councils (Iringa Municipal Council and Iringa District Council) of Iringa District in the Iringa region in Tanzania from May – June 2023. Iringa region is in the western southern part of the country and is one of the three Tanzanian regions with the highest prevalence of HIV/AIDS. The region's estimated prevalence of HIV is 11.3%, which is more than double of the national prevalence of HIV (4.7). 14 Among women of reproductive age, the prevalence of HIV (15.5%) is also more than twice of the prevalence in men (6.6%) and it's the second region with a high prevalence rate of HIV in children (1.4%) in the country. 14
At the health facilities, HEID services are offered at post-natal clinics as a part of the Prevention of Mother-to-Child Transmission - Reproductive and Child Health (PMTCT- RCH) services. HIV-positive mother/caregiver should bring her HIV-exposed infant at a recommended age (4-6 weeks) to the health facility, where the same-day dried blood spot (DBS) sample collection is done by trained healthcare workers, particularly the nurses. The collected samples are then transported to the centers with equipped laboratories for the analysis of DBS samples. Before this, mothers living with HIV are informed during their routine ART/PMTCT visits that DBS samples will be collected from their infants initially at 4–6 weeks of life for early HIV status diagnosis. According to the guidelines, the results of the HIV test ought to be returned within a month post-DBS sample collection followed by timely initiation of ART for HIV-positive infants.
Study Population
The study enrolled mothers living with HIV with HIV-exposed infants aged 6 weeks to 18 months attending RCH clinics for HIV preventive services and vaccination at selected facilities offering services in the Iringa district during the study period and who agreed to take part in the study. The study excluded mothers with HIV-exposed infants who lacked the necessary records for cross-checking the date on which the initial DBS sample was obtained for HIV DNA-PCR testing.
Sample Size Determination
The sample size was determined using the formula for cross-sectional studies.
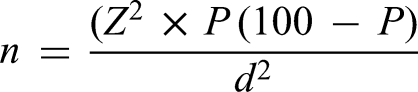
Sampling Technique and Procedure
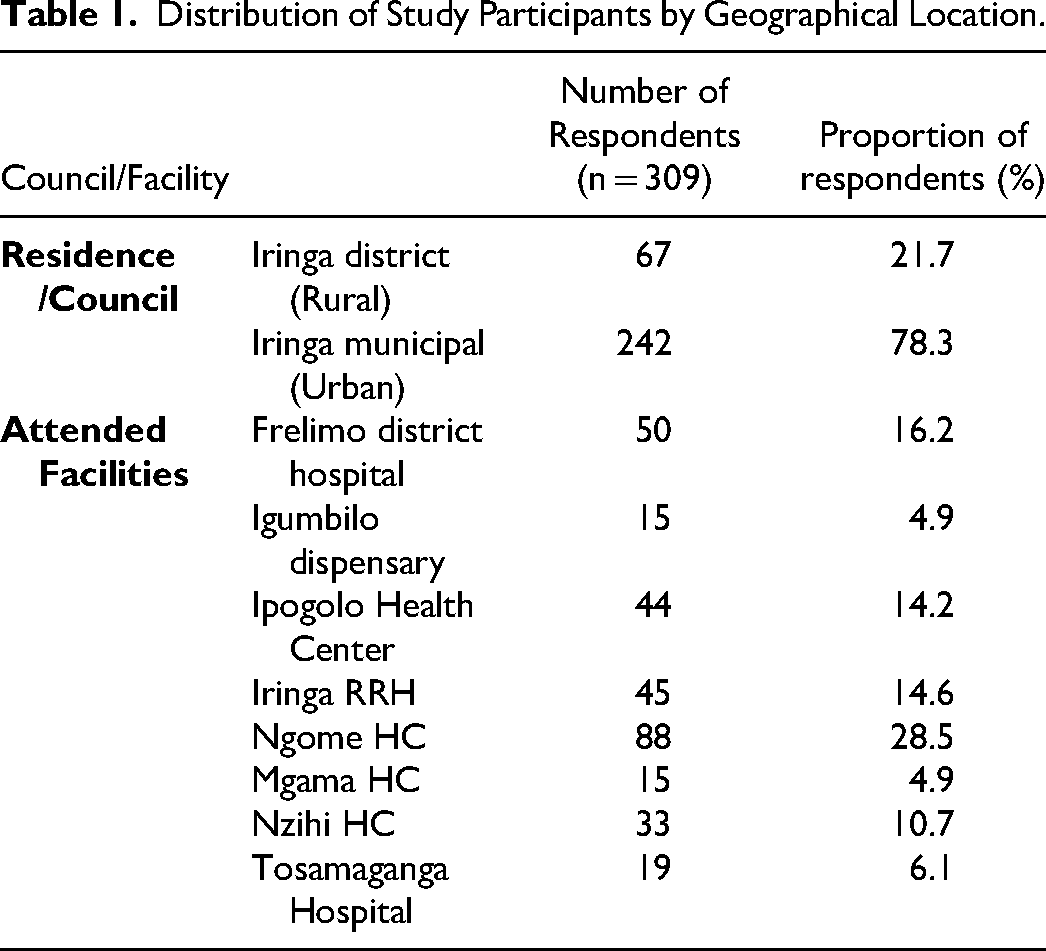
Multi-stage sampling technique was employed. In the first phase healthcare facilities were selected. A list of PMTCT-RCH high-volume health facilities was obtained. We defined a high-volume facility in this study as the center with more than 25 HIV-positive mothers with HIV-exposed infants aged 6 weeks to 18 months. Eight health facilities out of 16 high-volume facilities were randomly selected from the list for representativeness (Table 1). The total sampling frame had around 390 participants. High volume facility was determined by monthly flow rate based on 3 months follow up from registers to calculate the average monthly flow rate and clinic attendance per day.
Distribution of Study Participants by Geographical Location.
In the second phase of the study, participants were recruited at the selected health facilities. All HIV-positive mothers with HIV-exposed infants aged 6 weeks to 18 months were recruited and asked to participate in the study voluntarily as they came for follow-up visits or were contacted via telephone and at times through community-based healthcare workers until the sample size of 314 was attained
Data Collection Tools and Quality Assurance
Data collection tools consisting of pretested interviewer-administered structured questions were used to collect data from the consented HIV-positive mothers with HIV-exposed infants. The tool (Appendix 1) was administered by the first author and a team of trained research assistants and it was adopted from similar studies to fit the current study.16,17 The tool was administered using Kobo toolbox v15 and translated into Swahili language the language spoken by all Tanzanians. Pre-testing of the tool was done on 10 HIV-positive mothers with HIV-exposed infants at Sabasaba dispensary located in Iringa Municipal to confirm the clarity of the questions and ensure the data collected is of high quality. Cross-checking of the records (follow-up registers and HEI cards) was done to verify the reported information on the uptake of the HEID test.
Variables and Measurements
The study's dependent variable was the uptake of HEID (Yes or No). “Yes”, was for infants who had an initial HIV test (EID) performed within 6 weeks of age and “No” for those whose initial HEID was done when the baby was aged above six weeks of life (tested at ≥7 weeks of age). Sensitivity analysis was done for 8 weeks. The outcome variable was calculated from the date of birth of the infant to the date of the initial HIV test to get the exact age when HEID was performed. The independent variables were area of residence, age of HIV-positive mother, marital status, education level, occupation, parity (number of children) and HIV-related stigma. The three independent variables from the health belief model constructs (perceived benefit, self-efficacy and perceived risk,) were measured via a Likert scale consisting of a 5-point scale, ranging from strongly agree which scored 5 points in descending order to strongly disagree which scored 1 point for perceived benefit.
Six questions were asked to assess the perceived benefit. The scores for each question were summed up and divided by six to find the average score. The same process was done on the perceived self-efficacy which had three questions that examined the mothers living with HIV’ confidence on uptake of HIV early infant diagnosis and its results including how to manage emotional disturbances and stigma in case a child is found to be HIV positive. The perceived self-efficacy in this context is the mothers living with HIV confidence in the uptake of early infant HIV diagnosis and its results including emotional disturbances and stigma management, in case a child is found to be HIV positive. The perceived risk questions included six negative statements with reverse scoring from strongly agree which scored 1 point to strongly disagree which scored 5 points. We report the mean score and standard deviation for each construct.
Data Management and Analysis
Data collected with the Kobo toolbox was extracted into Microsoft Excel and then imported into STATA software version 18 SE for cleaning, coding, and analysis. Frequency and percentage were employed in descriptive statistics to summarize categorical data, whereas mean and standard deviation were used for continuous variables. Logistic regression was employed to compute crude odds ratios at a 95% significance level to determine factors associated with the uptake of early infant HIV diagnosis. Variables were statistically significant at a p-value less than 0.05. Variables that had p ≤ 0.2 at bivariate analysis were entered into a multivariate logistic regression to compute for adjusted odds ratio at a 95% significance level and to control for confounders to determine independent predictors of early infant HIV diagnosis uptake.
Ethical Approval and Informed Consent
This study received ethical approval from the Muhimbili University of Health and Allied Sciences Ethical Review Committee (Ref: MUHS-REC-04-2023-1619). All the methods in this study were performed in accordance with the relevant guidelines and regulations (Declaration of Helsinki). Before enrolment we explained the objectives and procedures of this study to the respondents and obtained informed written consent from them.
Result
Distribution of Study Participants by Geographical Location
Most Participants in this study were from Iringa Municipality (78.3%) (Table 1).
Social-Demographic Characteristics of the Study Participants
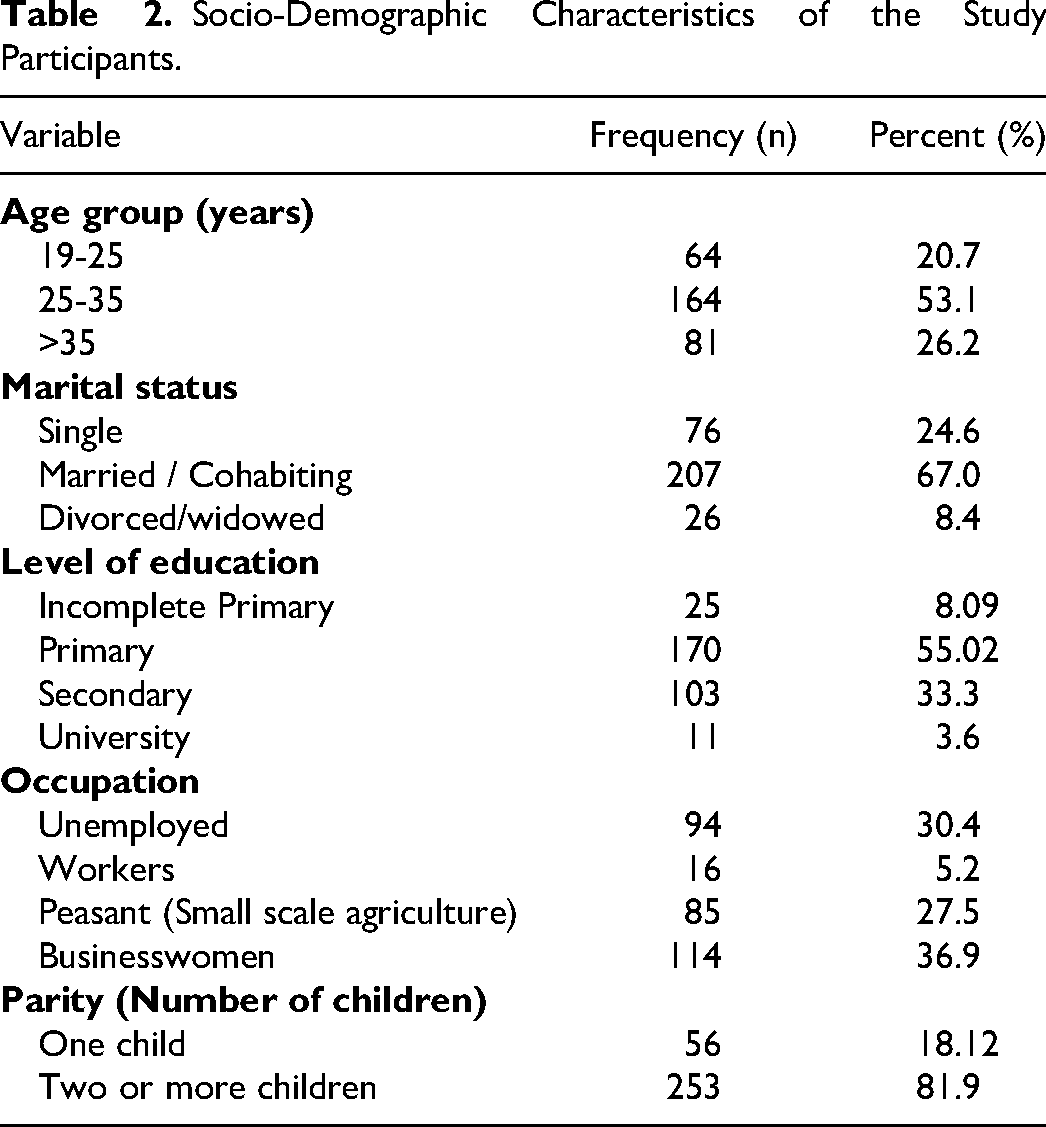
A total of 309 mothers living with HIV with HIV-exposed infants aged 6 weeks to 18 months participated in the study. More than half 164(53.1%) of the mothers were aged between 25 and 35 years, 64(20.7%) were adolescents and young women (19-25 years) and the mean age was 31(SD 6.5). Most of the mothers were businesswomen 114(36.9%), 170(55.02%) had primary education, 206(67.0%) married /cohabiting, and 252(81.9%) had more than one child (Table 2).
Socio-Demographic Characteristics of the Study Participants.
Proportion of HEID Uptake
We found that 241 (78.3%) of HEI had HIV testing within 6 weeks of life as recommended and 86.1% within 8 weeks of life. All children (309) had taken their HIV testing with 6.8% within 4 weeks and 89.0% within 10 weeks of life. Out of 90% of HEI who had their results at the time of study, 12 (5%) were HIV-positive. Among the HIV-exposed infants who tested positive, less than half 5(42%) were diagnosed within 6 weeks of life.
Description of Health Belief Model Constructs
The perceived risk from the six negative statements was 2.7(SD 0.6), the perceived benefit was 4.3(SD 0.6) and the perceived self-efficacy was 3.8(SD 1.0).
Factors Associated with the Uptake of HIV Early Infant Diagnosis
From logistic regression bivariate and multivariable analysis, perceived self-efficacy on the uptake of HEID was statistically significantly associated with high uptake of HEID between 6 weeks of life (Table 3). Being a businesswoman was also associated with less uptake of the EID in multivariate analysis. These results were still consistent when we did a sensitivity analysis within 8 weeks (Appendix 2).
Bivariable and Multivariable Analysis of the Factors Associated with the Uptake of HEID Services Within Six Weeks.
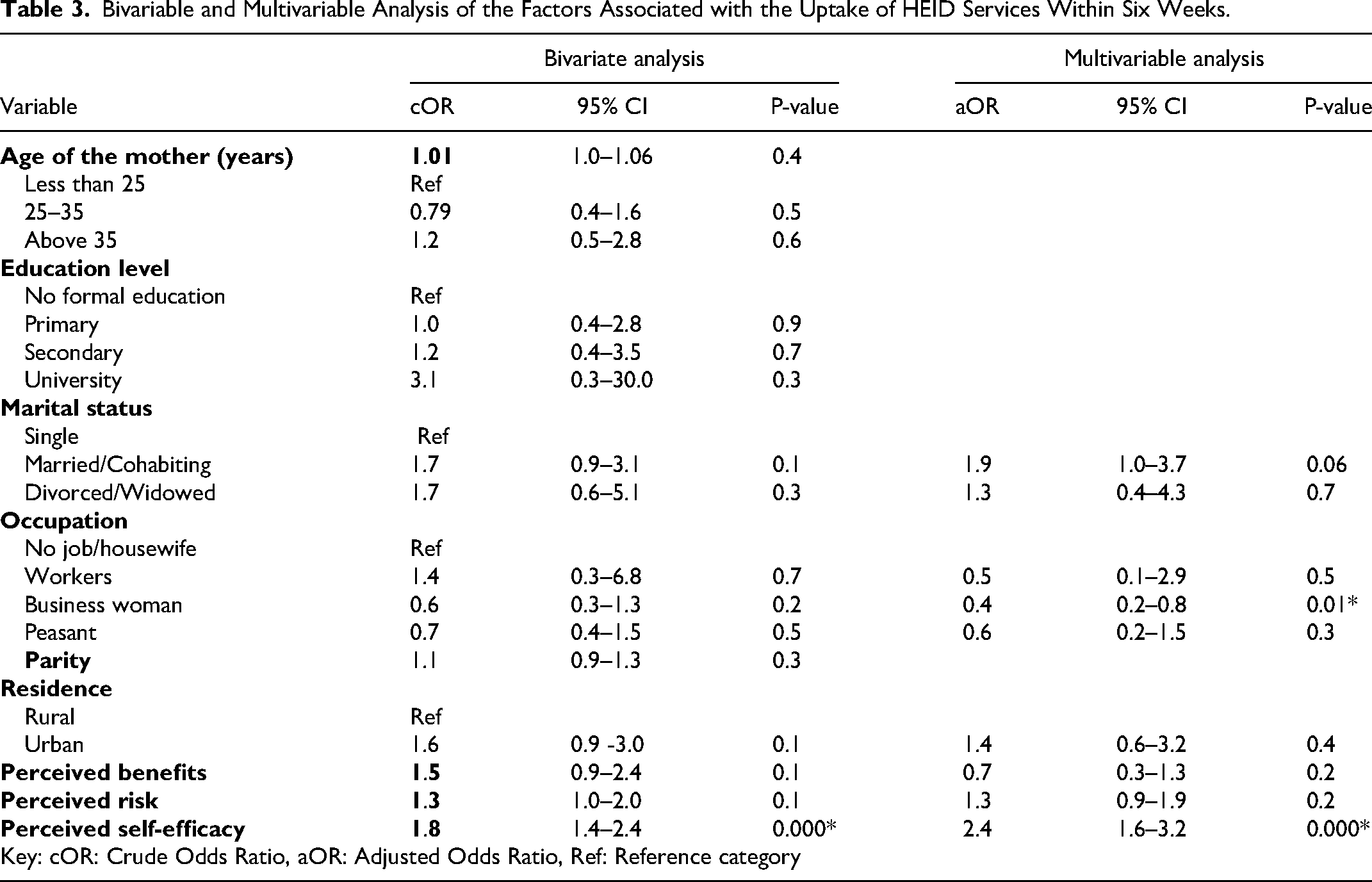
An increase of perceived self-efficacy by one unit on a 5 Likert scale would increase the odds of uptake of HEID by 2.4 times (aOR 2.4 95% CI 1.6-3.2) of bringing their HIV-exposed infants for the initial HIV testing within 6 weeks of age and 1.9 (aOR 1.9 95% CI 1.3-2.7) within 8 weeks. The odds of being a businesswoman were 0.4 in the 6 weeks and 0.3 in 8 weeks (aOR 0.4 95% CI 0.2-0.8) and (aOR 0.3 95% CI 0.1-0.8) respectively.
Discussion
We found that 78.3% and 86.1% of HIV-exposed infants had an uptake of HEID within 6 and 8 weeks respectively, which is still lower than the national target of 95%. Most of the mothers perceived HEID uptake as beneficial with a mean score of 4.3 out of 5, and self-efficacy with a mean score of 3.8, but nearly half of the mothers did not perceive the risk of HIV infection to their HEI with a mean score of 2.7. The mothers living with HIV perceived self-efficacy, and confidence in the uptake of HEID, which was an independent predictor of high HEID uptake while been a businesswoman was associated with lower uptake of HEID.
Proportion of Early Infant HIV Diagnosis Uptake
We found that 78.3% of HIV-exposed infants were tested within 6 weeks of life; the uptake of HEID found in this study is higher than the global (63%) and national (46.6%) estimates10,18 and also higher compared to previous reported studies in the country. In the Mbeya region, the uptake of HEID within 8 weeks of life was 75.6% 15 while in Muheza, Tanga, 57.1% of the infants had initial HIV testing within 6 weeks of life. 12 The time difference between the conduct of this study and previous studies might have accounted for the differences in the findings due to the ongoing efforts to scale up the utilization of PMTCT and HEID services in the country.
Mothers Perceived Self-Efficacy on the Uptake of Early Infant HIV Diagnosis
In this study, the mean score of perceived self-efficacy was 3.8 out of 5 with 5 points showing the highest self-efficacy on the Likert scale on the uptake of HEID services. The heightened perception of self-efficacy observed in this study may be due to the low HIV-related stigma reported at home, in the community, and health facilities in the study area, as HIV-related stigma affects perceptions. 19 High perceived self-efficacy on the uptake of PMTCT-HIV testing services was also reported among pregnant women in Sudan and Ethiopia. 17
A high perceived self-efficacy on the uptake of HEID services among mothers was also associated with high HEID uptake. Mothers with high perceived self-efficacy were more likely to bring their HIV-exposed infants for the early HIV diagnostic tests compared to those with low perceived self-efficacy. This finding is similar to previous studies conducted on determinants of HIV testing during Pregnancy in Sudan and predictors of HIV-test utilization in PMTCT among antenatal care attendees in Addis Ababa Ethiopia.17,20 These findings suggest that building self-efficacy among the populations including the mothers living with HIV’ is likely to have the utmost effect on HIV testing in general and particularly predispose the mothers to the uptake of the HEID test for their HEI. 21
Perceived Risk of HIV Infection in HIV-Exposed Infant
Nearly half of the mothers had a low perceived risk of HIV infection in their HIV-exposed infants with a mean score of 2.7 on the 5-level Likert scale with 5 points showing the highest perceived risk, contrary to a study conducted in Sudan, where most of the pregnant women had high HIV risk perception. 17 The low perception of HIV risk to the infants observed among the positive mothers in this study can be explained by the reported ART efficacy in preventing maternal-infant transmission of HIV-AIDs once a mother follows PMTCT recommendations, particularly adhering to ART medication use when pregnant and providing ARV prophylaxis to the infants after delivery.
In this study, perceived risk did not influence the uptake of HIV early infant diagnosis. The findings are similar to a study in Ethiopia. 20 This finding is contrary to a study in Sudan where high perceived risk influenced the uptake of HIV testing among pregnant women. 17 Understanding the risk of EID is important, health care providers’ role has been highlighted to increase the perception of the risk of HIV to HEU. Pregnant women should be informed of the risk of HIV to their newborn by providers during PMTCT pregnancy visits. 5
Perceived Benefits of HEID Services
Most of the mothers had high perceptions of the benefits of the uptake of HIV early infant to their HIV-exposed infants with a mean score of 4.3 out of five on the 5-level Likert scale with the five showing the higher perceived benefit. The high perceived benefit reported in this study might be because of the much effort put into reducing the barriers toward early infant HIV diagnosis services, such as HIV-related stigma, and the increase in the coverage of PMTCT/HEID services in the study settings. The findings are contrary to what was in Ethiopia where pregnant women perceived low net benefits (perceived benefits over the barrier) of the utilization of PMTCT-HIV testing. 20
In this study, the perceived benefit had no statistically significant association with the uptake of HIV early infant diagnosis. The findings differ from that of a study in Ethiopia in which low perceived benefits of PMTCT-HIV testing were negatively associated with utilization of PMTCT-HIV testing. 20
Limitation of the Study
This study has some limitations. Data for this study was collected from high-volume health facilities which are not representative of the low-volume health facilities. Therefore, this finding cannot be representative of the low-volume facilities in this area. Secondly, with the cross-sectional design applied, it might not be possible to draw a direct link between self-efficacy and HEID uptake in the study although the two appeared to be significantly associated, because they were all measured at the same time, it may not mean one caused the other. Nevertheless, the study provided useful insights into the predictors of mothers living with HIV uptake of HEID in the study settings. A prospective study looking at the issues of self-efficacy and HEID uptake would yield useful information to ascertain their causal relationship for better-targeted interventions.
Conclusion
The study found that over three-quarters of HIV-exposed infants had the uptake of the initial DNA-PCR testing within 6 weeks of life per the recommendations, though the rate is still lower than the national target of 95%. Mothers perceived self-efficacy on the uptake of HEID services was the main factor that influenced the high uptake of HEID, however, mothers’ perception of the risks and perception of the benefits of HEID uptake didn’t influence the uptake of the initial DNA-PCR HIV test. This calls for targeted efforts to increase perceived self-efficacy to HEID among mothers living with HIV to boost their uptake of HEID and accelerate reaching the national and global targets for HIV detection, prompt initiation of ART services and ultimately better health outcomes. Future studies should look prospectively at the effects of perceived self-efficacy and the benefits of EID on the uptake of the HEID.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
All raw data will be obtained from the appropriate authors upon reasonable request.